Candida auris
Candida auris is a species of fungus that grows as yeast.[1] It is one of the few species of the genus Candida which cause candidiasis in humans. Often, candidiasis is acquired in hospitals by patients with weakened immune systems. C. auris can cause invasive candidiasis (fungemia) in which the bloodstream, the central nervous system, and internal organs are infected. It has attracted widespread attention because of its multiple drug resistance. Treatment is also complicated because it is easily misidentified as other Candida species.
| Candida auris | |
|---|---|
 | |
| Scientific classification | |
| Kingdom: | Fungi |
| Division: | Ascomycota |
| Class: | Saccharomycetes |
| Order: | Saccharomycetales |
| Family: | Saccharomycetaceae |
| Genus: | Candida |
| Species: | C. auris |
| Binomial name | |
| Candida auris | |
| Type strain | |
| DSM 21092[2] | |
Candida auris was first described in 2009 after it was isolated from the ear canal of a 70-year-old Japanese woman at the Tokyo Metropolitan Geriatric Hospital in Japan. In 2011, South Korea saw its first cases of disease-causing C. auris. Reportedly, this spread across Asia and Europe, and first appeared in the U.S. in 2013.[4]
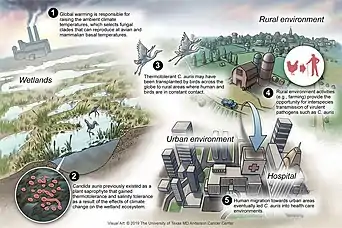
DNA analysis of four distinct but drug-resistant strains of Candida auris indicate an evolutionary divergence taking place at least 4,000 years ago, with a common leap among the four varieties into drug-resistance possibly linked to widespread azole-type antifungal use in agriculture.[4] However, explanations for its emergence remain speculative.
Identification and morphology
First identified in 2009, Candida auris is a species of ascomycetous fungus of the genus Candida that grows as a yeast.[1] Its name comes from the Latin word for ear, auris.[5] It forms smooth, shiny, whitish-gray, viscous colonies on growth media. Microscopically cells are ellipsoid in shape.[1]
Clinical significance
Candida auris is one of the few Candida species that can cause candidiasis in humans. Candidiasis is most often acquired in hospitals by patients with weakened immune systems. It can cause invasive candidiasis, in which the blood stream (fungemia), the central nervous system, kidneys, liver, bones, muscles, joints, spleen, or eyes are invaded. It usually presents with other co-morbidities such as diabetes, sepsis, lung diseases, and kidney diseases.
Candida auris has attracted increased clinical attention because of its multiple drug resistance.[6][7][4]
In vitro, more than 90% of C. auris isolates are resistant to fluconazole[8][9] and a range of 3–73% of C. auris isolates are resistant to voriconazole,[9][10] while other triazoles (posaconazole, itraconazole, and isavuconazole) display better activity.[8][9][10] Of isolates 13% to 35% were reported resistant to amphotericin B;[8][10] however, most isolates are susceptible to echinocandins.[8][9][10]
Treatment is complicated because C. auris is easily misidentified as various other Candida species.[6][7] [11][12] A brief outline of its clinical relevance as of 2016, understandable by general audiences, was published by the Center for Infectious Disease Research and Policy at the University of Minnesota.[13]
According to the Centers for Disease Control and Prevention (CDC), 30–60% of people with C. auris bloodstream infections (BSI) have died.[14] However, many of these people had other serious illnesses and conditions (comorbidities) that also increased their risk of death.[14][15]
Vaccine development
There is currently no vaccine for Candida auris, however, attempts have been made, with experiments involving the NDV-3A vaccine that successfully immunized mice against the fungus.[16] The vaccine also improved the protective efficacy of the antifungal drug micafungin against C. auris infection in the bloodstream.[17]
Genome
Several draft genomes from whole genome sequencing have been published.[6][18] C. auris has a genome size of 12.3–12.5 Mb with a GC-content of 44.5–44.8%.[6][18] The C. auris genome was found to encode several genes for the ABC transporter family, a major facilitator superfamily, which helps to explain its multiple drug resistance.[6] Its genome also encodes virulence-related gene families such as lipases, oligopeptide transporters, mannosyl transferases and transcription factors which facilitate colonization, invasion, and iron acquisition.[6] Another factor contributing to antifungal resistance is the presence of a set of genes known to be involved in biofilm formation.[6]
More studies are needed to determine whether the phylogenetic divergence of C. auris clones exhibits region-specific patterns of invasiveness, virulence, and/or drug resistance.[19]
Epidemiology
Geographical differentiation
The phylogenetics of C. auris suggest distinct genotypes exist in different geographical regions with substantial genomic diversity.[19] A variety of sequence-based analytical methods have been used to support this finding.
