History of medicine
The history of medicine is a both a study of medicine throughout history as well as a multidisciplinary field of study that seeks to explore and understand medical practices, both past and present, throughout human societies.[1]



_Brockenhurst_(operation_theatre).jpg.webp)
.jpg.webp)

More than just history and medicine, this field of study incorporates learnings from across disciplines such as anthropology, economics, health sciences, sociology, and politics to better understand the institutions, practices, people, professions, and social systems that have influenced and shaped medicine throughout the ages.[1][2]
As a documentation of medicine over time, the history of medicine shows how societies have changed in their approach to illness and disease from ancient times to the present. Early medical traditions include those of Babylon, China, Egypt and India. The Hippocratic Oath was written in ancient Greece in the 5th century BCE, and is a direct inspiration for oaths of office that physicians swear upon entry into the profession today. In the Middle Ages, surgical practices inherited from the ancient masters were improved and then systematized in Rogerius's The Practice of Surgery. Universities began systematic training of physicians around 1220 CE in Italy.
Invention of the microscope was a consequence of improved understanding, during the Renaissance. Prior to the 19th century, humorism (also known as humoralism) was thought to explain the cause of disease but it was gradually replaced by the germ theory of disease, leading to effective treatments and even cures for many infectious diseases. Military doctors advanced the methods of trauma treatment and surgery. Public health measures were developed especially in the 19th century as the rapid growth of cities required systematic sanitary measures. Advanced research centers opened in the early 20th century, often connected with major hospitals. The mid-20th century was characterized by new biological treatments, such as antibiotics. These advancements, along with developments in chemistry, genetics, and radiography led to modern medicine. Medicine was heavily professionalized in the 20th century, and new careers opened to women as nurses (from the 1870s) and as physicians (especially after 1970).
Prehistoric medicine
Although there is little record to establish when plants were first used for medicinal purposes (herbalism), the use of plants as healing agents, as well as clays and soils is ancient. Over time, through emulation of the behavior of fauna, a medicinal knowledge base developed and passed between generations. Even earlier, Neanderthals may have engaged in medical practices.[3] As tribal culture specialized specific castes, shamans and apothecaries fulfilled the role of healer.[4] The first known dentistry dates to c. 7000 BCE in Baluchistan where Neolithic dentists used flint-tipped drills and bowstrings.[5] The first known trepanning operation was carried out c. 5000 BCE in Ensisheim, France.[6] A possible amputation was carried out c. 4,900 BCE in Buthiers-Bulancourt, France.[7]
Ancient medicine
Places
Ancient China

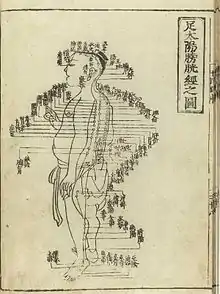
China also developed a large body of traditional medicine. Much of the philosophy of traditional Chinese medicine derived from empirical observations of disease and illness by Taoist physicians and reflects the classical Chinese belief that individual human experiences express causative principles effective in the environment at all scales. These causative principles, whether material, essential, or mystical, correlate as the expression of the natural order of the universe.
The foundational text of Chinese medicine is the Huangdi neijing, (or Yellow Emperor's Inner Canon), written 5th century to 3rd century BCE.[8] Near the end of the 2nd century CE, during the Han dynasty, Zhang Zhongjing, wrote a Treatise on Cold Damage, which contains the earliest known reference to the Neijing Suwen. The Jin dynasty practitioner and advocate of acupuncture and moxibustion, Huangfu Mi (215–282), also quotes the Yellow Emperor in his Jiayi jing, c. 265. During the Tang dynasty, the Suwen was expanded and revised and is now the best extant representation of the foundational roots of traditional Chinese medicine. Traditional Chinese medicine that is based on the use of herbal medicine, acupuncture, massage and other forms of therapy has been practiced in China for thousands of years.
In the 18th century, during the Qing dynasty, there was a proliferation of popular books as well as more advanced encyclopedias on traditional medicine. Jesuit missionaries introduced Western science and medicine to the royal court, although the Chinese physicians ignored them.[9]
Finally in the 19th century, Western medicine was introduced at the local level by Christian medical missionaries from the London Missionary Society (Britain), the tMethodist Church (Britain) and the Presbyterian Church (US). Benjamin Hobson (1816–1873) in 1839, set up a highly successful Wai Ai Clinic in Guangzhou, China.[10] The Hong Kong College of Medicine for Chinese was founded in 1887 by the London Missionary Society, with its first graduate (in 1892) being Sun Yat-sen, who later led the Chinese Revolution (1911). The Hong Kong College of Medicine for Chinese was the forerunner of the School of Medicine of the University of Hong Kong, which started in 1911.
Because of the social custom that men and women should not be near to one another, the women of China were reluctant to be treated by male doctors. The missionaries sent women doctors such as Dr. Mary Hannah Fulton (1854–1927). Supported by the Foreign Missions Board of the Presbyterian Church (US) she in 1902 founded the first medical college for women in China, the Hackett Medical College for Women, in Guangzhou.[11]
Historiography of Chinese medicine
When reading the Chinese classics, it is important for scholars to examine these works from the Chinese perspective. Historians have noted two key aspects of Chinese medical history: understanding conceptual differences when translating the term 身, and observing the history from the perspective of cosmology rather than biology.[12]: 19
In Chinese classical texts, the term 身 is the closest historical translation to the English word "body" because it sometimes refers to the physical human body in terms of being weighed or measured, but the term is to be understood as an "ensemble of functions" encompassing both the human psyche and emotions. This concept of the human body is opposed to the European duality of a separate mind and body.[12]: 19–20 It is critical for scholars to understand the fundamental differences in concepts of the body in order to connect the medical theory of the classics to the "human organism" it is explaining.[12]: 20
Chinese scholars established a correlation between the cosmos and the "human organism." The basic components of cosmology, qi, yin yang and the Five Phase theory, were used to explain health and disease in texts such as Huangdi neijing.[12]: 21 Yin and yang are the changing factors in cosmology, with qi as the vital force or energy of life. The Five Phase theory Wu Xing of the Han dynasty contains the elements wood, fire, earth, metal, and water. By understanding medicine from a cosmology perspective, historians better understand Chinese medical and social classifications such as gender, which was defined by a domination or remission of yang in terms of yin.
