Bacterial vaginosis
Bacterial vaginosis (BV) is an infection of the vagina caused by excessive growth of bacteria.[6][9] Common symptoms include increased vaginal discharge that often smells like fish.[2] The discharge is usually white or gray in color.[2] Burning with urination may occur.[2] Itching is uncommon.[2][6] Occasionally, there may be no symptoms.[2] Having BV approximately doubles the risk of infection by a number of sexually transmitted infections, including HIV/AIDS.[8][10] It also increases the risk of early delivery among pregnant women.[3][11]
| Bacterial vaginosis | |
|---|---|
| Other names | Anaerobic vaginositis, non-specific vaginitis, vaginal bacteriosis, Gardnerella vaginitis[1] |
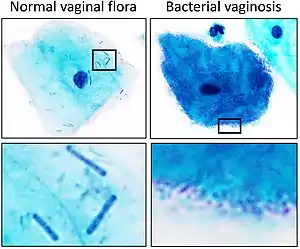 | |
| Vaginal squamous cell with normal vaginal flora versus bacterial vaginosis on Pap stain. Normal vaginal flora (left) is predominantly rod-shaped Lactobacilli whereas in bacterial vaginosis (right) there is an overgrowth of bacteria which can be of multiple species. | |
| Specialty | Gynecology, Infectious disease |
| Symptoms | Vaginal discharge that often smells like fish, burning with urination[2] |
| Complications | Early delivery among pregnant women[3] |
| Causes | Imbalance of the naturally occurring bacteria in the vagina[4][5] |
| Risk factors | Douching, new or multiple sex partners, antibiotics, using an intrauterine device[5] |
| Diagnostic method | Testing the vaginal discharge[6] |
| Differential diagnosis | Vaginal yeast infection, infection with Trichomonas[7] |
| Prevention | Probiotics[6] |
| Medication | Clindamycin or metronidazole[6] |
| Frequency | ~ 5% to 70% of women[8] |
BV is caused by an imbalance of the naturally occurring bacteria in the vagina.[4][5] There is a change in the most common type of bacteria and a hundred to thousand fold increase in total numbers of bacteria present.[6] Typically, bacteria other than Lactobacilli become more common.[12] Risk factors include douching, new or multiple sex partners, antibiotics, and using an intrauterine device, among others.[5] However, it is not considered a sexually transmitted infection and, unlike gonorrhoea and chlamydia, sexual partners are not treated.[13] Diagnosis is suspected based on the symptoms, and may be verified by testing the vaginal discharge and finding a higher than normal vaginal pH, and large numbers of bacteria.[6] BV is often confused with a vaginal yeast infection or infection with Trichomonas.[7]
Usually treatment is with an antibiotic, such as clindamycin or metronidazole.[6] These medications may also be used in the second or third trimesters of pregnancy.[6] However, the condition often recurs following treatment.[6] Probiotics may help prevent re-occurrence.[6] It is unclear if the use of probiotics or antibiotics affects pregnancy outcomes.[6][14]
BV is the most common vaginal infection in women of reproductive age.[5] The percentage of women affected at any given time varies between 5% and 70%.[8] BV is most common in parts of Africa and least common in Asia and Europe.[8] In the United States about 30% of women between the ages of 14 and 49 are affected.[15] Rates vary considerably between ethnic groups within a country.[8] While BV-like symptoms have been described for much of recorded history, the first clearly documented case occurred in 1894.[1]
Signs and symptoms
Although about 50% of women with BV are asymptomatic,[16] common symptoms include increased vaginal discharge that usually smells like fish. The discharge is often white or gray in color. There may be burning with urination. Occasionally, there may be no symptoms.[2]
The discharge coats the walls of the vagina, and is usually without significant irritation, pain, or erythema (redness), although mild itching can sometimes occur. By contrast, the normal vaginal discharge will vary in consistency and amount throughout the menstrual cycle and is at its clearest at ovulation—about two weeks before the period starts. Some practitioners claim that BV can be asymptomatic in almost half of affected women,[17] though others argue that this is often a misdiagnosis.[18]
Complications
