Evolutionary medicine
Evolutionary medicine or Darwinian medicine is the application of modern evolutionary theory to understanding health and disease. Modern biomedical research and practice have focused on the molecular and physiological mechanisms underlying health and disease, while evolutionary medicine focuses on the question of why evolution has shaped these mechanisms in ways that may leave us susceptible to disease. The evolutionary approach has driven important advances in the understanding of cancer,[1] autoimmune disease,[2] and anatomy.[3] Medical schools have been slower to integrate evolutionary approaches because of limitations on what can be added to existing medical curricula.[4] The International Society for Evolution, Medicine and Public Health coordinates efforts to develop the field. It owns the Oxford University Press journal Evolution, Medicine and Public Health and The Evolution and Medicine Review.
| Part of a series on |
| Evolutionary biology |
|---|
 |
|
|

Core principles
Utilizing the Delphi method, 56 experts from a variety of disciplines, including anthropology, medicine, and biology agreed upon 14 core principles intrinsic to the education and practice of evolutionary medicine.[5] These 14 principles can be further grouped into five general categories: question framing, evolution I and II (with II involving a higher level of complexity), evolutionary trade-offs, reasons for vulnerability, and culture. Additional information regarding these principles may be found in the table below.
| Topic | Core Principle |
|---|---|
| Types of explanation (question framing) | Both proximate (mechanistic) and ultimate (evolutionary) explanations are needed to provide a full biological understanding of traits, including those that increase vulnerability to disease. |
| Evolutionary processes (evolution I) | All evolutionary processes, including natural selection, genetic drift, mutation, migration and non-random mating, are important for understanding traits and disease. |
| Reproductive success (evolution I) | Natural selection maximizes reproductive success, sometimes at the expense of health and longevity. |
| Sexual selection (evolution I) | Sexual selection shapes traits that result in different health risks between sexes. |
| Constraints (evolution I) | Several constraints inhibit the capacity of natural selection to shape traits that are hypothetically optimal for health. |
| Trade-offs (evolutionary trade-offs) | Evolutionary changes in one trait that improve fitness can be linked to changes in other traits that decrease fitness. |
| Life History Theory (evolutionary trade-offs) | Life history traits, such as age at first reproduction, reproductive lifespan and rate of senescence, are shaped by evolution, and have implications for health and disease. |
| Levels of selection (evolution II) | Vulnerabilities to disease can result when selection has opposing effects at different levels (e.g. genetic elements, cells, organisms, kin and other levels). |
| Phylogeny (evolution II) | Tracing phylogenetic relationships for species, populations, traits or pathogens can provide insights into health and disease. |
| Coevolution (evolution II) | Coevolution among species can influence health and disease (e.g. evolutionary arms races and mutualistic relationships such as those seen in the microbiome). |
| Plasticity (evolution II) | Environmental factors can shift developmental trajectories in ways that influence health and the plasticity of these trajectories can be the product of evolved adaptive mechanisms. |
| Defenses (reasons for vulnerability) | Many signs and symptoms of disease (e.g. fever) are useful defenses, which can be pathological if dysregulated. |
| Mismatch (reasons for vulnerability) | Disease risks can be altered for organisms living in environments that differ from those in which their ancestors evolved. |
| Cultural practices (culture) | Cultural practices can influence the evolution of humans and other species (including pathogens), in ways that can affect health and disease (e.g. anti-biotic use, birth practices, diet, etc.). |
Human adaptations
Adaptation works within constraints, makes compromises and trade-offs, and occurs in the context of different forms of competition.[6]
Constraints
Adaptations can only occur if they are evolvable. Some adaptations which would prevent ill health are therefore not possible.
- DNA cannot be totally prevented from undergoing somatic replication corruption; this has meant that cancer, which is caused by somatic mutations, has not (so far) been eliminated by natural selection.
- Humans cannot biosynthesize vitamin C, and so risk scurvy, vitamin C deficiency disease, if dietary intake of the vitamin is insufficient.
- Retinal neurons and their axon output have evolved to be inside the layer of retinal pigment cells. This creates a constraint on the evolution of the visual system such that the optic nerve is forced to exit the retina through a point called the optic disc. This, in turn, creates a blind spot. More importantly, it makes vision vulnerable to increased pressure within the eye (glaucoma) since this cups and damages the optic nerve at this point, resulting in impaired vision.
Other constraints occur as the byproduct of adaptive innovations.
Trade-offs and conflicts
One constraint upon selection is that different adaptations can conflict, which requires a compromise between them to ensure an optimal cost-benefit tradeoff.