These two distinctions are imperative when analyzing the history of traditional Chinese medical science.
A majority of Chinese medical history written after the classical canons comes in the form of primary source case studies where academic physicians record the illness of a particular person and the healing techniques used, as well as their effectiveness.[12]: 225 Historians have noted that Chinese scholars wrote these studies instead of "books of prescriptions or advice manuals;" in their historical and environmental understanding, no two illnesses were alike so the healing strategies of the practitioner was unique every time to the specific diagnosis of the patient.[12]: 226–27 Medical case studies existed throughout Chinese history, but "individually authored and published case history" was a prominent creation of the Ming dynasty.[12]: 225 An example such case studies would be the literati physician, Cheng Congzhou, collection of 93 cases published in 1644.[12]: 226–27
Ancient India

The Atharvaveda, a sacred text of Hinduism dating from the Early Iron Age, is one of the first Indian texts dealing with medicine. The Atharvaveda also contains prescriptions of herbs for various ailments. The use of herbs to treat ailments would later form a large part of Ayurveda.
Ayurveda, meaning the "complete knowledge for long life" is another medical system of India. Its two most famous texts belong to the schools of Charaka and Sushruta. The earliest foundations of Ayurveda were built on a synthesis of traditional herbal practices together with a massive addition of theoretical conceptualizations, new nosologies and new therapies dating from about 600 BCE onwards, and coming out of the communities of thinkers which included the Buddha and others.[13]
According to the compendium of Charaka, the Charakasamhitā, health and disease are not predetermined and life may be prolonged by human effort. The compendium of Suśruta, the Suśrutasamhitā defines the purpose of medicine to cure the diseases of the sick, protect the healthy, and to prolong life. Both these ancient compendia include details of the examination, diagnosis, treatment, and prognosis of numerous ailments. The Suśrutasamhitā is notable for describing procedures on various forms of surgery, including rhinoplasty, the repair of torn ear lobes, perineal lithotomy, cataract surgery, and several other excisions and other surgical procedures. Most remarkable was Susruta's surgery specially the rhinoplasty for which he is called father of modern plastic surgery. Susruta also described more than 125 surgical instruments in detail. Also remarkable is Sushruta's penchant for scientific classification: His medical treatise consists of 184 chapters, 1,120 conditions are listed, including injuries and illnesses relating to aging and mental illness.
The Ayurvedic classics mention eight branches of medicine: kāyācikitsā (internal medicine), śalyacikitsā (surgery including anatomy), śālākyacikitsā (eye, ear, nose, and throat diseases), kaumārabhṛtya (pediatrics with obstetrics and gynaecology), bhūtavidyā (spirit and psychiatric medicine), agada tantra (toxicology with treatments of stings and bites), rasāyana (science of rejuvenation), and vājīkaraṇa (aphrodisiac and fertility). Apart from learning these, the student of Āyurveda was expected to know ten arts that were indispensable in the preparation and application of his medicines: distillation, operative skills, cooking, horticulture, metallurgy, sugar manufacture, pharmacy, analysis and separation of minerals, compounding of metals, and preparation of alkalis. The teaching of various subjects was done during the instruction of relevant clinical subjects. For example, the teaching of anatomy was a part of the teaching of surgery, embryology was a part of training in pediatrics and obstetrics, and the knowledge of physiology and pathology was interwoven in the teaching of all the clinical disciplines. The normal length of the student's training appears to have been seven years. But the physician was to continue to learn.[14]
As an alternative form of medicine in India, Unani medicine found deep roots and royal patronage during medieval times. It progressed during the Indian sultanate and mughal periods. Unani medicine is very close to Ayurveda. Both are based on the theory of the presence of the elements (in Unani, they are considered to be fire, water, earth, and air) in the human body. According to followers of Unani medicine, these elements are present in different fluids and their balance leads to health and their imbalance leads to illness.[15]
By the 18th century CE, Sanskrit medical wisdom still dominated. Muslim rulers built large hospitals in 1595 in Hyderabad, and in Delhi in 1719, and numerous commentaries on ancient texts were written.[16]
Places
Ancient Egypt

Ancient Egypt developed a large, varied and fruitful medical tradition. Herodotus described the Egyptians as "the healthiest of all men, next to the Libyans",[17] because of the dry climate and the notable public health system that they possessed. According to him, "the practice of medicine is so specialized among them that each physician is a healer of one disease and no more." Although Egyptian medicine, to a considerable extent, dealt with the supernatural,[18] it eventually developed a practical use in the fields of anatomy, public health, and clinical diagnostics.
Medical information in the Edwin Smith Papyrus may date to a time as early as 3000 BCE.[19] Imhotep in the 3rd dynasty is sometimes credited with being the founder of ancient Egyptian medicine and with being the original author of the Edwin Smith Papyrus, detailing cures, ailments and anatomical observations. The Edwin Smith Papyrus is regarded as a copy of several earlier works and was written c. 1600 BCE. It is an ancient textbook on surgery almost completely devoid of magical thinking and describes in exquisite detail the examination, diagnosis, treatment, and prognosis of numerous ailments.[20]
The Kahun Gynaecological Papyrus[21] treats women's complaints, including problems with conception. Thirty four cases detailing diagnosis and[22] treatment survive, some of them fragmentarily.[23] Dating to 1800 BCE, it is the oldest surviving medical text of any kind.
