Trabeculectomy
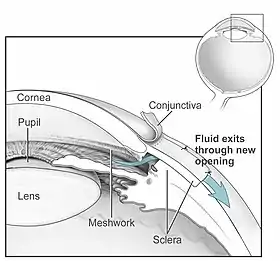
Trabeculectomy is a surgical procedure used in the treatment of glaucoma to relieve intraocular pressure by removing part of the eye's trabecular meshwork and adjacent structures. It is the most common glaucoma surgery performed and allows drainage of aqueous humor from within the eye to underneath the conjunctiva where it is absorbed. This outpatient procedure was most commonly performed under monitored anesthesia care using a retrobulbar block or peribulbar block or a combination of topical and subtenon (Tenon's capsule) anesthesia. Due to the higher risks associated with bulbar blocks, topical analgesia with mild sedation is becoming more common. Rarely general anesthesia will be used, in patients with an inability to cooperate during surgery.
| Trabeculectomy | |
|---|---|
 Trabeculectomy for treating glaucoma | |
| ICD-9-CM | 12.64 |
| MeSH | D014130 |
Procedure
An initial pocket is created under the conjunctiva and Tenon's capsule and the wound bed is treated for several seconds to minutes with mitomycin C (MMC, 0.5–0.2 mg/ml) or 5-fluorouracil (5-FU, 50 mg/ml) soaked sponges. These chemotherapeutics help to prevent failure of the filter bleb from scarring by inhibiting fibroblast proliferation. Alternatively, non-chemotherapeutic adjuvants can be implemented to prevent super scarring by wound modulation, such as the ologen collagen matrix implant.[1][2][3][4][5] Some surgeons prefer "fornix-based" conjunctival incisions while others use "limbus-based" construction at the corneoscleral junction which may allow easier access in eyes with deep sulci. A partial thickness flap with its base at the corneoscleral junction is then made in the sclera after careful cauterization of the flap area, and a window opening is created under the flap with a Kelly-punch to remove a portion of the sclera, Schlemm's canal and the trabecular meshwork to enter the anterior chamber. Because of the fluid egress the iris will partially prolapse through the sclerostomy and is usually therefore grasped to perform an excision called iridectomy. This iridectomy will prevent future blockage of the sclerostomy. The scleral flap is then sutured loosely back in place with several sutures. The conjunctiva is closed in a watertight fashion at the end of the procedure.
Mechanism
Intraocular pressure may be lowered by allowing drainage of aqueous humor from within the eye to the following routes: (1) filtration through the sclerotomy around the margins of the scleral flap into the filtering bleb that forms underneath the conjunctiva, (2) filtration through outlet channels in the scleral flap to underneath the conjunctiva,(3) Filtration through the connective tissue of the scleral flap to underneath the conjunctiva. Into cut ends of Schlemm's canal. (4) aqueous flow into cut ends of Schlemm's canal into collector channels and episcleral veins (5) into a cyclodialysis cleft between the ciliary body and the sclera if tissue is dissected posterior to the scleral spur.
Postoperative care
Glaucoma medications are usually discontinued to improve aqueous humor flow to the bleb. Topical medications consist typically of antibiotic drops four times per day and anti-inflammatory therapy e.g. with prednisolone drops every two hours. A shield is applied to cover the eye until anesthesia has worn off (that also anesthetizes the optic nerve) and vision resumes.
Patients are instructed to call immediately for pain that cannot be controlled with over the counter pain medication or if vision decreases, to not rub the eye and to wear the shield at night for several days after surgery.
If 5-FU was used during surgery or if no anti-fibrotic agent was applied, 5 mg 5-FU daily can be injected in the 7–14 postoperative days. In the following days to weeks sutures that hold the scleral flap down can be cut by laser suture lysis to titrate the intraocular pressure down by improving outflow. In laser suture lysis a red light laser and a contact lens are used to penetrate noninvasively the overlying conjunctiva and cut the black nylon suture. Some surgeons prefer adjustable flap sutures during the trabeculectomy that can be loosened later on with forceps in a slit lamp office procedure.
Postoperative challenges
- Flat bleb – will fail if not formed in first postoperative days; if early scarring is cause, subconjunctival 5-FU injections or wound modulation with ologen collagen matrix can prevent conjunctiva from adhering down the wound bed.
