Zygomaticomaxillary complex fracture
The zygomaticomaxillary complex fracture, also known as a quadripod fracture, quadramalar fracture, and formerly referred to as a tripod fracture or trimalar fracture, has four components, three of which are directly related to connections between the zygoma and the face, and the fourth being the orbital floor. Its specific locations are the lateral orbital wall (at its superior junction with the zygomaticofrontal suture or its inferior junction with the zygomaticosphenoid suture at the sphenoid greater wing), separation of the maxilla and zygoma at the anterior maxilla (near the zygomaticomaxillary suture), the zygomatic arch, and the orbital floor near the infraorbital canal.
| ZMC complex fracture | |
|---|---|
| Other names | Quadripod fracture |
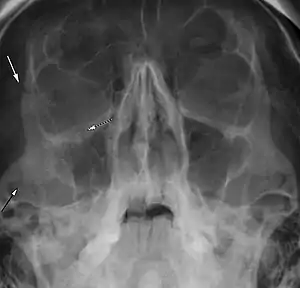 | |
| Right zygomaticomaxillary complex fracture with disruption of the lateral orbital wall, orbital floor, zygomatic arch and maxillary sinus. | |
Signs and symptoms
On physical exam, the fracture appears as a loss of cheek projection with increased width of the face. In most cases, there is loss of sensation in the cheek and upper lip due to infraorbital nerve injury. Facial bruising, periorbital ecchymosis, soft tissue gas, swelling, trismus, altered mastication, diplopia, and ophthalmoplegia are other indirect features of the injury.[1] The zygomatic arch usually fractures at its weakest point, 1.5 cm behind the zygomaticotemporal suture.[2]
Cause
The cause is usually a direct blow to the malar eminence of the cheek during assault. The paired zygomas each have two attachments to the cranium, and two attachments to the maxilla, making up the orbital floors and lateral walls. These complexes are referred to as the zygomaticomaxillary complex. The upper and transverse maxillary bone has the zygomaticomaxillary and zygomaticotemporal sutures, while the lateral and vertical maxillary bone has the zygomaticomaxillary and frontozygomatic sutures.
The formerly used 'tripod fracture' refers to these buttresses, but did not also incorporate the posterior relationship of the zygoma to the sphenoid bone at the zygomaticosphenoid suture.
There is an association of ZMC fractures with naso-orbito-ethmoidal fractures (NOE) on the same side as the injury. Concomitant NOE fractures predict a higher incidence of post operative deformity.[3]
Treatment
Non-displaced or minimally displaced fractures may be treated conservatively. Open reduction and internal fixation is reserved for cases that are severely angulated or comminuted. The purpose of fixation is to restore the normal appearance of the face. Specific attention is given to the position of the malar eminence and reduction of orbital volume by realigning the zygoma and sphenoid. Failure to correct can result in rotational deformity and increase the volume of the orbit, causing the eye to sink inwards.
Fractures with displacement require surgery consisting of fracture reduction with miniplates, microplates and screws. Gillie's approach is used for depressed zygomatic fractures.[4] The prognosis of tripod fractures is generally good. In some cases there may be persistent post-surgical facial asymmetry, which can require further treatment.[5]
References
- Fraioli, RE; Branstetter BF, 4th; Deleyiannis, FW (February 2008). "Facial fractures: beyond Le Fort". Otolaryngologic Clinics of North America. 41 (1): 51–76, vi. doi:10.1016/j.otc.2007.10.003. PMID 18261526.
- Winegar, BA; Murillo, H; Tantiwongkosi, B (2013). "Spectrum of critical imaging findings in complex facial skeletal trauma". Radiographics. 33 (1): 3–19. doi:10.1148/rg.331125080. PMID 23322824.
- Buchanan, EP; Hopper, RA; Suver, DW; Hayes, AG; Gruss, JS; Birgfeld, CB (December 2012). "Zygomaticomaxillary complex fractures and their association with naso-orbito-ethmoid fractures: a 5-year review". Plastic and Reconstructive Surgery. 130 (6): 1296–304. doi:10.1097/prs.0b013e31826d1643. PMID 23190812. S2CID 19945049.
- Swanson, E; Vercler, C; Yaremchuk, MJ; Gordon, CR (May 2012). "Modified Gillies approach for zygomatic arch fracture reduction in the setting of bicoronal exposure". The Journal of Craniofacial Surgery. 23 (3): 859–62. doi:10.1097/scs.0b013e31824dd5c3. PMID 22565912. S2CID 33669080.
- Linnau, KF; Stanley RB, Jr; Hallam, DK; Gross, JA; Mann, FA (October 2003). "Imaging of high-energy midfacial trauma: what the surgeon needs to know". European Journal of Radiology. 48 (1): 17–32. doi:10.1016/s0720-048x(03)00205-5. PMID 14511857.