Medical institutions, referred to as Houses of Life are known to have been established in ancient Egypt as early as 2200 BCE.[24]
The Ebers Papyrus is the oldest written text mentioning enemas. Many medications were administered by enemas and one of the many types of medical specialists was an Iri, the Shepherd of the Anus.[25]
The earliest known physician is also credited to ancient Egypt: Hesy-Ra, "Chief of Dentists and Physicians" for King Djoser in the 27th century BCE.[26] Also, the earliest known woman physician, Peseshet, practiced in Ancient Egypt at the time of the 4th dynasty. Her title was "Lady Overseer of the Lady Physicians."[27]
Mesopotamia
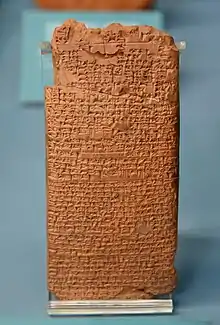
The ancient Mesopotamians had no distinction between "rational science" and magic.[30][31][32] When a person became ill, doctors would prescribe both magical formulas to be recited as well as medicinal treatments.[30][31][32][29] The earliest medical prescriptions appear in Sumerian during the Third Dynasty of Ur (c. 2112 BCE – c. 2004 BCE).[33] The oldest Babylonian texts on medicine date back to the Old Babylonian period in the first half of the 2nd millennium BCE.[34] The most extensive Babylonian medical text, however, is the Diagnostic Handbook written by the ummânū, or chief scholar, Esagil-kin-apli of Borsippa,[35]: 99 [36] during the reign of the Babylonian king Adad-apla-iddina (1069–1046 BCE).[37] Along with the Egyptians, the Babylonians introduced the practice of diagnosis, prognosis, physical examination, and remedies. In addition, the Diagnostic Handbook introduced the methods of therapy and cause. The text contains a list of medical symptoms and often detailed empirical observations along with logical rules used in combining observed symptoms on the body of a patient with its diagnosis and prognosis.[35]: 97–98 The Diagnostic Handbook was based on a logical set of axioms and assumptions, including the modern view that through the examination and inspection of the symptoms of a patient, it is possible to determine the patient's disease, its cause and future development, and the chances of the patient's recovery. The symptoms and diseases of a patient were treated through therapeutic means such as bandages, herbs and creams.[35]: 99
In East Semitic cultures, the main medicinal authority was a kind of exorcist-healer known as an āšipu.[30][31][32] The profession was generally passed down from father to son[30] and was held in extremely high regard.[30] Of less frequent recourse was another kind of healer known as an asu, who corresponds more closely to a modern physician[29] and treated physical symptoms using primarily folk remedies composed of various herbs, animal products, and minerals, as well as potions, enemas, and ointments or poultices.[29] These physicians, who could be either male or female, also dressed wounds, set limbs, and performed simple surgeries.[29] The ancient Mesopotamians also practiced prophylaxis[29] and took measures to prevent the spread of disease.[29]
Mental illnesses were well known in ancient Mesopotamia,[38] where diseases and mental disorders were believed to be caused by specific deities.[28] Because hands symbolized control over a person, mental illnesses were known as "hands" of certain deities.[28] One psychological illness was known as Qāt Ištar, meaning "Hand of Ishtar".[28] Others were known as "Hand of Shamash", "Hand of the Ghost", and "Hand of the God".[28] Descriptions of these illnesses, however, are so vague that it is usually impossible to determine which illnesses they correspond to in modern terminology.[28] Mesopotamian doctors kept detailed record of their patients' hallucinations and assigned spiritual meanings to them.[38] A patient who hallucinated that he was seeing a dog was predicted to die;[38] whereas, if he saw a gazelle, he would recover.[38] The royal family of Elam was notorious for its members frequently suffering from insanity.[38] Erectile dysfunction was recognized as being rooted in psychological problems.[38]
Ideas
Humors

The theory of humors was derived from ancient medical works, dominated western medicine until the 19th century, and is credited to Greek philosopher and surgeon Galen of Pergamon (129–c. 216 BCE).[39] In Greek medicine, there are thought to be four humors, or bodily fluids that are linked to illness: blood, phlegm, yellow bile, and black bile.[40] Early scientists believed that food is digested into blood, muscle, and bones, while the humors that weren't blood were then formed by indigestible materials that are left over. An excess or shortage of any one of the four humors is theorized to cause an imbalance that results in sickness; the aforementioned statement was hypothesized by sources before Hippocrates.[40] Hippocrates (c. 400 BCE) deduced that the four seasons of the year and four ages of man that affect the body in relation to the humors.[39] The four ages of man are childhood, youth, prime age, and old age.[40] The four humors as associated with the four seasons are black bile – autumn, yellow bile – summer, phlegm – winter and blood – spring.[41]
In De temperamentis, Galen linked what he called temperaments, or personality characteristics, to a person's natural mixture of humors. He also said that the best place to check the balance of temperaments was in the palm of the hand. A person that is considered to be phlegmatic is said to be an introvert, even-tempered, calm, and peaceful.[40] This person would have an excess of phlegm, which is described as a viscous substance or mucous.[42] Similarly, a melancholic temperament related to being moody, anxious, depressed, introverted, and pessimistic.[40] A melancholic temperament is caused by an excess of black bile, which is sedimentary and dark in color.[42] Being extroverted, talkative, easygoing, carefree, and sociable coincides with a sanguine temperament, which is linked to too much blood.[40] Finally, a choleric temperament is related to too much yellow bile, which is actually red in color and has the texture of foam; it is associated with being aggressive, excitable, impulsive, and also extroverted.