Whole genome sequencing and analyses of isolates from Pakistan, India, South Africa, Venezuela, Japan, and previously sequenced C. auris genomes deposited in the National Center for Biotechnology Information's Sequence Read Archive[20] identified a distinct geographic distribution of genotypes.[8] Four distinct clades separated by tens of thousands of single-nucleotide polymorphisms were identified.[8] The distribution of these clades segregated geographically to South Asia (India and Pakistan), South Africa, Venezuela, and Japan with minimal observed intraregion genetic diversity.[8]
Amplified fragment length polymorphism analysis of C. auris isolates from the United Kingdom, India, Japan, South Africa, South Korea, and Venezuela suggested that the London isolates formed a distinct cluster compared to the others.[21]
Comparison of ribosomal DNA sequences of C. auris isolates from Israel, Asia, South Africa, and Kuwait found that the strains from Israel were phylogenetically distinct from those from the other regions.[22] Chatterjee et al. wrote in 2015, "Its actual global distribution remains obscure as the current commercial methods of clinical diagnosis misidentify it as C. haemulonii."[6]
History


Candida auris was first described after it was isolated from the ear canal of a 70-year-old Japanese woman at the Tokyo Metropolitan Geriatric Hospital in Japan.[1] It was isolated based on its ability to grow in the presence of the fungicide micafungin, an echinocandin class fungicide.[1] Phenotypic, chemotaxonomic and phylogenetic analyses established C. auris as a new strain of the genus Candida.[1][23]
The first three cases of disease-causing C. auris were reported from South Korea in 2011.[24] Two isolates had been obtained during a 2009 study and a third was discovered in a stored sample from 1996.[24] All three cases had persistent fungemia, i.e. bloodstream infection, and two of the patients subsequently died due to complications.[24] Notably, the isolates initially were misidentified as Candida haemulonii and Rhodotorula glutinis using standard methods, until sequence analysis correctly identified them as C. auris.[24] These first cases emphasize the importance of accurate species identification and timely application of the correct antifungal for the effective treatment of candidiasis with C. auris.[24]
During 2009–2011, 12 C. auris isolates were obtained from patients at two hospitals in Delhi, India.[25] The same genotype was found in distinct settings: intensive care, surgical, medical, oncologic, neonatal, and pediatric wards, which were mutually exclusive with respect to health care personnel.[25] Most had persistent candidemia and a high mortality rate was observed.[25] All isolates were of the same clonal strain, however, and were only identified positively by DNA sequence analysis.[25] As previously, the strain was misidentified with established diagnostic laboratory tests.[25] The Indian researchers wrote in 2013 that C. auris was much more prevalent than published reports indicate since most diagnostic laboratories do not use sequence-based methods for strain identification.[25]
The fungus spread to other continents and eventually, a multi-drug-resistant strain was discovered in Southeast Asian countries in early 2016.[26]
The first report of a C. auris outbreak in Europe was an October 2016 in Royal Brompton Hospital, a London cardio-thoracic hospital.[21] In April 2017, CDC director Anne Schuchat named it a "catastrophic threat".[27] As of May 2017 the CDC had reported 77 cases in the United States. Of these, 69 were from samples collected in New York and New Jersey.[28]
As of 31 August 2019 the number of cases of people having contracted C. auris in the United States had risen to 806, with 388 reported in New York, 137 in New Jersey and 227 in Illinois, according to the CDC.[4][29]
Since it was first observed in the United Kingdom, it has spread to more than 20 NHS Trust hospitals and infected 200 people.[30]
As of April 2019, the CDC has documented cases of C. auris from the following countries: Australia, Austria, Belgium, Canada, China, Colombia, France, Germany, India, Iran, Israel, Japan, Kenya, Kuwait, Malaysia, Mexico, the Netherlands, Norway, Oman, Pakistan, Panama, Russia, Saudi Arabia, Singapore, South Africa, South Korea, Spain, Switzerland, Taiwan, Thailand, the United Arab Emirates, the United Kingdom, the United States, and Venezuela.[29]
Candida auris fungus (C. auris) is a multi-drug–resistant fungal infection that spreads in hospitals and is extremely deadly—killing as many as one in three who get it.
