Cellular adoptive immunotherapy
Cellular adoptive immunotherapy is a type of immunotherapy. Immune cells such as T-cells are usually isolated from patients for expansion or engineering purposes and reinfused back into patients to fight diseases using their own immune system. A major application of cellular adoptive therapy is cancer treatment, as the immune system plays a vital role in the development and growth of cancer.[1] The primary types of cellular adoptive immunotherapies are T cell therapies. Other therapies include CAR-T therapy, CAR-NK therapy, macrophage-based immunotherapy and dendritic cell therapy.

History
Although immunotherapy with immune checkpoint blockade and targeted therapy was used to treat and improve the survival of patients with several types of cancers, such as non-small cell lung cancer, many patients still develop disease progression even after receiving these therapies. Cellular adoptive therapy is another alternative for these patients. The first studies with tumor-infiltrating lymphocytes (TILs) were performed at the Surgery Branch in the National Institutes of Health. These studies used TILs grown from different murine tumors and showed in vivo anti-tumor activity of these cells. Current cellular adoptive therapies consist of the ex-vivo expansion of TILs from resected tumors and transferred back to the patients' bodies with support of interleukin -2 (IL–2). This treatment has been shown to be effective in tumors such as metastatic melanoma.[1]
T - cell therapies
Tumor-Infiltrating Lymphocyte (TIL) Therapy
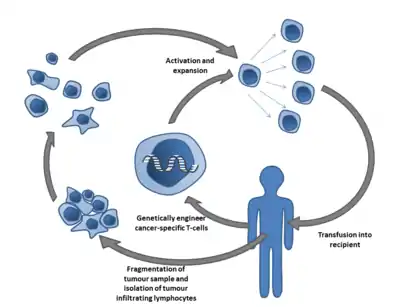
Although T- cells are powerful tools that help us defend against cancer through immune responses, errors may still occur during the process, and cancer's anti-tumour effect may vary. For example, the T- cells may not be activated and sustain the anti-tumor effect long enough, or the number of T-cells presented is insufficient. TIL therapy isolates tumor-infiltrating lymphocytes (TILs), which are naturally occurring T cells in cancer patients that have already recognised cancer cells and infiltrated into the tumor as an anti-tumor response from their own immune system after tumor resection. These isolated cells will then be cultured with interleukin-2 and tested to choose cells with high tumor recognition or selected through the "young TIL" approach. Selected cells are activated and rapidly expanded, then re-infused back into the patient.[1][2]
Melanoma
Melanoma was the first type of tumor that provided insight into cancer immunotherapy due to its high immunogenicity. TIL therapy has been shown to be one of the most effective methods against metastatic melanoma.[3]
Other solid tumors
Apart from melanoma, TIL therapy can also be applied to other solid tumors. The presence of TILs has been considered an important factor for predicting clinical outcome and prognosis of cancer patients with different types of tumors such as Head and neck squamous cell carcinoma (A type of head and neck cancer), ovarian cancer, and renal cell carcinoma (RCC).[4][5][6] However, previous clinical trials of TIL therapy on patients with ovarian cancer and renal cell carcinoma have only shown mixed results and modest success respectively.[5]
Advantages
TILs in TIL therapy were exposed and stimulated by tumor antigens before isolation. These tumors often express chemokine receptors and combine with the tumor-specific T-cell receptors presented on them. This makes it easier for the TILs to target tumor cells after being re-infused. Off-target toxicity was also rarely reported in TIL therapy.[2]
Challenges
1) TIL therapy needs to overcome the heterogeneity of solid tumors, which adds difficulty to the identification of a target for all tumor cells.[2]
2) Achieving full function of T cells and tumor microenvironment (TME) with different immunosuppressive mechanisms is another primary concern.[2]
Engineered T Cell Receptor (TCR) Therapy
TCR therapy has a similar principle as TIL therapy. However, TCR therapy isolates peripheral blood T cells and engineers them to target tumor tissues. This therapy has shown to be more effective in treating solid tumors than other cellular adoptive immunotherapies such as CAR T cell therapy.