Although previously considered a mere nuisance infection, untreated bacterial vaginosis may cause increased susceptibility to sexually transmitted infections, including HIV, and pregnancy complications.[19][20]
It has been shown that HIV-infected women with bacterial vaginosis (BV) are more likely to transmit HIV to their sexual partners than those without BV.[10] There is evidence of an association between BV and increased rates of sexually transmitted infections such as HIV/AIDS.[19] BV is associated with up to a six-fold increase in HIV shedding. BV is a risk factor for viral shedding and herpes simplex virus type 2 infection. BV may increase the risk of infection with or reactivation of human papillomavirus (HPV).[19][21]
In addition, bacterial vaginosis as either pre-existing, or acquired, may increase the risk of pregnancy complications, most notably premature birth or miscarriage.[22][23] Pregnant women with BV have a higher risk of chorioamnionitis, miscarriage, preterm birth, premature rupture of membranes, and postpartum endometritis.[24] Women with BV who are treated with in vitro fertilization have a lower implantation rate and higher rates of early pregnancy loss.[19][21]
Causes
Healthy vaginal microbiota consists of species that neither cause symptoms or infections, nor negatively affect pregnancy. It is dominated mainly by Lactobacillus species.[12][25] BV is defined by the disequilibrium in the vaginal microbiota, with decline in the number of lactobacilli. While the infection involves a number of bacteria, it is believed that most infections start with Gardnerella vaginalis creating a biofilm, which allows other opportunistic bacteria, such as Prevotella and Bacteroides, to thrive.[26][9][27]
One of the main risks for developing BV is douching, which alters the vaginal microbiota and predisposes women to developing BV.[28] Douching is strongly discouraged by the U.S. Department of Health and Human Services and various medical authorities, for this and other reasons.[28]
BV is a risk factor for pelvic inflammatory disease, HIV, sexually transmitted infections (STIs), endometriosis, and reproductive and obstetric disorders or negative outcomes. Although BV can be associated with sexual activity, there is no clear evidence of sexual transmission.[26][29][30] It is possible for sexually inactive persons to develop bacterial vaginosis.[29][9]
Also, subclinical iron deficiency may correlate with bacterial vaginosis in early pregnancy.[31] A longitudinal study published in February 2006, in the American Journal of Obstetrics and Gynecology, showed a link between psychosocial stress and bacterial vaginosis persisted even when other risk factors were taken into account.[32] Exposure to the spermicide nonoxynol-9 does not affect the risk of developing bacterial vaginosis.[33]
Diagnosis
To make a diagnosis of bacterial vaginosis, a swab from inside the vagina should be obtained. These swabs can be tested for:
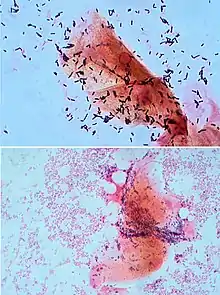
- Gram stain which shows the depletion of lactobacilli and overgrowth of Gardnerella vaginalis bacteria. Bacterial vaginosis is usually confirmed by a Gram stain of vaginal secretions.[34]
- A characteristic "fishy" odor on wet mount. This test, called the whiff test, is performed by adding a small amount of potassium hydroxide to a microscope slide containing the vaginal discharge. A characteristic fishy odor is considered a positive whiff test and is suggestive of bacterial vaginosis.
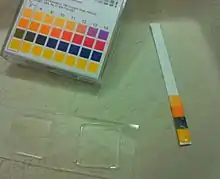
- Loss of acidity. To control bacterial growth, the vagina is normally slightly acidic with a pH of 3.8–4.2. A swab of the discharge is put onto litmus paper to check its acidity. A pH greater than 4.5 is considered alkaline and is suggestive of bacterial vaginosis.
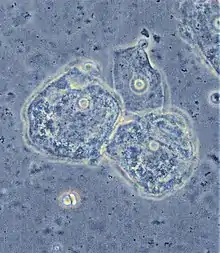
- The presence of clue cells on wet mount. Similar to the whiff test, the test for clue cells is performed by placing a drop of sodium chloride solution on a slide containing vaginal discharge. If present, clue cells can be visualized under a microscope. They are so-named because they give a clue to the reason behind the discharge. These are epithelial cells that are coated with bacteria.