- —Abby Haglage of Yahoo! Lifestyle,[31] citing the Centers for Disease Control and Prevention[32]
Arturo Casadevall, MD, PhD, and Molecular Microbiology and Immunology chair at Johns Hopkins Bloomberg School of Public Health stated:
What this study suggests is this is the beginning of fungi adapting to higher temperatures, and we are going to have more and more problems as the century goes on. Global warming will lead to selection of fungal lineages that are more thermally tolerant.[31]
The COVID-19 pandemic has taken resources away from combating and tracking the fungus, which has led to outbreaks.[33] Shortages of personal protective equipment forced medical personnel to reuse of gowns and masks during the pandemic, which has contributed to the fungi's spread.[33] In 2021, the CDC identified strains of Candida auris that were immune to all existing medications used to treat fungal infections.[34]
Context
Antimicrobial resistance in general is an increasingly common phenomenon. In 2010, two million people were reported to have contracted resistant infections in the United States – 23,000 fatally.[upper-alpha 1] "[M]ore recent estimates from researchers at Washington University School of Medicine put the death toll at 162,000. Worldwide fatalities from resistant infections are estimated at 700,000 per year.[4][35] C. auris is one of the many microbial contributors to this global AMR estimation.[35]
See also
References
Notes
- According to official Center for Disease Control estimations.[4]
Citations
- Satoh K, Makimura K, Hasumi Y, Nishiyama Y, Uchida K, Yamaguchi H (January 2009). "Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital". Microbiology and Immunology. 53 (1): 41–4. doi:10.1111/j.1348-0421.2008.00083.x. PMID 19161556.
- "Candida auris". DSMZ – German Collection of Microorganisms and Cell Cultures. Retrieved 1 August 2017.
- Casadevall A, Kontoyiannis DP, Robert V (July 2019). "On the Emergence of Candida auris: Climate Change, Azoles, Swamps, and Birds". mBio. 10 (4): e01397–19. doi:10.1128/mBio.01397-19. PMC 6650554. PMID 31337723.
- Richtel M, Jacobs A (6 April 2019). "A Mysterious Infection, Spanning the Globe in a Climate of Secrecy". The New York Times. ISSN 0362-4331. Retrieved 7 April 2019.
C. auris is so tenacious, in part, because it is impervious to major antifungal medications, making it a new example of one of the world's most intractable health threats: the rise of drug-resistant infections.
- "Candida auris Questions and Answers". Centers for Disease Control and Prevention (CDC). 4 November 2016. Archived from the original on 2 January 2017. Retrieved 1 January 2017.
- Chatterjee S, Alampalli SV, Nageshan RK, Chettiar ST, Joshi S, Tatu US (September 2015). "Draft genome of a commonly misdiagnosed multidrug resistant pathogen Candida auris". BMC Genomics. 16 (1): 686. doi:10.1186/s12864-015-1863-z. PMC 4562351. PMID 26346253.
- "Identification of Candida auris". Centers for Disease Control and Prevention (CDC). Retrieved 1 April 2017.
- Lockhart SR, Etienne KA, Vallabhaneni S, Farooqi J, Chowdhary A, Govender NP, et al. (January 2017). "Simultaneous Emergence of Multidrug-Resistant Candida auris on 3 Continents Confirmed by Whole-Genome Sequencing and Epidemiological Analyses". Clinical Infectious Diseases. 64 (2): 134–140. doi:10.1093/cid/ciw691. PMC 5215215. PMID 27988485.
- Chowdhary A, Anil Kumar V, Sharma C, Prakash A, Agarwal K, Babu R, et al. (June 2014). "Multidrug-resistant endemic clonal strain of Candida auris in India". European Journal of Clinical Microbiology & Infectious Diseases. 33 (6): 919–26. doi:10.1007/s10096-013-2027-1. PMID 24357342. S2CID 14873835.
- Rudramurthy SM, Chakrabarti A, Paul RA, Sood P, Kaur H, Capoor MR, et al. (June 2017). "Candida auris candidaemia in Indian ICUs: analysis of risk factors". The Journal of Antimicrobial Chemotherapy. 72 (6): 1794–1801. doi:10.1093/jac/dkx034. PMID 28333181.
- "Clinical Alert to U.S. Healthcare Facilities - June 2016". Centers for Disease Control and Prevention (CDC). 27 June 2019. Retrieved 2 July 2019.
- "Candida auris Clinical Update - September 2017". Centers for Disease Control and Prevention (CDC). 27 June 2019. Retrieved 2 July 2019.
- Dall C (29 June 2016). "CDC issues warning on multidrug-resistant yeast infection". CIDRAP News.
- Spivak ES, Hanson KE (February 2018). Kraft CS (ed.). "Candida auris: An Emerging Fungal Pathogen". Journal of Clinical Microbiology. 56 (2): e01588–17. doi:10.1128/JCM.01588-17. PMC 5786713. PMID 29167291.
- Chakrabarti A, Sood P, Rudramurthy SM, Chen S, Kaur H, Capoor M, et al. (February 2015). "Incidence, characteristics and outcome of ICU-acquired candidemia in India". Intensive Care Medicine. 41 (2): 285–95. doi:10.1007/s00134-014-3603-2. PMID 25510301. S2CID 10471076.