- Running efficiency in women, and birth canal size[7]
- Encephalization, and gut size[8]
- Skin pigmentation protection from UV, and the skin synthesis of vitamin D
- Speech and its use of a descended larynx, and increased risk of choking[9]
Competition effects
Different forms of competition exist and these can shape the processes of genetic change.
- mate choice and disease susceptibility[10]
- genomic conflict between mother and fetus that results in pre-eclampsia[11][12]
"Diseases of civilization"
Humans evolved to live as simple hunter-gatherers in small tribal bands. Contemporary humans now have a very different environment and way of life.[13][14] This change makes present humans vulnerable to a number of health problems, termed "diseases of civilization" and "diseases of affluence". Stone-age humans evolved to live off the land, taking advantage of the resources that were readily available to them. Evolution is slow, and the rapid change from stone-age environments and practices to the world of today is problematic because we are still adapted to stone-age circumstances that no longer apply. This misfit has serious implications for our health. "Modern environments may cause many diseases such as deficiency syndromes like scurvy and rickets".[15]
Diet
In contrast to the diet of early hunter-gatherers, the modern Western diet often contains high quantities of fat, salt, and simple carbohydrates, such as refined sugars and flours. These relatively sudden dietary changes create health problems.[16][17][18]
Life expectancy
Examples of aging-associated diseases are atherosclerosis and cardiovascular disease, cancer, arthritis, cataracts, osteoporosis, type 2 diabetes, hypertension and Alzheimer's disease. The incidence of all of these diseases increases rapidly with aging (increases exponentially with age, in the case of cancer).
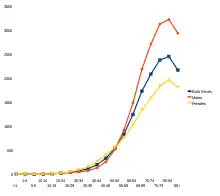
Of the roughly 150,000 people who die each day across the globe, about two thirds—100,000 per day—die of age-related causes.[19] In industrialized nations, the proportion is much higher, reaching 90%.[19]
Exercise
Many contemporary humans engage in little physical exercise compared to the physically active lifestyles of ancestral hunter-gatherers.[20][21][22][23][24] Prolonged periods of inactivity may have only occurred in early humans following illness or injury, so a modern sedentary lifestyle may continuously cue the body to trigger life preserving metabolic and stress-related responses such as inflammation, and some theorize that this causes chronic diseases.[25]
Cleanliness
Contemporary humans in developed countries are mostly free of parasites, particularly intestinal ones. This is largely due to frequent washing of clothing and the body, and improved sanitation. Although such hygiene can be very important when it comes to maintaining good health, it can be problematic for the proper development of the immune system. The hygiene hypothesis is that humans evolved to be dependent on certain microorganisms that help establish the immune system, and modern hygiene practices can prevent necessary exposure to these microorganisms. "Microorganisms and macroorganisms such as helminths from mud, animals, and feces play a critical role in driving immunoregulation" (Rook, 2012[26]). Essential microorganisms play a crucial role in building and training immune functions that fight off and repel some diseases, and protect against excessive inflammation, which has been implicated in several diseases. For instance, recent studies have found evidence supporting inflammation as a contributing factor in Alzheimer's Disease.[27]
Specific explanations
This is a partial list: all links here go to a section describing or debating its evolutionary origin.
Life stage related
Other
- Atherosclerosis[42]
- Arthritis and other chronic inflammatory diseases[29][30][31]
- Cough][43]
- Cystic fibrosis[44]
- Dental occlusion[45]
- Diabetes Type II[46][47]
- Diarrhea[43]
- Essential hypertension[48]
- Fever[49][50]
- Gestational hypertension
- Gout[51]
- Iron deficiency (paradoxical benefits)[52]
- Obesity[53][54]
- Phenylketonuria[55]
- Placebos[56]
- Osteoporosis[57]
- Red blood cell polymorphism disorders[58]
- Sickle cell anemia[59][60]
- Sickness behavior[61]
- Women's reproductive cancers[62]
Evolutionary psychology
As noted in the table below, adaptationist hypotheses regarding the etiology of psychological disorders are often based on analogies with evolutionary perspectives on medicine and physiological dysfunctions (see in particular, Randy Nesse and George C. Williams' book Why We Get Sick).[43] Evolutionary psychiatrists and psychologists suggest that some mental disorders likely have multiple causes.[63]
| Possible Causes of Psychological 'Abnormalities' from an Adaptationist Perspective Summary based on information in Buss (2011),[64] Gaulin & McBurney (2004),[65] Workman & Reader (2004)[66] | ||
|---|---|---|
| Possible cause | Physiological Dysfunction | Psychological Dysfunction |
| Functioning adaptation (adaptive defense) | Fever / Vomiting (functional responses to infection or ingestion of toxins) | Mild depression or anxiety (functional responses to mild loss or stress) |
| By-product of an adaptation(s) | Intestinal gas (byproduct of digestion of fiber) | Sexual fetishes (?) (possible byproduct of normal sexual arousal adaptations that have 'imprinted' on unusual objects or situations) |
| Adaptations with multiple effects | Gene for malaria resistance, in homozygous form, causes sickle cell anemia | Adaptation(s) for high levels of creativity may also predispose schizophrenia or bi-polar disorder (adaptations with both positive and negative effects, perhaps dependent on alternate developmental trajectories) |
| Malfunctioning adaptation | Allergies (over-reactive immunological responses) | Autism (possible malfunctioning of theory of mind module) |
| Frequency-dependent morphs | The two sexes / Different blood and immune system types | Personality traits and personality disorders (may represent alternative behavioral strategies dependent on the frequency of the strategy in the population) |
| Mismatch between ancestral & current environments | Modern diet-related Type 2 Diabetes | More frequent modern interaction with strangers (compared to family and close friends) may predispose greater incidence of depression & anxiety |
| Tails of normal (bell shaped) curve | Very short or tall height | Tails of the distribution of personality traits (e.g., extremely introverted or extroverted) |
See several topic areas, and the associated references, below.