Differential diagnosis for bacterial vaginosis includes the following:[35]
- Normal vaginal discharge.
- Candidiasis (thrush, or a yeast infection).
- Trichomoniasis, an infection caused by Trichomonas vaginalis.
- Aerobic vaginitis[36]
The Center for Disease Control (CDC) defines STIs as "a variety of clinical syndromes and infections caused by pathogens that can be acquired and transmitted through sexual activity."[37] But the CDC does not specifically identify BV as sexually transmitted infection.[13]
Amsel criteria
In clinical practice BV can be diagnosed using the Amsel criteria:[38]
- Thin, white, yellow, homogeneous discharge
- Clue cells on microscopy
- pH of vaginal fluid >4.5
- Release of a fishy odor on adding alkali—10% potassium hydroxide (KOH) solution.
At least three of the four criteria should be present for a confirmed diagnosis.[39] A modification of the Amsel criteria accepts the presence of two instead of three factors and is considered equally diagnostic.[40]
Gram stain
An alternative is to use a Gram-stained vaginal smear, with the Hay/Ison[41] criteria or the Nugent[24] criteria. The Hay/Ison criteria are defined as follows:[39]
- Grade 1 (Normal): Lactobacillus morphotypes predominate.
- Grade 2 (Intermediate): Some lactobacilli present, but Gardnerella or Mobiluncus morphotypes also present.
- Grade 3 (Bacterial Vaginosis): Predominantly Gardnerella and/or Mobiluncus morphotypes. Few or absent lactobacilli. (Hay et al., 1994)
Gardnerella vaginalis is the main culprit in BV. Gardnerella vaginalis is a short, Gram-variable rod (coccobacillus). Hence, the presence of clue cells and gram variable coccobacilli are indicative or diagnostic of bacterial vaginosis.[42]
Nugent score
The Nugent score is now rarely used by physicians due to the time it takes to read the slides and requires the use of a trained microscopist.[4] A score of 0-10 is generated from combining three other scores. The scores are as follows:[24]
- 0–3 is considered negative for BV
- 4–6 is considered intermediate
- 7+ is considered indicative of BV.
At least 10–20 high power (1000× oil immersion) fields are counted and an average determined.[43]
|
Lactobacillus morphotypes – average per high powered (1000× oil immersion) field. View multiple fields. |
Gardnerella / Bacteroides morphotypes – average per high powered (1000× oil immersion) field. View multiple fields. |
Curved Gram variable rods – average per high powered (1000× oil immersion) field. View multiple fields (note that this factor is less important – scores of only 0–2 are possible) |
|
|
|
DNA hybridization testing with Affirm VPIII was compared to the Gram stain using the Nugent criteria.[44] The Affirm VPIII test may be used for the rapid diagnosis of BV in symptomatic women but uses expensive proprietary equipment to read results, and does not detect other pathogens that cause BV, including Prevotella spp, Bacteroides spp, and Mobiluncus spp.[45] The cervicovaginal microbiome measured using 16S rRNA sequencing has the capacity to increase throughput of the Nugent Score and has demonstrate to be directly comparable to clinical Nugent Score measurement.[46]
Screening
Screening during pregnancy is not recommended in the United States as of 2020 because " the US Preventive Services Task Force concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for bacterial vaginosis in pregnant persons at increased risk for preterm delivery".[47]
Prevention
Some steps suggested to lower the risk include: not douching, avoiding sex, or limiting the number of sex partners.[48]
One review concluded that probiotics may help prevent re-occurrence.[6] Another review found that, while there is tentative evidence, it is not strong enough to recommend their use for this purpose.[49]
Early evidence suggested that antibiotic treatment of male partners could re-establish the normal microbiota of the male urogenital tract and prevent the recurrence of infection.[19] However, a 2016 Cochrane review found high-quality evidence that treating the sexual partners of women with bacterial vaginosis had no effect on symptoms, clinical outcomes, or recurrence in the affected women. It also found that such treatment may lead treated sexual partners to report increased adverse events.[19]
Treatment
Antibiotics