There are numerous ways to treat a disproportion of the humors. For example, if someone was suspected to have too much blood, then the physician would perform bloodletting as a treatment. Likewise, if a person that had too much phlegm would feel better after expectorating, and someone with too much yellow bile would purge.[42] Another factor to be considered in the balance of humors is the quality of air in which one resides, such as the climate and elevation. Also, the standard of food and drink, balance of sleeping and waking, exercise and rest, retention and evacuation are important. Moods such as anger, sadness, joy, and love can affect the balance. During that time, the importance of balance was demonstrated by the fact that women lose blood monthly during menstruation, and have a lesser occurrence of gout, arthritis, and epilepsy then men do.[42] Galen also hypothesized that there are three faculties. The natural faculty affects growth and reproduction and is produced in the liver. Animal or vital faculty controls respiration and emotion, coming from the heart. In the brain, the psychic faculty commands the senses and thought.[42] The structure of bodily functions is related to the humors as well. Greek physicians understood that food was cooked in the stomach; this is where the nutrients are extracted. The best, most potent and pure nutrients from food are reserved for blood, which is produced in the liver and carried through veins to organs. Blood enhanced with pneuma, which means wind or breath, is carried by the arteries.[40] The path that blood take is as follows: venous blood passes through the vena cava and is moved into the right ventricle of the heart; then, the pulmonary artery takes it to the lungs.[42] Later, the pulmonary vein then mixes air from the lungs with blood to form arterial blood, which has different observable characteristics.[40] After leaving the liver, half of the yellow bile that is produced travels to the blood, while the other half travels to the gallbladder. Similarly, half of the black bile produced gets mixed in with blood, and the other half is used by the spleen.[42]
Places
Ancient Greek medicine
Around 800 BCE Homer in the Iliad gives descriptions of wound treatment by the two sons of Asklepios, the admirable physicians Podaleirius and Machaon and one acting doctor, Patroclus. Because Machaon is wounded and Podaleirius is in combat Eurypylus asks Patroclus to "cut out the arrow-head, and wash the dark blood from my thigh with warm water, and sprinkle soothing herbs with power to heal on my wound".[43] Asklepios, like Imhotep, came to be associated as a god of healing over time.

Temples dedicated to the healer-god Asclepius, known as Asclepieia (Ancient Greek: Ἀσκληπιεῖα, sing. Ἀσκληπιεῖον, Asclepieion), functioned as centers of medical advice, prognosis, and healing.[44] At these shrines, patients would enter a dream-like state of induced sleep known as enkoimesis (ἐγκοίμησις) not unlike anesthesia, in which they either received guidance from the deity in a dream or were cured by surgery.[45] Asclepeia provided carefully controlled spaces conducive to healing and fulfilled several of the requirements of institutions created for healing.[44] In the Asclepeion of Epidaurus, three large marble boards dated to 350 BCE preserve the names, case histories, complaints, and cures of about 70 patients who came to the temple with a problem and shed it there. Some of the surgical cures listed, such as the opening of an abdominal abscess or the removal of traumatic foreign material, are realistic enough to have taken place, but with the patient in a state of enkoimesis induced with the help of soporific substances such as opium.[45] Alcmaeon of Croton wrote on medicine between 500 and 450 BCE. He argued that channels linked the sensory organs to the brain, and it is possible that he discovered one type of channel, the optic nerves, by dissection.[46]
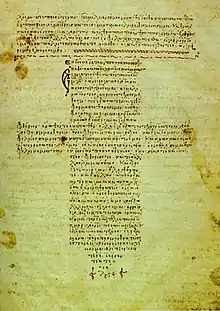
Hippocrates of Kos (c. 460 – c. 370 BCE), considered the "father of modern medicine."[47][48] The Hippocratic Corpus is a collection of around seventy early medical works from ancient Greece strongly associated with Hippocrates and his students. Most famously, the Hippocratics invented the Hippocratic Oath for physicians. Contemporary physicians swear an oath of office which includes aspects found in early editions of the Hippocratic Oath.
Hippocrates and his followers were first to describe many diseases and medical conditions. Though humorism (humoralism) as a medical system predates 5th-century Greek medicine, Hippocrates and his students systematized the thinking that illness can be explained by an imbalance of blood, phlegm, black bile, and yellow bile.[49] Hippocrates is given credit for the first description of clubbing of the fingers, an important diagnostic sign in chronic suppurative lung disease, lung cancer and cyanotic heart disease. For this reason, clubbed fingers are sometimes referred to as "Hippocratic fingers".[50] Hippocrates was also the first physician to describe the Hippocratic face in Prognosis. Shakespeare famously alludes to this description when writing of Falstaff's death in Act II, Scene iii. of Henry V.[51] Hippocrates began to categorize illnesses as acute, chronic, endemic and epidemic, and use terms such as, "exacerbation, relapse, resolution, crisis, paroxysm, peak, and convalescence."[52][53]
The Greek Galen (c. 129–216 CE) was one of the greatest physicians of the ancient world, as his theories dominated all medical studies for nearly 1500 years.[54] His theories and experimentation laid the foundation for modern medicine surrounding the heart and blood. Galen's influence and innovations in medicine can be attributed to the experiments he conducted, which were unlike any other medical experiments of his time. Galen strongly believed that medical dissection was one of the essential procedures in truly understanding medicine. He began to dissect different animals that were anatomically similar to humans, which allowed him to learn more about the internal organs and extrapolate the surgical studies to the human body.[54] In addition, he performed many audacious operations—including brain and eye surgeries—that were not tried again for almost two millennia. Through the dissections and surgical procedures, Galen concluded that blood is able to circulate throughout the human body, and the heart is most similar to the human soul.[54][55] In Ars medica ("Arts of Medicine"), he further explains the mental properties in terms of specific mixtures of the bodily organs.[56][57] While much of his work surrounded the physical anatomy, he also worked heavily in humoral physiology.
Galen's medical work was regarded as authoritative until well into the Middle Ages. He left a physiological model of the human body that became the mainstay of the medieval physician's university anatomy curriculum. Although he attempted to extrapolate the animal dissections towards the model of the human body, some of Galen's theories were incorrect. This caused his model to suffer greatly from stasis and intellectual stagnation.[58] Greek and Roman taboos caused dissection of the human body to usually be banned in ancient times, but in the Middle Ages it changed.[59][60]
In 1523 Galen's On the Natural Faculties was published in London. In the 1530s Belgian anatomist and physician Andreas Vesalius launched a project to translate many of Galen's Greek texts into Latin. Vesalius's most famous work, De humani corporis fabrica was greatly influenced by Galenic writing and form.