- Bleb leak – may cause flat bleb; leaking blebs can be revised with the use of ologen collagen matrix or bandage contact lens for several days followed by leak repair if necessary
- Flat anterior chamber – reform to prevent corneal decompensation; can often be done in the office at the slit lamp with viscoelastics used in cataract surgery
- Blebitis – if infectious can progress to devastating endophthalmitis
- Suprachoroidal hemorrhage – rupture of long posterior ciliary artery from progressive stretching with progressive serous choroidal detachment; usually occurs several days after trabeculectomy with acute pain often while straining
- Hypotony – wound revision[6]
- Cataract formation – cataract surgery if visually significant
- Small encapsulated bleb – injection of subconjunctival MMC and lidocaine can balloon up adjacent conjunctiva followed by needle incision of the bleb side and bleb extension; alternatively or together, the use of biodegradable spacer or ologen collagen matrix implant may be implemented.[7]
Conclusion
Trabeculectomy is the most common invasive glaucoma surgery. It is highly effective in the treatment of advanced glaucoma as demonstrated in major glaucoma studies. Even if a prior trabeculectomy has failed a second trabeculectomy can be performed at a different site. If scarring is the main reason, anti-fibrotic and anti-inflammatory therapy has to be intensified in the second procedure. Alternatively, insertion of a glaucoma valve device can be used.
Modifications of trabeculectomy
Trabeculectomy has undergone numerous modifications, e.g. filtering trepanotrabeculectomy (TTE) is a modification of the operation after J. Fronimopoulos. A triangular scleral flap is created which is approximately one-half as thick as the sclera. Trepanation is performed with a 2 mm trephine. The scleral edge of the trepanation opening is heat-cauterized.[8]
Additional deep scleral dissection can also be performed in the scleral bed with trabeculectomy, first introduced by T. Dada et al.;[9] deep scleral excision is performed in non-penetrating filtering surgeries but not traditionally in trabeculectomy. The space created from the deep scleral dissection is proposed to accommodate certain biocompatible spacer or devices in order to prevent subscleral fibrosis and to maintain good filtering results in this modified operation.
Various devices have been used with trabeculectomy techniques with the goal of improving safety of the procedure, maintaining drainage of aqueous humor, and to maintain the patency of bleb.[10] Examples of Trabeculectomy-modifying devices are Ex-PRESS, Gelfilm, XEN Gel stent, antifibrotic materials (e.g Ologen), ePTFE (expanded polytetrafluoroethylene) membrane and PreserFlo MicroShunt. Comparing each of these devices for effectiveness and safety is required.[10] There is some low low-quality evidence that usage of Ex-PRESS implant, a miniature stainless steel shunt, and human amniotic membrane as adjuncts with trabeculectomy have been associated with reduced intraocular pressure in patients after a one-year follow-up, compared to standard trabeculectomy.[10] In addition, the PreserFlo MicroShunt may help prevent complications such as postoperative hypotony or bleb leakage, however, this technique may have a lower effectiveness at reducing intraoculur pressure compared to a standard trabeculectomy procedures.[10]
Research
Further research is needed to compare the effectiveness of trabeculectomy techniques. It is not clear if a fornix-based surgical approach has a different safety rating, complication rate, surgical failure rate, or effectiveness compared to a limbal-based conjunctival flaps technique.[11]
Currently, there are no published trials which compare the efficacy and safety of ab interno trabeculectomy with Trabectome with other procedures for treating glaucoma.[12] The first trial to do so is the TAGS randomised controlled trial which investigated if eye drops or trabeculectomy is more effective in treating advanced primary open-angle glaucoma. After two years researchers found that vision and quality of life are similar in both treatments. At the same time eye pressure was lower in people who underwent surgery and in the long-run surgery is more cost-effective.[13][14]
History
Peter Gordon Watson and John Cairns developed the trabeculectomy procedure in the 1970s.[15]
See also
References
- Cillino, S; Pace F Di; Cillino G; Casuccio A (Sep 2011). "Biodegradable collagen matrix implant vs mitomycin-C as an adjuvant in trabeculectomy: a 24-month, randomized clinical trial". Eye. 25 (12): 1598–606. doi:10.1038/eye.2011.219. PMC 3234465. PMID 21921953.
- Marey, H M; S S Mandour; A F Ellakwa (Oct 2012). "Subscleral Trabeculectomy with Mitomycin-C Versus Ologen for Treatment of Glaucoma". Journal of Ocular Pharmacology and Therapeutics. 29 (3): 330–34. doi:10.1089/jop.2012.0120. PMID 23113645.