History
Charles Darwin did not discuss the implications of his work for medicine, though biologists quickly appreciated the germ theory of disease and its implications for understanding the evolution of pathogens, as well as an organism's need to defend against them.
Medicine, in turn, ignored evolution, and instead focused (as done in the hard sciences) upon proximate mechanical causes.
medicine has modelled itself after a mechanical physics, deriving from Galileo, Newton, and Descartes.... As a result of assuming this model, medicine is mechanistic, materialistic, reductionistic, linear-causal, and deterministic (capable of precise predictions) in its concepts. It seeks explanations for diseases, or their symptoms, signs, and cause in single, materialistic— i.e., anatomical or structural (e.g., in genes and their products)— changes within the body, wrought directly (linearly), for example, by infectious, toxic, or traumatic agents.[74] p. 510
George C. Williams was the first to apply evolutionary theory to health in the context of senescence.[32] Also in the 1950s, John Bowlby approached the problem of disturbed child development from an evolutionary perspective upon attachment.
An important theoretical development was Nikolaas Tinbergen's distinction made originally in ethology between evolutionary and proximate mechanisms.[75]
Randolph M. Nesse summarizes its relevance to medicine:
all biological traits need two kinds of explanation, both proximate and evolutionary. The proximate explanation for a disease describes what is wrong in the bodily mechanism of individuals affected by it. An evolutionary explanation is completely different. Instead of explaining why people are different, it explains why we are all the same in ways that leave us vulnerable to disease. Why do we all have wisdom teeth, an appendix, and cells that can divide out of control?[76]
The paper of Paul Ewald in 1980, "Evolutionary Biology and the Treatment of Signs and Symptoms of Infectious Disease",[77] and that of Williams and Nesse in 1991, "The Dawn of Darwinian Medicine"[15] were key developments. The latter paper "draw a favorable reception",[43]page x and led to a book, Why We Get Sick (published as Evolution and healing in the UK). In 2008, an online journal started: Evolution and Medicine Review.
See also
- Evolutionary therapy
- Evolutionary psychiatry
- Evolutionary physiology
- Evolutionary psychology
- Evolutionary developmental psychopathology
- Evolutionary approaches to depression
- Illness
- Paleolithic lifestyle
- Universal Darwinism
References
- Merlo LM, Pepper JW, Reid BJ, Maley CC (December 2006). "Cancer as an evolutionary and ecological process". Nature Reviews. Cancer. 6 (12): 924–35. doi:10.1038/nrc2013. PMID 17109012. S2CID 8040576.
- Elliott DE, Weinstock JV (January 2012). "Helminth-host immunological interactions: prevention and control of immune-mediated diseases". Annals of the New York Academy of Sciences. 1247 (1): 83–96. Bibcode:2012NYASA1247...83E. doi:10.1111/j.1749-6632.2011.06292.x. PMC 3744090. PMID 22239614.
- Shubin, Neil (2008). Your inner fish : a journey into the 3.5-billion-year history of the human body (1st ed.). New York: Pantheon Books. ISBN 9780375424472.