Ancient Roman medicine
The Romans invented numerous surgical instruments, including the first instruments unique to women,[61] as well as the surgical uses of forceps, scalpels, cautery, cross-bladed scissors, the surgical needle, the sound, and speculas.[62][63] Romans also performed cataract surgery.[64]
The Roman army physician Dioscorides (c. 40–90 CE), was a Greek botanist and pharmacologist. He wrote the encyclopedia De Materia Medica describing over 600 herbal cures, forming an influential pharmacopoeia which was used extensively for the following 1,500 years.[65]
Early Christians in the Roman Empire incorporated medicine into their theology, ritual practices, and metaphors.[66]
People
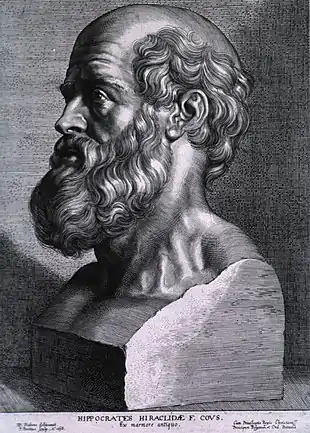 Hippocrates (c. 460 - 370 BCE). Known as the "father of medicine".
Hippocrates (c. 460 - 370 BCE). Known as the "father of medicine". Galen (129 - 216 CE). Known for their wide insights into anatomy.
Galen (129 - 216 CE). Known for their wide insights into anatomy.
Herophilus and Erasistratus
Two great Alexandrians laid the foundations for the scientific study of anatomy and physiology, Herophilus of Chalcedon and Erasistratus of Ceos.[68] Other Alexandrian surgeons gave us ligature (hemostasis), lithotomy, hernia operations, ophthalmic surgery, plastic surgery, methods of reduction of dislocations and fractures, tracheotomy, and mandrake as an anaesthetic. Some of what we know of them comes from Celsus and Galen of Pergamum.[69]
Herophilus of Chalcedon, the renowned Alexandrian physician, was one of the pioneers of human anatomy. Though his knowledge of the anatomical structure of the human body was vast, he specialized in the aspects of neural anatomy.[70] Thus, his experimentation was centered around the anatomical composition of the blood-vascular system and the pulsations that can be analyzed from the system.[70] Furthermore, the surgical experimentation he administered caused him to become very prominent throughout the field of medicine, as he was one of the first physicians to initiate the exploration and dissection of the human body.[71]
The banned practice of human dissection was lifted during his time within the scholastic community. This brief moment in the history of Greek medicine allowed him to further study the brain, which he believed was the core of the nervous system.[71] He also distinguished between veins and arteries, noting that the latter pulse and the former do not. Thus, while working at the medical school of Alexandria, Herophilus placed intelligence in the brain based on his surgical exploration of the body, and he connected the nervous system to motion and sensation. In addition, he and his contemporary, Erasistratus of Chios, continued to research the role of veins and nerves. After conducting extensive research, the two Alexandrians mapped out the course of the veins and nerves across the human body. Erasistratus connected the increased complexity of the surface of the human brain compared to other animals to its superior intelligence. He sometimes employed experiments to further his research, at one time repeatedly weighing a caged bird, and noting its weight loss between feeding times.[72] In Erasistratus' physiology, air enters the body, is then drawn by the lungs into the heart, where it is transformed into vital spirit, and is then pumped by the arteries throughout the body. Some of this vital spirit reaches the brain, where it is transformed into animal spirit, which is then distributed by the nerves.[72]
5th to 15th century medicine

Places
Byzantine medicine
Byzantine medicine encompasses the common medical practices of the Byzantine Empire from about 400 CE to 1453 CE. Byzantine medicine was notable for building upon the knowledge base developed by its Greco-Roman predecessors. In preserving medical practices from antiquity, Byzantine medicine influenced Islamic medicine as well as fostering the Western rebirth of medicine during the Renaissance.
Byzantine physicians often compiled and standardized medical knowledge into textbooks. Their records tended to include both diagnostic explanations and technical drawings. The Medical Compendium in Seven Books, written by the leading physician Paul of Aegina, survived as a particularly thorough source of medical knowledge. This compendium, written in the late seventh century, remained in use as a standard textbook for the following 800 years.
Late antiquity ushered in a revolution in medical science, and historical records often mention civilian hospitals (although battlefield medicine and wartime triage were recorded well before Imperial Rome). Constantinople stood out as a center of medicine during the Middle Ages, which was aided by its crossroads location, wealth, and accumulated knowledge.