Treatment is typically with the antibiotics metronidazole or clindamycin.[50] They can be either given by mouth or applied inside the vagina with similar efficacy.[16][50] About 10% to 15% of people, however, do not improve with the first course of antibiotics and recurrence rates of up to 80% have been documented.[21] Recurrence rates are increased with sexual activity with the same pre-/posttreatment partner and inconsistent condom use although estrogen-containing contraceptives decrease recurrence.[51] When clindamycin is given to pregnant women symptomatic with BV before 22 weeks of gestation the risk of pre-term birth before 37 weeks of gestation is lower.[52]
Other antibiotics that may work include macrolides, lincosamides, nitroimidazoles, and penicillins.[19]
Bacterial vaginosis is not considered a sexually transmitted infection, and treatment of a male sexual partner of a woman with bacterial vaginosis is not recommended.[53][54]
Probiotics
A 2009 Cochrane review found tentative but insufficient evidence for probiotics as a treatment for BV.[21] A 2014 review reached the same conclusion.[55] A 2013 review found some evidence supporting the use of probiotics during pregnancy.[56] The preferred probiotics for BV are those containing high doses of lactobacilli (around 109 CFUsTooltip Colony-forming units) given in the vagina.[57] Intravaginal administration is preferred to taking them by mouth.[57] Prolonged repetitive courses of treatment appear to be more promising than short courses.[57]
The lack of effectiveness of commercially available Lactobacillus probiotics may be because most do not actually contain vaginal lactobacilli strains.[58] LACTIN-V is a live biopharmaceutical medication containing the vaginally important Lactobacillus crispatus which is under development for the treatment of bacterial vaginosis and recurrent urinary tract infections.[58][59][60] It has shown initial effectiveness in considerably reducing recurrence of bacterial vaginosis following antibiotic treatment.[58][60] LACTIN-V is not yet Food and Drug Administration (FDA)-approved or commercially available.[60][59]
Antiseptics
Topical antiseptics, for example dequalinium chloride, policresulen, hexetidine or povidone-iodine vaginal suppositories may be applied, if the risk of ascending infections is low (outside of pregnancy and in immunocompetent people without histories of upper genital tract infections).[61] One study found that vaginal irrigations with hydrogen peroxide (3%) resulted in a slight improvement but this was much less than with the use of oral metronidazole.[62] Intravaginal boric acid in conjunction with other medications may be helpful in the treatment of recurrent BV.[60][63] TOL-463, a formulation of boric acid enhanced with ethylenediaminetetraacetic acid (EDTA), is under development as an intravaginal medication for the treatment of BV and has shown preliminary effectiveness.[64][63][65][66]
Epidemiology
BV is the most common infection of the vagina in women of reproductive age.[5] The percentage of women affected at any given time varies between 5% and 70%.[8] BV is most common in parts of Africa, and least common in Asia and Europe.[8] In the United States, about 30% of those between the ages of 14 and 49 are affected.[15] Rates vary considerably between ethnic groups within a country.[8]
References
- Borchardt KA (1997). Sexually transmitted diseases: epidemiology, pathology, diagnosis, and treatment. Boca Raton [u.a.]: CRC Press. p. 4. ISBN 9780849394768. Archived from the original on 10 September 2017.
- "What are the symptoms of bacterial vaginosis?". 21 May 2013. Archived from the original on 2 April 2015. Retrieved 3 March 2015.
- Queena JT, Spong CY, Lockwood CJ, eds. (2012). Queenan's management of high-risk pregnancy: an evidence-based approach (6th ed.). Chichester, West Sussex: Willey-Blackwell. p. 262. ISBN 9780470655764.
- Bennett J (2015). Mandell, Douglas, and Bennett's principles and practice of infectious diseases. Philadelphia, PA: Elsevier/Saunders. ISBN 9781455748013.
- "Bacterial Vaginosis (BV): Condition Information". National Institute of Child Health and Human Development. 21 May 2013. Archived from the original on 2 April 2015. Retrieved 3 March 2015.
- Donders GG, Zodzika J, Rezeberga D (April 2014). "Treatment of bacterial vaginosis: what we have and what we miss". Expert Opinion on Pharmacotherapy. 15 (5): 645–57. doi:10.1517/14656566.2014.881800. PMID 24579850. S2CID 19241611.