- Nesse RM, Bergstrom CT, Ellison PT, Flier JS, Gluckman P, Govindaraju DR, Niethammer D, Omenn GS, Perlman RL, Schwartz MD, Thomas MG, Stearns SC, Valle D (January 2010). "Evolution in health and medicine Sackler colloquium: Making evolutionary biology a basic science for medicine". Proceedings of the National Academy of Sciences of the United States of America. 107. 107 Suppl 1 (suppl_1): 1800–7. Bibcode:2010PNAS..107.1800N. doi:10.1073/pnas.0906224106. PMC 2868284. PMID 19918069.
- Grunspan DZ, Nesse RM, Barnes ME, Brownell SE (2017-12-26). "Core principles of evolutionary medicine: A Delphi study". Evolution, Medicine, and Public Health. 2018 (1): 13–23. doi:10.1093/emph/eox025. PMC 5822696. PMID 29493660.
- Stearns SC (2005). "Issues in evolutionary medicine". American Journal of Human Biology. 17 (2): 131–40. doi:10.1002/ajhb.20105. PMID 15736177. S2CID 42756608.
- Sagan D, Skoyles JR (2002). Up from dragons: the evolution of human intelligence. New York: McGraw-Hill. pp. 240–1. ISBN 978-0-07-137825-3.
- Aiello LC, Wheeler P (1995). "The Expensive-Tissue Hypothesis: The Brain and the Digestive System in Human and Primate Evolution". Current Anthropology. 36 (2): 199–221. doi:10.1086/204350. S2CID 144317407.
- Lieberman P (2007). "The Evolution of Human Speech: Its Anatomical and Neural Bases" (PDF). Current Anthropology. 48 (1): 39–66. doi:10.1086/509092. S2CID 28651524.
- Howard RS, Lively CM (November 2004). "Good vs complementary genes for parasite resistance and the evolution of mate choice". BMC Evolutionary Biology. 4 (1): 48. doi:10.1186/1471-2148-4-48. PMC 543473. PMID 15555062.
- Haig D (December 1993). "Genetic conflicts in human pregnancy". The Quarterly Review of Biology. 68 (4): 495–532. doi:10.1086/418300. PMID 8115596. S2CID 38641716.
- Schuiling GA (September 2000). "Pre-eclampsia: a parent–offspring conflict". Journal of Psychosomatic Obstetrics and Gynaecology. 21 (3): 179–82. doi:10.3109/01674820009075626. PMID 11076340. S2CID 28586243.
- Eaton SB, Konner M, Shostak M (April 1988). "Stone agers in the fast lane: chronic degenerative diseases in evolutionary perspective". The American Journal of Medicine. 84 (4): 739–49. doi:10.1016/0002-9343(88)90113-1. PMID 3135745.
- Knowler WC, Bennett PH, Hamman RF, Miller M (December 1978). "Diabetes incidence and prevalence in Pima Indians: a 19-fold greater incidence than in Rochester, Minnesota". American Journal of Epidemiology. 108 (6): 497–505. doi:10.1093/oxfordjournals.aje.a112648. PMID 736028.
- Williams GC, Nesse RM (March 1991). "The dawn of Darwinian medicine". The Quarterly Review of Biology. 66 (1): 1–22. doi:10.1086/417048. PMID 2052670. S2CID 40357032.
- Eaton SB, Strassman BI, Nesse RM, Neel JV, Ewald PW, Williams GC, Weder AB, Eaton SB, Lindeberg S, Konner MJ, Mysterud I, Cordain L (February 2002). "Evolutionary health promotion" (PDF). Preventive Medicine. 34 (2): 109–18. doi:10.1006/pmed.2001.0876. PMID 11817903. Archived from the original (PDF) on 2008-12-17. Retrieved 2008-08-21.
- Eaton SB (February 2006). "The ancestral human diet: what was it and should it be a paradigm for contemporary nutrition?". The Proceedings of the Nutrition Society. 65 (1): 1–6. doi:10.1079/PNS2005471. PMID 16441938.
- Milton K (September 2003). "Micronutrient intakes of wild primates: are humans different?" (PDF). Comparative Biochemistry and Physiology. Part A, Molecular & Integrative Physiology. 136 (1): 47–59. doi:10.1016/S1095-6433(03)00084-9. PMID 14527629.
- Aubrey DNJ dG (2007). "Life Span Extension Research and Public Debate: Societal Considerations" (PDF). Studies in Ethics, Law, and Technology. 1 (1, Article 5). CiteSeerX 10.1.1.395.745. doi:10.2202/1941-6008.1011. S2CID 201101995. Archived from the original (PDF) on October 13, 2016. Retrieved August 7, 2011.