The first ever known example of separating conjoined twins occurred in the Byzantine Empire in the 10th century. The next example of separating conjoined twins will be first recorded many centuries later in Germany in 1689.[73][74]
The Byzantine Empire's neighbors, the Persian Sassanid Empire, also made their noteworthy contributions mainly with the establishment of the Academy of Gondeshapur, which was "the most important medical center of the ancient world during the 6th and 7th centuries."[75] In addition, Cyril Elgood, British physician and a historian of medicine in Persia, commented that thanks to medical centers like the Academy of Gondeshapur, "to a very large extent, the credit for the whole hospital system must be given to Persia."[76]
Islamic medicine
The Islamic civilization rose to primacy in medical science as its physicians contributed significantly to the field of medicine, including anatomy, ophthalmology, pharmacology, pharmacy, physiology, and surgery. Islamic civilization's contribution to these fields within medicine was a gradual process that took hundreds of years. During the time of the first great Muslim dynasty, the Umayyad Caliphate (661-750 CE), these fields that were in their very early stages of development, and not much progress was made.[77] One reason for the limited advancement in medicine during the Umayyad Caliphate was the Caliphate's focus on expansion after the death of Prophet Muhammad (632 CE).[78] The focus on expansionism redirected resources from other fields, such as medicine. The priority on these factors led a dense amount of the population to believe that God will provide cures for their illnesses and diseases because of the attention on spirituality.[78]
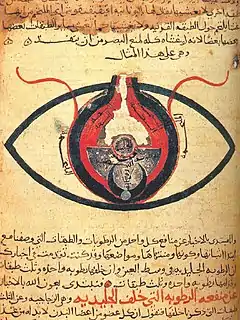
There were also many other areas of interest during that time before there was a rising interest in the field of medicine. Abd al-Malik ibn Marwan, the fifth caliph of the Umayyad, developed governmental administration, adopted Arabic as the main language, and focused on many other areas.[79] However, this rising interest in Islamic medicine grew significantly when the Abbasid Caliphate (750-1258 CE) overthrew the Umayyad Caliphate in 750 CE.[80] This change in dynasty from the Umayyad Caliphate to the Abbasid Caliphate served as a turning point towards scientific and medical developments. A big contributor to this is because, under Abbasid rule, there was a great part of the Greek legacy that was transmitted into Arabic which by then, was the main language of Islamic nations.[78] Because of this, many Islamic physicians were heavily influenced by the works of Greek scholars of Alexandria and Egypt and were able to further expand on those texts to produce new medical pieces of knowledge.[81] This period of time is also known as the Islamic Golden Age where there was a period of development for development and flourishments of technology, commerce, and sciences including medicine. Additionally, during this time the creation of the first Islamic Hospital in 805 CE by the Abbasid caliph Harun al-Rashid in Baghdad was recounted as a glorious event of the Golden Age.[77] This hospital in Baghdad contributed immensely to Baghdad's success and also provided educational opportunities for Islamic physicians. During the Islamic Golden Age, there were many famous Islamic physicians that paved the way for medical advancements and understandings. Muhammad ibn Zakariya al-Razi (965-1040 CE), sometimes referred to as the father of modern optics, is the author of the monumental Book of Optics and also was known for his work in differentiating smallpox from measles.[82] However, this would not be possible without the influence from many different areas of the world that influenced the Arabs.
The Arabs were influenced by ancient Indian, Persian, Greek, Roman and Byzantine medical practices, and helped them develop further.[83]Galen & Hippocrates were pre-eminent authorities. The translation of 129 of Galen's works into Arabic by the Nestorian Christian Hunayn ibn Ishaq and his assistants, and in particular Galen's insistence on a rational systematic approach to medicine, set the template for Islamic medicine, which rapidly spread throughout the Arab Empire.[84] Its most famous physicians included the Persian polymaths Muhammad ibn Zakarīya al-Rāzi and Avicenna, who wrote more than 40 works on health, medicine, and well-being. Taking leads from Greece and Rome, Islamic scholars kept both the art and science of medicine alive and moving forward.[85] Persian polymath Avicenna has also been called the "father of medicine".[86] He wrote The Canon of Medicine which became a standard medical text at many medieval European universities,[87] considered one of the most famous books in the history of medicine.[88] The Canon of Medicine presents an overview of the contemporary medical knowledge of the medieval Islamic world, which had been influenced by earlier traditions including Greco-Roman medicine (particularly Galen),[89] Persian medicine, Chinese medicine and Indian medicine. Persian physician al-Rāzi[90] was one of the first to question the Greek theory of humorism, which nevertheless remained influential in both medieval Western and medieval Islamic medicine.[91] Some volumes of al-Rāzi's work Al-Mansuri, namely "On Surgery" and "A General Book on Therapy", became part of the medical curriculum in European universities.[92] Additionally, he has been described as a doctor's doctor,[93] the father of pediatrics,[94][95] and a pioneer of ophthalmology. For example, he was the first to recognize the reaction of the eye's pupil to light.[95]
In addition to contributions to humanity's understanding of human anatomy, Islamicate scientists and scholars, physicians specifically, played an invaluable role in the development of the modern hospital system, creating the foundations on which more contemporary medical professionals would build models of public health systems in Europe and elsewhere.[96] During the time of the Safavid empire (16th–18th centuries) in Iran and the Mughal empire (16th–19th centuries) in India, Muslim scholars radically transformed the institution of the hospital, creating an environment in which rapidly developing medical knowledge of the time could be passed among students and teachers from a wide range of cultures.[97] There were two main schools of thought with patient care at the time. These included humoral physiology from the Persians and Ayurvedic practice. After these theories were translated from Sanskrit to Persian and vice-versa, hospitals could have a mix of culture and techniques. This allowed for a sense of collaborative medicine. Hospitals became increasingly common during this period as wealthy patrons commonly founded them. Many features that are still in use today, such as an emphasis on hygiene, a staff fully dedicated to the care of patients, and separation of individual patients from each other were developed in Islamicate hospitals long before they came into practice in Europe.[98] At the time, the patient care aspects of hospitals in Europe had not taken effect. European hospitals were places of religion rather than institutions of science. As was the case with much of the scientific work done by Islamicate scholars, many of these novel developments in medical practice were transmitted to European cultures hundreds of years after they had long been utilized throughout the Islamicate world. Although Islamicate scientists were responsible for discovering much of the knowledge that allows the hospital system to function safely today, European scholars who built on this work still receive the majority of the credit historically.[96]
Before the development of scientific medical practices in the Islamicate empires, medical care was mainly performed by religious figures such as priests.[96] Without a profound understanding of how infectious diseases worked and why sickness spread from person to person, these early attempts at caring for the ill and injured often did more harm than good. Contrarily, with the development of new and safer practices by Islamicate scholars and physicians in Arabian hospitals, ideas vital for the effective care of patients were developed, learned, and transmitted widely. Hospitals developed novel "concepts and structures" which are still in use today: separate wards for male and female patients, pharmacies, medical record-keeping, and personal and institutional sanitation and hygiene.[96] Much of this knowledge was recorded and passed on through Islamicate medical texts, many of which were carried to Europe and translated for the use of European medical workers. The Tasrif, written by surgeon Abu Al-Qasim Al-Zahrawi, was translated into Latin; it became one of the most important medical texts in European universities during the Middle Ages and contained useful information on surgical techniques and spread of bacterial infection.[96]
The hospital was a typical institution included in the majority of Muslim cities, and although they were often physically attached to religious institutions, they were not themselves places of religious practice.[97] Rather, they served as facilities in which education and scientific innovation could flourish. If they had places of worship, they were secondary to the medical side of the hospital. Islamicate hospitals, along with observatories used for astronomical science, were some of the most important points of exchange for the spread of scientific knowledge. Undoubtedly, the hospital system developed in the Islamicate world played an invaluable role in the creation and evolution of the hospitals we as a society know and depend on today.