Challenges
| Manufacturing | The production of TCR T-cells requires complex processes with strict monitoring. Moreover, the cost of the manufacturing process is expensive.[7]
Cost of single infusions of axicabtagene ciloleucel: US$373,000 Tisagenlecleucel: US$475,000 |
| T cell | Efficacy of treatment highly depends on whether infused cells can persist within patients. Increasing the T - cell persistence has been a major challenge and direction for TCR therapy.[7] |
| Tumor microenvironment | Tumor microenvironments are usually immunosuppressive. They attract immunosuppressive cells and promote cancer cell survival. Thus, making it difficult for T - cells to perform anti-tumor functions.[7] |
Chimeric Antigen Receptor (CAR) T Cell Therapy
Chimeric antigen receptor T-cells (CAR-T) are predominantly used in cancer immunotherapy. T-cells are harvested from patients' bodies and infused after genetic engineering (equipped with CAR construct). And the currently developing mRNA vaccine technology may provide the possibility for in vivo CAR induction in the future.
Applications
The major application of CAR-T immunotherapy is to treat hematological malignancies, such as multiple myeloma, chronic lymphocytic leukemia, acute lymphoblastic leukemia and lymphoma.[8] Also, CAR-T-related solid tumor treatments have become increasingly promising due to protein and cell engineering improvements.[9]
Hematological malignancies
Acute lymphoblastic leukemia (ALL)
Anti-CD19 (CD19 is crucial for B cell lineage, which is overexpressed on leukemic B-cells) is the most commonly used and effective CAR in ALL treatments. Many clinical studies have reported its efficacy with satisfying complete and partial remission rates (CR and PR).[8] Besides anti-CD19, other potential candidates include anti-CD20 and immunoglobulin light chains. Further suggestions from clinical trials such as controlled CD4+ and CD8+ CAR-T could be potential strategies to investigate factors relevant to the drug efficacy, adverse effects, etc.
Other hematological malignancies
Targeting different biomarkers can treat chronic lymphocytic leukemia, lymphoma and multiple myeloma.
Solid tumors
Potential treatments for melanoma, breast cancer and sarcoma are still in the research phase. The challenges for CAR-T therapy to achieve efficacy and recent development and improvement will be discussed in the limitation and recent advances and future improvement section.[8]
Side effects
Neurological complications
Confusion, deliriumand occasional seizures and cerebral edema are observed as adverse effects of anti-CD19 CAR-T, which still lack well-explained pathogenesis [3]. Furthermore, the immune effector cell-associated neurotoxicity can cause death occasionally. Some hypothesized causes such as endothelial cell activation and the increase of blood-brain barrier permeability are still under investigation. Nakinra, an anti-IL-1R antibody, has exhibited an anti-neurotoxicity effect on CAR-T treated murine model.
Cytokine release syndrome (CRS)
Hemophagocytic lymphohistiocytosis, macrophage activation syndrome, and CRS are common side effects after CAR-T treatment.[8]
Main articles: Cytokine release syndrome; chimeric antigen receptor T cell.
IgE-mediated anaphylactic reaction
CAR derived from humanized mice or human antibodies might still be recognized as a foreign antigen and be attacked by patients' immune systems, causing IgE-mediated anaphylactic responses.[8]
Advantages
CAR-T therapy exhibits distinct specificity compared to other adaptive immunotherapies and traditional cancer treatments such as chemotherapy.[8] CAR-T kill tumor cells specifically by targeting the tumor-associated antigens to keep the damage to healthy tissue at a minimum level. Additionally, these engineered T-cells can perform their function independent from HLA - major histocompatibility complex (MHC) presentation. Furthermore, CAR structure can be manipulated flexibly to target different antigens, which greatly promises the extension of its application.