- Abuissa H, O'Keefe JH, Cordain L (2005). "Realigning our 21st century diet and lifestyle with our hunter-gatherer genetic identity" (PDF). Directions Psych. 25: SR1–SR10. Archived from the original (PDF) on 2008-12-17. Retrieved 2008-08-21.
- Eaton SB, Cordain L, Sebastian A (2007). "The Ancestral Biomedical Environment" (PDF). In Aird WC (ed.). Endothelial Biomedicine. Cambridge University Press. pp. 129–34. ISBN 978-0-521-85376-7.
- Eaton SB, Eaton SB (September 2003). "An evolutionary perspective on human physical activity: implications for health". Comparative Biochemistry and Physiology. Part A, Molecular & Integrative Physiology. 136 (1): 153–9. doi:10.1016/S1095-6433(03)00208-3. PMID 14527637.
- Cordain L, Gotshall RW, Eaton SB, Eaton SB (July 1998). "Physical activity, energy expenditure and fitness: an evolutionary perspective" (PDF). International Journal of Sports Medicine. 19 (5): 328–35. doi:10.1055/s-2007-971926. PMID 9721056. Archived from the original (PDF) on 2008-12-17. Retrieved 2008-08-21.
- Cordain L, Gotshall RW, Eaton SB (1997). "Evolutionary aspects of exercise". Nutrition and Fitness: Evolutionary Aspects, Children's Health, Programs and Policies (PDF). World Review of Nutrition and Dietetics. World Review of Nutrition and Dietetics (Vol. 81 + 82). Vol. 81. pp. 49–60. doi:10.1159/000059601. ISBN 978-3-8055-6452-6. PMID 9287503. Archived from the original (PDF) on 2008-12-17. Retrieved 2019-08-14.
- Charansonney OL, Després JP (August 2010). "Disease prevention--should we target obesity or sedentary lifestyle?". Nature Reviews. Cardiology. 7 (8): 468–72. doi:10.1038/nrcardio.2010.68. PMID 20498671. S2CID 9560960.
- http://www.microbemagazine.org/index.php Archived 2013-10-17 at the Wayback Machine? option=com_content&view=article&id=4700:a-darwinian-view-of-the-hygiene-or-old-friends- hypothesis&catid=950&Itemid=1301
- Fox M, Knapp LA, Andrews PW, Fincher CL (January 2013). "Hygiene and the world distribution of Alzheimer's disease: Epidemiological evidence for a relationship between microbial environment and age-adjusted disease burden". Evolution, Medicine, and Public Health. 2013 (1): 173–86. doi:10.1093/emph/eot015. PMC 3868447. PMID 24481197.
- Kuzawa CW (1998). "Adipose tissue in human infancy and childhood: an evolutionary perspective". American Journal of Physical Anthropology. Suppl. Suppl 27 (S27): 177–209. doi:10.1002/(SICI)1096-8644(1998)107:27+<177::AID-AJPA7>3.0.CO;2-B. PMID 9881526. S2CID 16299149.
- Straub RH, Besedovsky HO (December 2003). "Integrated evolutionary, immunological, and neuroendocrine framework for the pathogenesis of chronic disabling inflammatory diseases". FASEB Journal. 17 (15): 2176–83. doi:10.1096/fj.03-0433hyp. PMID 14656978. S2CID 24742889.
- Straub, R. H., del Rey, A., Besedovsky, H. O. (2007) "Emerging concepts for the pathogenesis of chronic disabling inflammatory diseases: neuroendocrine-immune interactions and evolutionary biology" In: Ader, R. (2007) "Psychoneuroimmunology", Volume 1, Academic Press, San Diego, pp.217-232
- Straub RH, Besedovsky HO, Del Rey A (2007). "[Why are there analogous disease mechanisms in chronic inflammatory diseases?]". Wiener Klinische Wochenschrift (in German). 119 (15–16): 444–54. doi:10.1007/s00508-007-0834-z. PMID 17721763. S2CID 22737085.
- Williams GC (1957). "Pleiotropy, Natural Selection, and the Evolution of Senescence" (PDF). Evolution. 11 (4): 398–411. doi:10.2307/2406060. JSTOR 2406060. Archived from the original (PDF) on 2006-09-19. Retrieved 2008-12-29. abstract
- Wick G, Berger P, Jansen-Dürr P, Grubeck-Loebenstein B (2003). "A Darwinian-evolutionary concept of age-related diseases". Experimental Gerontology. 38 (1–2): 13–25. doi:10.1016/S0531-5565(02)00161-4. PMID 12543257. S2CID 6009798.