Europe
After 400 CE, the study and practice of medicine in the Western Roman Empire went into deep decline. Medical services were provided, especially for the poor, in the thousands of monastic hospitals that sprang up across Europe, but the care was rudimentary and mainly palliative.[99] Most of the writings of Galen and Hippocrates were lost to the West, with the summaries and compendia of St. Isidore of Seville being the primary channel for transmitting Greek medical ideas.[100] The Carolingian renaissance brought increased contact with Byzantium and a greater awareness of ancient medicine,[101] but only with the twelfth-century renaissance and the new translations coming from Muslim and Jewish sources in Spain, and the fifteenth-century flood of resources after the fall of Constantinople did the West fully recover its acquaintance with classical antiquity.
Greek and Roman taboos had meant that dissection was usually banned in ancient times, but in the Middle Ages it changed: medical teachers and students at Bologna began to open human bodies, and Mondino de Luzzi (c. 1275–1326) produced the first known anatomy textbook based on human dissection.[59][60]
Wallis identifies a prestige hierarchy with university educated physicians on top, followed by learned surgeons; craft-trained surgeons; barber surgeons; itinerant specialists such as dentist and oculists; empirics; and midwives.[102]
Institutions

The first medical schools were opened in the 9th century, most notably the Schola Medica Salernitana at Salerno in southern Italy. The cosmopolitan influences from Greek, Latin, Arabic, and Hebrew sources gave it an international reputation as the Hippocratic City. Students from wealthy families came for three years of preliminary studies and five of medical studies. The medicine, following the laws of Federico II, that he founded in 1224 the university and improved the Schola Salernitana, in the period between 1200 and 1400, it had in Sicily (so-called Sicilian Middle Ages) a particular development so much to create a true school of Jewish medicine.[103]
As a result of which, after a legal examination, was conferred to a Jewish Sicilian woman, Virdimura, wife of another physician Pasquale of Catania, the historical record of before woman officially trained to exercise of the medical profession.[104]
At the University of Bologna the training of physicians began in 1219. The Italian city attracted students from across Europe. Taddeo Alderotti built a tradition of medical education that established the characteristic features of Italian learned medicine and was copied by medical schools elsewhere.Turisanus (d. 1320) was his student.[105]
The University of Padua was founded about 1220 by walkouts from the University of Bologna, and began teaching medicine in 1222. It played a leading role in the identification and treatment of diseases and ailments, specializing in autopsies and the inner workings of the body.[106] Starting in 1595, Padua's famous anatomical theatre drew artists and scientists studying the human body during public dissections. The intensive study of Galen led to critiques of Galen modeled on his own writing, as in the first book of Vesalius's De humani corporis fabrica. Andreas Vesalius held the chair of Surgery and Anatomy (explicator chirurgiae) and in 1543 published his anatomical discoveries in De Humani Corporis Fabrica. He portrayed the human body as an interdependent system of organ groupings. The book triggered great public interest in dissections and caused many other European cities to establish anatomical theatres.[107]

By the thirteenth century, the medical school at Montpellier began to eclipse the Salernitan school. In the 12th century, universities were founded in Italy, France, and England, which soon developed schools of medicine. The University of Montpellier in France and Italy's University of Padua and University of Bologna were leading schools. Nearly all the learning was from lectures and readings in Hippocrates, Galen, Avicenna, and Aristotle. In later centuries, the importance of universities founded in the late Middle Ages gradually increased, e.g. Charles University in Prague (established in 1348), Jagiellonian University in Cracow (1364), University of Vienna (1365), Heidelberg University (1386) and University of Greifswald (1456).
Women
In 1376, in Sicily, it was historically given, in relationship to the laws of Federico II that they foresaw an examination with a regal errand of physicists, the first qualification to the exercise of the medicine to a woman, Virdimura a Jewish woman of Catania, whose document is preserved in Palermo to the Italian national archives.[108]
16th century medicine
Places
England
In England, there were but three small hospitals after 1550. Pelling and Webster estimate that in London in the 1580 to 1600 period, out of a population of nearly 200,000 people, there were about 500 medical practitioners. Nurses and midwives are not included. There were about 50 physicians, 100 licensed surgeons, 100 apothecaries, and 250 additional unlicensed practitioners. In the last category about 25% were women.[109] All across England—and indeed all of the world—the vast majority of the people in city, town or countryside depended for medical care on local amateurs with no professional training but with a reputation as wise healers who could diagnose problems and advise sick people what to do—and perhaps set broken bones, pull a tooth, give some traditional herbs or brews or perform a little magic to cure what ailed them.
People
 Paracelsus (1493-1541). Known as the "father" of toxicology.
Paracelsus (1493-1541). Known as the "father" of toxicology. Michael Servetus (1511-1553). Known as the first European to correctly describe pulmonary circulation.
Michael Servetus (1511-1553). Known as the first European to correctly describe pulmonary circulation..jpg.webp) Andreas Vesalius (1514-1564). Known as the modern founder of human anatomy.