Limitations
1) To achieve complete remission, manufacture of CAR-T, infusion, and efficacy of tumor-killing effect must all be successfully performed. Sometimes, it is hard to harvest sufficient T-cells from a patient, CAR-T fails to expand in vitro or in vitro, or CAR-T exhibit poor persistence. These would lead to Failure to achieve durable remissions. 2) And therapy efficacy would be limited by antigen modulation related to antigen down-regulation and when infused back into patients' bodies. Hence disease relapse occurs frequently. 3) Toxicity and adverse events. 4) CAR-T treatment efficacy and safety are greatly reduced because of solid tumors' immunosuppressive microenvironment and the lack of distinct tumor antigen as the target.[10]
Recent advances and future improvements
CAR structure is continuously developing from the first generation to the fourth, improving cell expansion, efficacy, and persistence.[11]
Other therapies
CAR-NK therapy
Natural killer cells belong to the innate immune system, while they perform anti-tumor functions in a very similar mechanism to CD8+ cytotoxic T-cells. CAR-NK provides new perspectives in the cancer immunotherapy field after the advancement of CAR-T therapy.
Advantages
- Improved safety: mitigated cytokine release syndrome, neurotoxicity and graft-versus-host response compared to CAR-T therapy.
- Multiple activation mechanisms: can perform cytotoxic activity both CAR-dependently and CAR-independently.
- "off-the-shelf" potential.[12]
Limitations
The lack of an efficient way for gene transduction is the major limitation of CAR-NK therapy. Although retroviral vectors exhibit up to 70% efficiency with the presence of membrane-bound cytokines, it would bring problems such as insertional mutagenesis and reduced NK viability. While lentivirus transduction generally causes lower genotoxicity but with lower transfection efficiency.[12]
Dendritic cell therapy
Main article: see Cancer immunotherapy
Prospects
The final destination of cellular adoptive therapies is to create cellular products that are personalized and specific to each patient's tumor - hopefully creating products that can target different tumors in cancer patients. The future direction of cellular adoptive therapies focuses on improving anti-tumor effects of the therapies and reducing toxicity.[1]
For T - cell therapies
Increasing the reactivity of TIL towards tumor antigen through CD137 or PD-1 is a possible direction of treatment improvement. Gene editing on TILs by genetic editing tools such as Zinc finger nucleases to decrease PD-1 expression on TILs is another way to improve the efficacy of TIL therapy.[1]
Another major challenge to tackle is to reduce the 'on target, off tumor' toxicity of TCR therapy. Antigens presented only on the tumor, but not in the healthy tissue should be identified to decrease the chance of TCRs targeting healthy tissue. Side effects should also be reduced by techniques such as tumor reduction prior to therapy and dose adaptive strategies.[1]
For chimeric antigen receptor related therapies
Besides the structural development of CAR constructs, the mRNA vaccine could provide a novel platform for CAR delivery and induction in vivo. Recently, the COVID-19 mRNA vaccine was approved by the FDA, which is lipid nanoparticle loaded. If the mRNA delivery strategy is applied to cellular adoptive therapy, the manufacture of CAR immune cells could be more time-efficient and cost-effective. It means cancer patients with aggressive tumor exacerbation could be saved in time. Moreover, the currently expensive immunotherapies would be more affordable to the general public.[13]
References
- Rohaan, Maartje W.; Wilgenhof, Sofie; Haanen, John B. A. G. (2018-11-23). "Adoptive cellular therapies: the current landscape". Virchows Archiv. 474 (4): 449–461. doi:10.1007/s00428-018-2484-0. ISSN 1432-2307. PMC 6447513. PMID 30470934.
- Wang, Shuhang; Sun, Jingwei; Chen, Kun; Ma, Peiwen; Lei, Qi; Xing, Shujun; Cao, Zhongzheng; Sun, Shujun; Yu, Zicheng; Liu, Yarong; Li, Ning (2021-06-11). "Perspectives of tumor-infiltrating lymphocyte treatment in solid tumors". BMC Medicine. 19 (1): 140. doi:10.1186/s12916-021-02006-4. ISSN 1741-7015. PMC 8194199. PMID 34112147.
- Lee, Sylvia; Margolin, Kim (2012-08-10). "Tumor-infiltrating lymphocytes in melanoma". Current Oncology Reports. 14 (5): 468–474. doi:10.1007/s11912-012-0257-5. ISSN 1523-3790. PMC 3462483. PMID 22878966.