- Bogin, B. (1997) "Evolutionary hypotheses for human childhood". Yearbook of Physical Anthropology. 104: 63-89 abstract
- Gluckman PD, Hanson MA (2006). "Evolution, development and timing of puberty". Trends in Endocrinology and Metabolism. 17 (1): 7–12. doi:10.1016/j.tem.2005.11.006. PMID 16311040. S2CID 26141301.
- Kuhle BX (August 2007). "An evolutionary perspective on the origin and ontogeny of menopause". Maturitas. 57 (4): 329–37. doi:10.1016/j.maturitas.2007.04.004. PMID 17544235.
- Profet M (September 1993). "Menstruation as a defense against pathogens transported by sperm". The Quarterly Review of Biology. 68 (3): 335–86. doi:10.1086/418170. PMID 8210311. S2CID 23738569.
- Strassmann BI (June 1996). "The evolution of endometrial cycles and menstruation". The Quarterly Review of Biology. 71 (2): 181–220. doi:10.1086/419369. PMID 8693059. S2CID 6207295.
- Finn CA (1998). "Menstruation: A nonadaptive consequence of uterine evolution". The Quarterly Review of Biology. 73 (2): 163–173. doi:10.1086/420183. PMID 9618925. S2CID 25135630.
- Flaxman SM, Sherman PW (June 2000). "Morning sickness: a mechanism for protecting mother and embryo". The Quarterly Review of Biology. 75 (2): 113–48. doi:10.1086/393377. PMID 10858967. S2CID 28668687.
- Flaxman SM, Sherman PW (July 2008). "Morning sickness: adaptive cause or nonadaptive consequence of embryo viability?". The American Naturalist. 172 (1): 54–62. doi:10.1086/588081. PMID 18500939. S2CID 43837203.
- Wick G, Perschinka H, Millonig G (December 2001). "Atherosclerosis as an autoimmune disease: an update". Trends in Immunology. 22 (12): 665–9. doi:10.1016/S1471-4906(01)02089-0. PMID 11738996.
- Williams G, Nesse RM (1996). "Evolution and healing". Why We Get Sick: the new science of Darwinian medicine. New York: Vintage Books. pp. 37–8. ISBN 978-0-679-74674-4.
- Rotter JI, Diamond JM (1987). "What maintains the frequencies of human genetic diseases?". Nature. 329 (6137): 289–90. Bibcode:1987Natur.329..289R. doi:10.1038/329289a0. PMID 3114647. S2CID 4249162.
- Kaifu Y, Kasai K, Townsend GC, Richards LC (2003). "Tooth wear and the "design" of the human dentition: a perspective from evolutionary medicine". American Journal of Physical Anthropology. Suppl 37: 47–61. doi:10.1002/ajpa.10329. PMID 14666533. S2CID 907093.
- Neel JV (December 1962). "Diabetes mellitus: a "thrifty" genotype rendered detrimental by "progress"?". American Journal of Human Genetics. 14 (4): 353–62. PMC 1932342. PMID 13937884.
- Neel JV, Weder AB, Julius S (1998). "Type II diabetes, essential hypertension, and obesity as "syndromes of impaired genetic homeostasis": the "thrifty genotype" hypothesis enters the 21st century". Perspectives in Biology and Medicine. 42 (1): 44–74. doi:10.1353/pbm.1998.0060. PMID 9894356. S2CID 37780633.
- Wick G, Jansen-Dürr P, Berger P, Blasko I, Grubeck-Loebenstein B (February 2000). "Diseases of aging". Vaccine. 18 (16): 1567–83. doi:10.1016/S0264-410X(99)00489-2. PMID 10689131.
- Kluger MJ, Ringler DH, Anver MR (April 1975). "Fever and survival". Science. 188 (4184): 166–8. doi:10.1126/science.1114347. PMID 1114347. S2CID 35941390.
- Kluger MJ, Rothenburg BA (January 1979). "Fever and reduced iron: their interaction as a host defense response to bacterial infection". Science. 203 (4378): 374–6. Bibcode:1979Sci...203..374K. doi:10.1126/science.760197. PMID 760197.
- Ames BN, Cathcart R, Schwiers E, Hochstein P (November 1981). "Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: a hypothesis". Proceedings of the National Academy of Sciences of the United States of America. 78 (11): 6858–62. Bibcode:1981PNAS...78.6858A. doi:10.1073/pnas.78.11.6858. PMC 349151. PMID 6947260.
- Wander K, Shell-Duncan B, McDade TW (October 2008). "Evaluation of iron deficiency as a nutritional adaptation to infectious disease: an evolutionary medicine perspective". American Journal of Human Biology. 21 (2): 172–9. doi:10.1002/ajhb.20839. PMC 3938201. PMID 18949769.