- Papaconstantinou, Dimitris; Georgalas I; Karmiris E; Diagourtas A; Koutsandrea C; Ladas I; Apostolopoulos M; Georgopoulos G (Feb 2010). "Trabeculectomy with ologen versus trabeculectomy for the treatment of glaucoma: a pilot study". Acta Ophthalmol. 88 (1): 80–85. doi:10.1111/j.1755-3768.2009.01753.x. PMID 19900209.
- Rosentreter, Andre; Schild AM; Jordan JF; Krieglstein GK; Dietlein TS (Sep 2010). "A prospective randomised trial of trabeculectomy using mitomycin C vs an ologen implant in open angle glaucoma". Eye. 24 (9): 1449–57. doi:10.1038/eye.2010.106. PMID 20733558.
- Nilforushan, Naveed; Yadgari M; Falavarjani KG; Afshar AE (2010). "Evaluation of subconjunctival Oculusgen* implantation as an adjunct to trabeculectomy". Iranian J Ophthalmol. 22 (2): 55–62. Retrieved 3 November 2011.
- Dietlein TS, Rosentreter A. "Secondary subconjunctival implantation of biodegradable porous collagen matrix for treating ocular hypotony following trabeculectomy with mitomycin C" (PDF). 2012 EGS Congress, Copenhagen. Retrieved 20 December 2012.
- Kouros P, Loesche CC, Sbeity Z, Palmiero PM. "Ologen implants as an adjuvant for revision surgery after failed trabeculectomy" (PDF). 2012 EGS Congress, Copenhagen. Retrieved 20 December 2012.
- Sjarov N, Draganska A (July 1984). "[Filtering trepano-trabeculectomy with sponge-like scar]". Klin Monbl Augenheilkd (in German). 185 (1): 55–58. doi:10.1055/s-2008-1054571. PMID 6482288.
- Tanuj, D; Amit S; Saptorshi M; Meenakshi G (May 2013). "Combined Subconjunctival and Subscleral Ologen Implant Insertion In Trabeculectomy". Eye. 27 (7): 889. doi:10.1038/eye.2013.76. PMC 3709396. PMID 23640614.
- Park, Junghyun; Rittiphairoj, Thanitsara; Wang, Xue; E, Jian-Yu; Bicket, Amanda K. (2023-03-13). "Device-modified trabeculectomy for glaucoma". The Cochrane Database of Systematic Reviews. 3 (3): CD010472. doi:10.1002/14651858.CD010472.pub3. ISSN 1469-493X. PMC 10010250. PMID 36912740.
- Theventhiran, Alex B.; Kim, Gene; Yao, WenJeng (2021-08-26). "Fornix-based versus limbal-based conjunctival trabeculectomy flaps for glaucoma". The Cochrane Database of Systematic Reviews. 2021 (8): CD009380. doi:10.1002/14651858.CD009380.pub3. ISSN 1469-493X. PMC 8407098. PMID 34437715.
- Hu, Kuang; Shah, Anupa; Virgili, Gianni; Bunce, Catey; Gazzard, Gus (2021-02-04). "Ab interno trabecular bypass surgery with Trabectome for open-angle glaucoma". The Cochrane Database of Systematic Reviews. 2021 (2): CD011693. doi:10.1002/14651858.CD011693.pub3. ISSN 1469-493X. PMC 8094917. PMID 33580495.
- "Advanced glaucoma: surgery lowers pressure in the eye more effectively than eye drops". NIHR Evidence (Plain English summary). National Institute for Health and Care Research. 2022-03-31. doi:10.3310/alert_49606. S2CID 247918434.
- King, Anthony J; Fernie, Gordon; Hudson, Jemma; Kernohan, Ashleigh; Azuara-Blanco, Augusto; Burr, Jennifer; Homer, Tara; Shabaninejad, Hosein; Sparrow, John M; Garway-Heath, David; Barton, Keith; Norrie, John; McDonald, Alison; Vale, Luke; MacLennan, Graeme (December 2021). "Primary trabeculectomy versus primary glaucoma eye drops for newly diagnosed advanced glaucoma: TAGS RCT". Health Technology Assessment. 25 (72): 1–158. doi:10.3310/hta25720. ISSN 1366-5278. PMID 34854808.
- "Peter Watson, FRCOphth 1931 – 2017" (PDF).