- Mashburn J (2006). "Etiology, diagnosis, and management of vaginitis". Journal of Midwifery & Women's Health. 51 (6): 423–30. doi:10.1016/j.jmwh.2006.07.005. PMID 17081932.
- Kenyon C, Colebunders R, Crucitti T (December 2013). "The global epidemiology of bacterial vaginosis: a systematic review". American Journal of Obstetrics and Gynecology. 209 (6): 505–23. doi:10.1016/j.ajog.2013.05.006. PMID 23659989.
- Sharma H, Tal R, Clark NA, Segars JH (January 2014). "Microbiota and pelvic inflammatory disease". Seminars in Reproductive Medicine. 32 (1): 43–9. doi:10.1055/s-0033-1361822. PMC 4148456. PMID 24390920.
- Bradshaw CS, Brotman RM (July 2015). "Making inroads into improving treatment of bacterial vaginosis - striving for long-term cure". BMC Infectious Diseases. 15: 292. doi:10.1186/s12879-015-1027-4. PMC 4518586. PMID 26219949.
- "What are the treatments for bacterial vaginosis (BV)?". National Institute of Child Health and Human Development. 15 July 2013. Archived from the original on 2 April 2015. Retrieved 4 March 2015.
- Nardis C, Mosca L, Mastromarino P (September–October 2013). "Vaginal microbiota and viral sexually transmitted diseases". Annali di Igiene. 25 (5): 443–56. doi:10.7416/ai.2013.1946. PMID 24048183.
- "Bacterial Vaginosis – CDC Fact Sheet". Centers for Disease Control and Prevention. 11 March 2014. Archived from the original on 28 February 2015. Retrieved 2 March 2015.
- Othman M, Neilson JP, Alfirevic Z (January 2007). "Probiotics for preventing preterm labour". The Cochrane Database of Systematic Reviews. 2012 (1): CD005941. doi:10.1002/14651858.CD005941.pub2. PMC 9006117. PMID 17253567.
- "Bacterial Vaginosis (BV) Statistics Prevalence". cdc.gov. 14 September 2010. Archived from the original on 22 February 2015. Retrieved 3 March 2015.
- Tidbury FD, Langhart A, Weidlinger S, Stute P (January 2021). "Non-antibiotic treatment of bacterial vaginosis-a systematic review". Archives of Gynecology and Obstetrics. 303 (1): 37–45. doi:10.1007/s00404-020-05821-x. PMID 33025086. S2CID 222149236.
- Schwebke JR (December 2000). "Asymptomatic bacterial vaginosis: response to therapy". American Journal of Obstetrics and Gynecology. 183 (6): 1434–9. doi:10.1067/mob.2000.107735. PMID 11120507.
- Forney LJ, Foster JA, Ledger W (November 2006). "The vaginal flora of healthy women is not always dominated by Lactobacillus species". The Journal of Infectious Diseases. 194 (10): 1468–9, author reply 1469–70. doi:10.1086/508497. PMID 17054080.
- Amaya-Guio J, Viveros-Carreño DA, Sierra-Barrios EM, Martinez-Velasquez MY, Grillo-Ardila CF (October 2016). "Antibiotic treatment for the sexual partners of women with bacterial vaginosis". The Cochrane Database of Systematic Reviews. 2016 (10): CD011701. doi:10.1002/14651858.CD011701.pub2. PMC 6458027. PMID 27696372.
- "STD Facts — Bacterial Vaginosis (BV)". CDC. Archived from the original on 3 December 2007. Retrieved 4 December 2007.
- Senok AC, Verstraelen H, Temmerman M, Botta GA (October 2009). "Probiotics for the treatment of bacterial vaginosis". The Cochrane Database of Systematic Reviews (4): CD006289. doi:10.1002/14651858.CD006289.pub2. PMID 19821358.
- "Bacterial vaginosis". National Health Service, UK. Archived from the original on 9 February 2014. Retrieved 3 October 2013.
- Hillier SL, Nugent RP, Eschenbach DA, Krohn MA, Gibbs RS, Martin DH, et al. (December 1995). "Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group". The New England Journal of Medicine. 333 (26): 1737–42. doi:10.1056/NEJM199512283332604. PMID 7491137.