- Eaton SB, Eaton SB, Konner MJ (April 1997). "Paleolithic nutrition revisited: a twelve-year retrospective on its nature and implications". European Journal of Clinical Nutrition. 51 (4): 207–16. doi:10.1038/sj.ejcn.1600389. PMID 9104571.
- Eaton SB, Konner M (January 1985). "Paleolithic nutrition. A consideration of its nature and current implications". The New England Journal of Medicine. 312 (5): 283–9. doi:10.1056/NEJM198501313120505. PMID 2981409.
- Woolf LI, McBean MS, Woolf FM, Cahalane SF (May 1975). "Phenylketonuria as a balanced polymorphism: the nature of the heterozygote advantage". Annals of Human Genetics. 38 (4): 461–9. doi:10.1111/j.1469-1809.1975.tb00635.x. PMID 1190737. S2CID 970755.
- Humphrey N (2002). "19. Great Expectations: The Evolutionary Psychology of Faith-Healing and the Placebo Effect" (PDF). The mind made flesh: essays from the frontiers of psychology and evolution. Oxford [Oxfordshire]: Oxford University Press. pp. 255–85. ISBN 978-0-19-280227-9.
- Karasik D (November 2008). "Osteoporosis: an evolutionary perspective". Human Genetics. 124 (4): 349–56. doi:10.1007/s00439-008-0559-8. PMID 18781328. S2CID 21475384.
- Williams TN (August 2006). "Human red blood cell polymorphisms and malaria". Current Opinion in Microbiology. 9 (4): 388–94. doi:10.1016/j.mib.2006.06.009. PMID 16815736.
- Ayi K, Turrini F, Piga A, Arese P (November 2004). "Enhanced phagocytosis of ring-parasitized mutant erythrocytes: a common mechanism that may explain protection against falciparum malaria in sickle trait and beta-thalassemia trait". Blood. 104 (10): 3364–71. doi:10.1182/blood-2003-11-3820. PMID 15280204.
- Williams TN, Mwangi TW, Wambua S, Alexander ND, Kortok M, Snow RW, Marsh K (July 2005). "Sickle cell trait and the risk of Plasmodium falciparum malaria and other childhood diseases". The Journal of Infectious Diseases. 192 (1): 178–86. doi:10.1086/430744. PMC 3545189. PMID 15942909.
- Hart BL (1988). "Biological basis of the behavior of sick animals". Neuroscience and Biobehavioral Reviews. 12 (2): 123–37. doi:10.1016/S0149-7634(88)80004-6. PMID 3050629. S2CID 17797005.
- Eaton SB, Pike MC, Short RV, Lee NC, Trussell J, Hatcher RA, Wood JW, Worthman CM, Jones NG, Konner MJ (September 1994). "Women's reproductive cancers in evolutionary context". The Quarterly Review of Biology. 69 (3): 353–67. doi:10.1086/418650. PMID 7972680. S2CID 23772025.
- Gaulin, Steven J. C. and Donald H. McBurney. Evolutionary psychology. Prentice Hall. 2003. ISBN 978-0-13-111529-3, Chapter 1, p 1-24.
- Buss, D.M. (2011). Evolutionary Psychology.
- Gaulin & McBurney (2004), Evolutionary Psychology
- Workman & Reader (2004), Evolutionary Psychology
- Nesse R (1997). "An evolutionary perspective on panic disorder and agoraphobia". In Baron-Cohen S (ed.). The maladapted mind: classic readings in evolutionary psychopathology. East Sussex: Psychology Press. pp. 73–84. ISBN 978-0-86377-460-7. Retrieved 21 January 2011.
- Grinde B (June 2005). "An approach to the prevention of anxiety-related disorders based on evolutionary medicine". Preventive Medicine. 40 (6): 904–9. doi:10.1016/j.ypmed.2004.08.001. PMID 15850894.
- Nesse RM (January 2000). "Is depression an adaptation?". Archives of General Psychiatry. 57 (1): 14–20. CiteSeerX 10.1.1.318.2659. doi:10.1001/archpsyc.57.1.14. PMID 10632228.
- Nesse RM, Berridge KC (October 1997). "Psychoactive drug use in evolutionary perspective". Science. 278 (5335): 63–6. doi:10.1126/science.278.5335.63. PMID 9311928. S2CID 24161553.
- Crow TJ (July 1995). "A Darwinian approach to the origins of psychosis". The British Journal of Psychiatry. 167 (1): 12–25. doi:10.1192/bjp.167.1.12. PMID 7551604. S2CID 40054545.