- Santoiemma, Phillip P; Powell, Daniel J (2015-04-20). "Tumor infiltrating lymphocytes in ovarian cancer". Cancer Biology & Therapy. 16 (6): 807–820. doi:10.1080/15384047.2015.1040960. ISSN 1538-4047. PMC 4622931. PMID 25894333.
- Andersen, Rikke; Donia, Marco; Westergaard, Marie Christine Wulff; Pedersen, Magnus; Hansen, Morten; Svane, Inge Marie (2015-08-26). "Tumor infiltrating lymphocyte therapy for ovarian cancer and renal cell carcinoma". Human Vaccines & Immunotherapeutics. 11 (12): 2790–2795. doi:10.1080/21645515.2015.1075106. ISSN 2164-5515. PMC 5054777. PMID 26308285.
- Almangush, Alhadi; De Keukeleire, Stijn; Rottey, Sylvie; Ferdinande, Liesbeth; Vermassen, Tijl; Leivo, Ilmo; Mäkitie, Antti A. (2022-03-18). "Tumor-Infiltrating Lymphocytes in Head and Neck Cancer: Ready for Prime Time?". Cancers. 14 (6): 1558. doi:10.3390/cancers14061558. ISSN 2072-6694. PMC 8946626. PMID 35326709.
- Shafer, Paul; Kelly, Lauren M.; Hoyos, Valentina (2022). "Cancer Therapy With TCR-Engineered T Cells: Current Strategies, Challenges, and Prospects". Frontiers in Immunology. 13: 835762. doi:10.3389/fimmu.2022.835762. ISSN 1664-3224. PMC 8928448. PMID 35309357.
- Zhao, Zijun; Chen, Yu; Francisco, Ngiambudulu M.; Zhang, Yuanqing; Wu, Minhao (2018-07-01). "The application of CAR-T cell therapy in hematological malignancies: advantages and challenges". Acta Pharmaceutica Sinica B. SI: Targeted Cancer Therapy. 8 (4): 539–551. doi:10.1016/j.apsb.2018.03.001. ISSN 2211-3835. PMC 6090008. PMID 30109179.
- Hou, Andrew J.; Chen, Laurence C.; Chen, Yvonne Y. (2021-05-10). "Navigating CAR-T cells through the solid-tumour microenvironment". Nature Reviews Drug Discovery. 20 (7): 531–550. doi:10.1038/s41573-021-00189-2. ISSN 1474-1784. PMID 33972771. S2CID 234362096.
- Shah, Nirali N.; Fry, Terry J. (2019-03-05). "Mechanisms of resistance to CAR T cell therapy". Nature Reviews Clinical Oncology. 16 (6): 372–385. doi:10.1038/s41571-019-0184-6. ISSN 1759-4782. PMC 8214555. PMID 30837712.
- Huang, Ruihao; Li, Xiaoping; He, Yundi; Zhu, Wen; Gao, Lei; Liu, Yao; Gao, Li; Wen, Qin; Zhong, Jiang F.; Zhang, Cheng; Zhang, Xi (2020-07-02). "Recent advances in CAR-T cell engineering". Journal of Hematology & Oncology. 13 (1): 86. doi:10.1186/s13045-020-00910-5. ISSN 1756-8722. PMC 7333410. PMID 32616000.
- Xie, Guozhu; Dong, Han; Liang, Yong; Ham, James Dongjoo; Rizwan, Romee; Chen, Jianzhu (2020-09-01). "CAR-NK cells: A promising cellular immunotherapy for cancer". EBioMedicine. 59: 102975. doi:10.1016/j.ebiom.2020.102975. ISSN 2352-3964. PMC 7452675. PMID 32853984.
- Miao, Lei; Zhang, Yu; Huang, Leaf (2021-02-25). "mRNA vaccine for cancer immunotherapy". Molecular Cancer. 20 (1): 41. doi:10.1186/s12943-021-01335-5. ISSN 1476-4598. PMC 7905014. PMID 33632261.