- Nugent RP, Krohn MA, Hillier SL (February 1991). "Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation". Journal of Clinical Microbiology. 29 (2): 297–301. doi:10.1128/JCM.29.2.297-301.1991. PMC 269757. PMID 1706728.
- Petrova MI, Lievens E, Malik S, Imholz N, Lebeer S (2015). "Lactobacillus species as biomarkers and agents that can promote various aspects of vaginal health". Frontiers in Physiology. 6: 81. doi:10.3389/fphys.2015.00081. PMC 4373506. PMID 25859220.
- Jiang I, Yong PJ, Allaire C, Bedaiwy MA (May 2021). "Intricate Connections between the Microbiota and Endometriosis". International Journal of Molecular Sciences. 22 (11): 5644. doi:10.3390/ijms22115644. PMC 8198999. PMID 34073257.
- Patterson JL, Stull-Lane A, Girerd PH, Jefferson KK (February 2010). "Analysis of adherence, biofilm formation and cytotoxicity suggests a greater virulence potential of Gardnerella vaginalis relative to other bacterial-vaginosis-associated anaerobes". Microbiology. 156 (Pt 2): 392–399. doi:10.1099/mic.0.034280-0. PMC 2890091. PMID 19910411.
- Cottrell BH (2010). "An updated review of evidence to discourage douching". MCN: The American Journal of Maternal/Child Nursing. 35 (2): 102–7, quiz 108–9. doi:10.1097/NMC.0b013e3181cae9da. PMID 20215951. S2CID 46715131.
- Ali A, Jørgensen JS, Lamont RF (2022). "The contribution of bacteriophages to the aetiology and treatment of the bacterial vaginosis syndrome". Faculty Reviews. 11: 8. doi:10.12703/r/11-8. PMC 9022730. PMID 35509673.
- Bradshaw CS, Morton AN, Hocking J, Garland SM, Morris MB, Moss LM, Horvath LB, Kuzevska I, Fairley CK (2006). "High recurrence rates of bacterial vaginosis over the course of 12 months after oral metronidazole therapy and factors associated with recurrence". J. Infect. Dis. 193 (11): 1478–86. doi:10.1086/503780. PMID 16652274. S2CID 24440932.
- Verstraelen H, Delanghe J, Roelens K, Blot S, Claeys G, Temmerman M (July 2005). "Subclinical iron deficiency is a strong predictor of bacterial vaginosis in early pregnancy". BMC Infectious Diseases. 5 (1): 55. doi:10.1186/1471-2334-5-55. PMC 1199597. PMID 16000177.
- Nansel TR, Riggs MA, Yu KF, Andrews WW, Schwebke JR, Klebanoff MA (February 2006). "The association of psychosocial stress and bacterial vaginosis in a longitudinal cohort". American Journal of Obstetrics and Gynecology. 194 (2): 381–6. doi:10.1016/j.ajog.2005.07.047. PMC 2367104. PMID 16458633.
- Wilkinson D, Ramjee G, Tholandi M, Rutherford G (2002). "Nonoxynol-9 for preventing vaginal acquisition of sexually transmitted infections by women from men". The Cochrane Database of Systematic Reviews (4): CD003939. doi:10.1002/14651858.CD003939. PMID 12519623.
- Muzny CA, Kardas P (July 2020). "A Narrative Review of Current Challenges in the Diagnosis and Management of Bacterial Vaginosis". Sexually Transmitted Diseases. 47 (7): 441–446. doi:10.1097/OLQ.0000000000001178. PMC 7294746. PMID 32235174.
- "Diseases Characterized by Vaginal Discharge". cdc.gov. Centers for Disease Control and Prevention. Archived from the original on 11 July 2017.
- Donders GG, Vereecken A, Bosmans E, Dekeersmaecker A, Salembier G, Spitz B (January 2002). "Definition of a type of abnormal vaginal flora that is distinct from bacterial vaginosis: aerobic vaginitis". BJOG. 109 (1): 34–43. doi:10.1111/j.1471-0528.2002.00432.x. hdl:10067/1033820151162165141. PMID 11845812. S2CID 8304009.
- Workowski KA, Bolan GA (June 2015). "Sexually transmitted diseases treatment guidelines, 2015". MMWR. Recommendations and Reports. 64 (RR-03): 1–137. PMC 5885289. PMID 26042815.
- Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK (January 1983). "Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations". The American Journal of Medicine. 74 (1): 14–22. doi:10.1016/0002-9343(83)91112-9. PMID 6600371.
- "National guideline for the management of bacterial vaginosis (2006)". Clinical Effectiveness Group, British Association for Sexual Health and HIV (BASHH). Archived from the original on 3 November 2008. Retrieved 16 August 2008.
- Mittal V, Jain A, Pradeep Y (May 2012). "Development of modified diagnostic criteria for bacterial vaginosis at peripheral health centres in developing countries". Journal of Infection in Developing Countries. 6 (5): 373–377. doi:10.3855/jidc.1625. PMID 22610702.
- Ison CA, Hay PE (December 2002). "Validation of a simplified grading of Gram stained vaginal smears for use in genitourinary medicine clinics". Sexually Transmitted Infections. 78 (6): 413–5. doi:10.1136/sti.78.6.413. PMC 1758337. PMID 12473800.
- Paladine, H. L.; Desai, U. A. (2018). "Vaginitis: Diagnosis and Treatment". American Family Physician. 97 (5): 321–329. PMID 29671516.
- Kamga YM, Ngunde JP, Akoachere JK (May 2019). "Prevalence of bacterial vaginosis and associated risk factors in pregnant women receiving antenatal care at the Kumba Health District (KHD), Cameroon". BMC Pregnancy and Childbirth. 19 (1): 166. doi:10.1186/s12884-019-2312-9. PMC 6511194. PMID 31077161.
- Gazi H, Degerli K, Kurt O, Teker A, Uyar Y, Caglar H, et al. (November 2006). "Use of DNA hybridization test for diagnosing bacterial vaginosis in women with symptoms suggestive of infection". APMIS. 114 (11): 784–787. doi:10.1111/j.1600-0463.2006.apm_485.x. PMID 17078859. S2CID 36677972.
- Brown HL, Fuller DD, Jasper LT, Davis TE, Wright JD (2004). "Clinical evaluation of affirm VPIII in the detection and identification of Trichomonas vaginalis, Gardnerella vaginalis, and Candida species in vaginitis/vaginosis". Infectious Diseases in Obstetrics and Gynecology. 12 (1): 17–21. doi:10.1080/1064744042000210375. PMC 1784585. PMID 15460191.
- Usyk M, Schlecht NF, Pickering S, Williams L, Sollecito CC, Gradissimo A, et al. (January 2022). "molBV reveals immune landscape of bacterial vaginosis and predicts human papillomavirus infection natural history". Nature Communications. 13 (1): 233. Bibcode:2022NatCo..13..233U. doi:10.1038/s41467-021-27628-3. PMC 8752746. PMID 35017496.
- Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, Caughey AB, et al. (April 2020). "Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery: US Preventive Services Task Force Recommendation Statement". JAMA. 323 (13): 1286–1292. doi:10.1001/jama.2020.2684. PMID 32259236. S2CID 215408782.
- "Bacterial Vaginosis – CDC Fact Sheet". Centers for Disease Control and Prevention. 11 March 2014. Archived from the original on 7 May 2015. Retrieved 6 May 2015.
- Mastromarino P, Vitali B, Mosca L (July 2013). "Bacterial vaginosis: a review on clinical trials with probiotics" (PDF). The New Microbiologica. 36 (3): 229–38. PMID 23912864. Archived (PDF) from the original on 18 May 2015.
- Oduyebo OO, Anorlu RI, Ogunsola FT (July 2009). Oduyebo OO (ed.). "The effects of antimicrobial therapy on bacterial vaginosis in non-pregnant women". The Cochrane Database of Systematic Reviews (3): CD006055. doi:10.1002/14651858.CD006055.pub2. PMID 19588379.
- Bradshaw CS, Vodstrcil LA, Hocking JS, Law M, Pirotta M, Garland SM, et al. (March 2013). "Recurrence of bacterial vaginosis is significantly associated with posttreatment sexual activities and hormonal contraceptive use". Clinical Infectious Diseases. 56 (6): 777–86. doi:10.1093/cid/cis1030. PMID 23243173.