- Harper, Rachel (7 August 2019). "Major step towards Candida auris vaccine developed". (European Pharmaceutical Review). Archived from the original on 7 August 2019. Retrieved 1 February 2021.
- Singh, Shakti; Uppuluri, Priya; Mamouei, Zeinab; Alqarihi, Abdullah; Elhassan, Hana; French, Samuel; Lockhart, Shawn R.; Chiller, Tom; Edwards, John E.; Ibrahim, Ashraf S. (August 2019). "The NDV-3A vaccine protects mice from multidrug resistant Candida auris infection". PLOS Pathogens. 15 (8): e1007460. doi:10.1371/journal.ppat.1007460. ISSN 1553-7374. PMC 6695204. PMID 31381597.
- Sharma C, Kumar N, Meis JF, Pandey R, Chowdhary A (July 2015). "Draft Genome Sequence of a Fluconazole-Resistant Candida auris Strain from a Candidemia Patient in India". Genome Announcements. 3 (4): e00722–15. doi:10.1128/genomeA.00722-15. PMC 4505117. PMID 26184929.
- Ben-Ami R, Berman J, Novikov A, Bash E, Shachor-Meyouhas Y, Zakin S, et al. (February 2017). "Multidrug-Resistant Candida haemulonii and C. auris, Tel Aviv, Israel". Emerging Infectious Diseases. 23 (1): 195–203. doi:10.3201/eid2302.161486. PMC 5324804. PMID 28098529.
- National Center for Biotechnology Information's Sequence Read Archive U.S. National Library of Medicine, retrieved 31 May 2017
- Schelenz S, Hagen F, Rhodes JL, Abdolrasouli A, Chowdhary A, Hall A, et al. (19 October 2016). "Candida auris in a European hospital". Antimicrobial Resistance and Infection Control. 5: 35. doi:10.1186/s13756-016-0132-5. PMC 5069812. PMID 27777756.
- Miller R (April 1966). "Hospital design". Hospitals. 40 (7): 91–4. PMID 5324804.
- "Candida auris". MycoBank. Retrieved 2 April 2017.
- Lee WG, Shin JH, Uh Y, Kang MG, Kim SH, Park KH, Jang HC (September 2011). "First three reported cases of nosocomial fungemia caused by Candida auris". Journal of Clinical Microbiology. 49 (9): 3139–42. doi:10.1128/JCM.00319-11. PMC 3165631. PMID 21715586.
- Chowdhary A, Sharma C, Duggal S, Agarwal K, Prakash A, Singh PK, et al. (October 2013). "New clonal strain of Candida auris, Delhi, India". Emerging Infectious Diseases. 19 (10): 1670–3. doi:10.3201/eid1910.130393. PMC 3810747. PMID 24048006.
- Maryn McKenna (7 November 2016). "Fatal Fungus Linked to 4 New Deaths – What You Need to Know". National Geographic. National Geographic Society. Archived from the original on 2 January 2017. Retrieved 1 January 2017.
- Blau M (21 April 2017). "'Catastrophic threat': CDC chief fears a deadly superbug's spread". Stat News. Retrieved 23 April 2017.
- Tsay S, Welsh RM, Adams EH, Chow NA, Gade L, Berkow EL, et al. (May 2017). "Notes from the Field: Ongoing Transmission of Candida auris in Health Care Facilities - United States, June 2016-May 2017". MMWR. Morbidity and Mortality Weekly Report. 66 (19): 514–515. doi:10.15585/mmwr.mm6619a7. PMC 5657645. PMID 28520710.
- "Tracking Candida auris". Centers for Disease Control and Prevention (CDC). 31 August 2019. Retrieved 26 November 2019.
- Henk D (21 August 2017). "A killer fungus is spreading through UK hospitals – here's what you need to know about Candida auris". The Independent. Retrieved 27 August 2017.
- Haglage A (24 July 2019). "Deadly new fungal superbug is worrying doctors—here's what you need to know". Yahoo! Lifestyle. Retrieved 13 November 2019.
- "Candida auris: A Drug-resistant Germ That Spreads in Healthcare Facilities". Centers for Disease Control and Prevention. 21 December 2018. Retrieved 13 November 2019.
- Richtel, Matt (27 January 2021). "With All Eyes on Covid-19, Drug-Resistant Infections Crept In". The New York Times. Retrieved 28 January 2021.
- Jacobs, Andrew (23 July 2021). "Outbreaks of Untreatable, Drug-Resistant Fungus Spread in 2 Cities". The New York Times. Retrieved 24 July 2021.
- O'Neill J (2016). Tackling drug-resistant infections globally : final report and recommendations. OCLC 979367942.