- Brüne M (March 2004). "Schizophrenia-an evolutionary enigma?". Neuroscience and Biobehavioral Reviews. 28 (1): 41–53. doi:10.1016/j.neubiorev.2003.10.002. PMID 15036932. S2CID 3191985.
- Nesse RM (September 2004). "Natural selection and the elusiveness of happiness". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 359 (1449): 1333–47. doi:10.1098/rstb.2004.1511. PMC 1693419. PMID 15347525.
- Weiner H (1 July 1998). "Notes on an evolutionary medicine". Psychosomatic Medicine. 60 (4): 510–20. doi:10.1097/00006842-199807000-00020. PMID 9710299. S2CID 42597661.
- Tinbergen N (1963). "On Aims and Methods in Ethology" (PDF). Zeitschrift für Tierpsychologie. 20 (4): 410–433. doi:10.1111/j.1439-0310.1963.tb01161.x.
- Nesse RM (December 2008). "Evolution: medicine's most basic science". Lancet. 372 (Suppl 1): S21–7. doi:10.1016/S0140-6736(08)61877-2. S2CID 15306192.
- Ewald PW (September 1980). "Evolutionary biology and the treatment of signs and symptoms of infectious disease". Journal of Theoretical Biology. 86 (1): 169–76. Bibcode:1980JThBi..86..169E. doi:10.1016/0022-5193(80)90073-9. PMID 7464170.
Further reading
Books
- Williams G, Nesse RM (1996). Why We Get Sick: the new science of Darwinian medicine. New York: Vintage Books. ISBN 978-0-679-74674-4.
- Stearns SC, Koella JK (2008). Evolution in health and disease (2nd ed.). Oxford [Oxfordshire]: Oxford University Press. ISBN 978-0-19-920745-9.
- McKenna JJ, Trevathan W, Smith EO (2008). Evolutionary medicine and health: new perspectives (2nd ed.). Oxford [Oxfordshire]: Oxford University Press. ISBN 978-0-19-530706-1.
- O'Higgins P, Elton S (2008). Medicine and Evolution: Current Applications, Future Prospects (Society for the Study of Human Biology Symposium Series (Sshb). Boca Raton: CRC. ISBN 978-1-4200-5134-6.
- Ewald, P. W. (1996). Evolution of Infectious Disease. Oxford: Oxford University Press. ISBN 978-0-19-511139-2.
- Moalem S, Prince J (2007). Survival of the Sickest. New York: HarperLuxe. ISBN 978-0-06-088965-4.
Online articles
- Straub RH, Besedovsky HO (December 2003). "Integrated evolutionary, immunological, and neuroendocrine framework for the pathogenesis of chronic disabling inflammatory diseases". FASEB Journal. 17 (15): 2176–83. doi:10.1096/fj.03-0433hyp. PMID 14656978. S2CID 24742889.
- Straub RH (May 2012). "Evolutionary medicine and chronic inflammatory state--known and new concepts in pathophysiology". Journal of Molecular Medicine. 90 (5): 523–34. doi:10.1007/s00109-012-0861-8. PMC 3354326. PMID 22271169.
- LeGrand EK, Brown CC (July 2002). "Darwinian medicine: applications of evolutionary biology for veterinarians". The Canadian Veterinary Journal. 43 (7): 556–9. PMC 341948. PMID 12125190.
- Nesse RM, Stearns SC (February 2008). "The great opportunity: Evolutionary applications to medicine and public health" (PDF). Evolutionary Applications. 1 (1): 28–48. doi:10.1111/j.1752-4571.2007.00006.x. PMC 3352398. PMID 25567489. Archived from the original (PDF) on 2009-01-16.
- Naugler CT (September 2008). "Evolutionary medicine: update on the relevance to family practice". Canadian Family Physician. 54 (9): 1265–9. PMC 2553465. PMID 18791103.
- Childs B, Wiener C, Valle D (2005). "A science of the individual: implications for a medical school curriculum". Annual Review of Genomics and Human Genetics. 6 (1): 313–30. doi:10.1146/annurev.genom.6.080604.162345. PMID 16124864.
- Stiehm ER (January 2006). "Disease versus disease: how one disease may ameliorate another". Pediatrics. 117 (1): 184–91. doi:10.1542/peds.2004-2773. PMID 16396876. S2CID 20493524.
External links
Evolutionary psychology | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||
| Processes |
| ||||||||||
| Areas |
| ||||||||||
| People |
| ||||||||||
| Research centers/ organizations |
| ||||||||||
| Publications |
| ||||||||||
| Related subjects |
| ||||||||||
| |||||||||||