- Lamont RF, Nhan-Chang CL, Sobel JD, Workowski K, Conde-Agudelo A, Romero R (September 2011). "Treatment of abnormal vaginal flora in early pregnancy with clindamycin for the prevention of spontaneous preterm birth: a systematic review and metaanalysis". American Journal of Obstetrics and Gynecology. 205 (3): 177–90. doi:10.1016/j.ajog.2011.03.047. PMC 3217181. PMID 22071048.
- Mehta SD (October 2012). "Systematic review of randomized trials of treatment of male sexual partners for improved bacteria vaginosis outcomes in women". Sexually Transmitted Diseases. 39 (10): 822–30. doi:10.1097/OLQ.0b013e3182631d89. PMID 23007709. S2CID 36148239.
- Potter J (November 1999). "Should sexual partners of women with bacterial vaginosis receive treatment?". The British Journal of General Practice. 49 (448): 913–8. PMC 1313567. PMID 10818662.
- Huang H, Song L, Zhao W (June 2014). "Effects of probiotics for the treatment of bacterial vaginosis in adult women: a meta-analysis of randomized clinical trials". Archives of Gynecology and Obstetrics. 289 (6): 1225–34. doi:10.1007/s00404-013-3117-0. PMID 24318276. S2CID 9696920.
- VandeVusse L, Hanson L, Safdar N (2013). "Perinatal outcomes of prenatal probiotic and prebiotic administration: an integrative review". The Journal of Perinatal & Neonatal Nursing. 27 (4): 288–301, quiz E1-2. doi:10.1097/jpn.0b013e3182a1e15d. PMID 24164813. S2CID 205728750.
- Mastromarino P, Vitali B, Mosca L (July 2013). "Bacterial vaginosis: a review on clinical trials with probiotics". The New Microbiologica. 36 (3): 229–38. PMID 23912864.
- Lagenaur LA, Hemmerling A, Chiu C, Miller S, Lee PP, Cohen CR, Parks TP (June 2021). "Connecting the Dots: Translating the Vaginal Microbiome Into a Drug". J Infect Dis. 223 (12 Suppl 2): S296–S306. doi:10.1093/infdis/jiaa676. PMC 8502429. PMID 33330916.
- "CTV 05". AdisInsight. Springer Nature Switzerland AG.
- "Bacterial Vaginosis - STI Treatment Guidelines". Centers for Disease Control and Prevention. 19 July 2021.
- Schaefer C, Spielmann H, Vetter K, eds. (January 2006). "Spezielle Arzneimitteltherapie in der Schwangerschaft" [Special medicamentous therapies in pregnancy]. Arzneiverordnung in Schwangerschaft und Stillzeit (in German) (7th ed.). Urban & Fischer. pp. 33–557. doi:10.1016/B978-343721332-8.50004-1. ISBN 978-3-437-21332-8. PMC 7271219.
- Verstraelen H, Verhelst R, Roelens K, Temmerman M (June 2012). "Antiseptics and disinfectants for the treatment of bacterial vaginosis: a systematic review". BMC Infectious Diseases. 12: 148. doi:10.1186/1471-2334-12-148. PMC 3458956. PMID 22742642.
- Sobel JD (28 November 2022). Marrazzo J, Barbieri RL, Eckler K (eds.). "Bacterial vaginosis: Initial treatment". UpToDate.
- "TOL 463". AdisInsight. Springer Nature Switzerland AG.
- Sobel JD, Sobel R (August 2021). "Current and emerging pharmacotherapy for recurrent bacterial vaginosis". Expert Opin Pharmacother. 22 (12): 1593–1600. doi:10.1080/14656566.2021.1904890. PMID 33750246. S2CID 232325625.
- Marrazzo JM, Dombrowski JC, Wierzbicki MR, Perlowski C, Pontius A, Dithmer D, Schwebke J (February 2019). "Safety and Efficacy of a Novel Vaginal Anti-infective, TOL-463, in the Treatment of Bacterial Vaginosis and Vulvovaginal Candidiasis: A Randomized, Single-blind, Phase 2, Controlled Trial". Clin Infect Dis. 68 (5): 803–809. doi:10.1093/cid/ciy554. PMC 6376090. PMID 30184181.