Andreas Vesalius (1514-1564). Known as the modern founder of human anatomy.
17th century medicine
Europe
The Renaissance brought an intense focus on scholarship to Christian Europe. A major effort to translate the Arabic and Greek scientific works into Latin emerged. Europeans gradually became experts not only in the ancient writings of the Romans and Greeks, but in the contemporary writings of Islamic scientists. During the later centuries of the Renaissance came an increase in experimental investigation, particularly in the field of dissection and body examination, thus advancing our knowledge of human anatomy.[110]
_Venenbild.jpg.webp)

Ideas
- Animalcules: In 1677 Antonie van Leeuwenhoek identified "animalcules", which we now know as microorganisms, within their paper "letter on the protozoa".[111]
- Blood circulation: In 1628 the English physician William Harvey made a ground-breaking discovery when he correctly described the circulation of the blood in his Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus. Before this time the most useful manual in medicine used both by students and expert physicians was Dioscorides' De Materia Medica, a pharmacopoeia.
Inventions
- Microscopes: Bacteria and protists were first observed with a microscope by Antonie van Leeuwenhoek in 1676, initiating the scientific field of microbiology.[112]
Institutions
At the University of Bologna the curriculum was revised and strengthened in 1560–1590.[113] A representative professor was Julius Caesar Aranzi (Arantius) (1530–1589). He became Professor of Anatomy and Surgery at the University of Bologna in 1556, where he established anatomy as a major branch of medicine for the first time. Aranzi combined anatomy with a description of pathological processes, based largely on his own research, Galen, and the work of his contemporary Italians. Aranzi discovered the 'Nodules of Aranzio' in the semilunar valves of the heart and wrote the first description of the superior levator palpebral and the coracobrachialis muscles. His books (in Latin) covered surgical techniques for many conditions, including hydrocephalus, nasal polyp, goitre and tumours to phimosis, ascites, haemorrhoids, anal abscess and fistulae.[114]
People
Women
Catholic women played large roles in health and healing in medieval and early modern Europe.[115] A life as a nun was a prestigious role; wealthy families provided dowries for their daughters, and these funded the convents, while the nuns provided free nursing care for the poor.[116]
The Catholic elites provided hospital services because of their theology of salvation that good works were the route to heaven. The Protestant reformers rejected the notion that rich men could gain God's grace through good works—and thereby escape purgatory—by providing cash endowments to charitable institutions. They also rejected the Catholic idea that the poor patients earned grace and salvation through their suffering.[117] Protestants generally closed all the convents[118] and most of the hospitals, sending women home to become housewives, often against their will.[119] On the other hand, local officials recognized the public value of hospitals, and some were continued in Protestant lands, but without monks or nuns and in the control of local governments.[120]
In London, the crown allowed two hospitals to continue their charitable work, under nonreligious control of city officials.[121] The convents were all shut down but Harkness finds that women—some of them former nuns—were part of a new system that delivered essential medical services to people outside their family. They were employed by parishes and hospitals, as well as by private families, and provided nursing care as well as some medical, pharmaceutical, and surgical services.[122]
Meanwhile, in Catholic lands such as France, rich families continued to fund convents and monasteries, and enrolled their daughters as nuns who provided free health services to the poor. Nursing was a religious role for the nurse, and there was little call for science.[123]
18th century medicine
Events
European Age of Enlightenment
During the Age of Enlightenment, the 18th century, science was held in high esteem and physicians upgraded their social status by becoming more scientific. The health field was crowded with self-trained barber-surgeons, apothecaries, midwives, drug peddlers, and charlatans.
Across Europe medical schools relied primarily on lectures and readings. The final year student would have limited clinical experience by trailing the professor through the wards. Laboratory work was uncommon, and dissections were rarely done because of legal restrictions on cadavers. Most schools were small, and only Edinburgh, Scotland, with 11,000 alumni, produced large numbers of graduates.[124][125]
Places
Spain and the Spanish Empire
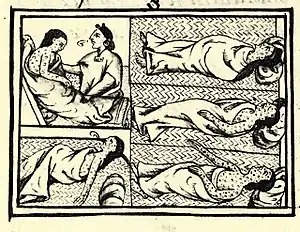
In the Spanish Empire, the viceregal capital of Mexico City was a site of medical training for physicians and the creation of hospitals. Epidemic disease had decimated indigenous populations starting with the early sixteenth-century Spanish conquest of the Aztec empire, when a black auxiliary in the armed forces of conqueror Hernán Cortés, with an active case of smallpox, set off a virgin land epidemic among indigenous peoples, Spanish allies and enemies alike. Aztec emperor Cuitlahuac died of smallpox.[126][127] Disease was a significant factor in the Spanish conquest elsewhere as well.[128]
Medical education instituted at the Royal and Pontifical University of Mexico chiefly served the needs of urban elites. Male and female curanderos or lay practitioners, attended to the ills of the popular classes. The Spanish crown began regulating the medical profession just a few years after the conquest, setting up the Royal Tribunal of the Protomedicato, a board for licensing medical personnel in 1527. Licensing became more systematic after 1646 with physicians, druggists, surgeons, and bleeders requiring a license before they could publicly practice.[129] Crown regulation of medical practice became more general in the Spanish empire.[130]
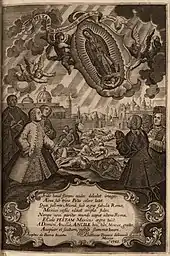
Elites and the popular classes alike called on divine intervention in personal and society-wide health crises, such as the epidemic of 1737. The intervention of the Virgin of Guadalupe was depicted in a scene of dead and dying Indians, with elites on their knees praying for her aid. In the late eighteenth century, the crown began implementing secularizing policies on the Iberian peninsula and its overseas empire to control disease more systematically and scientifically.[131][132][133]
Spanish Quest for Medicinal Spices
Botanical medicines also became popular during the 16th, 17th, and 18th Centuries. Spanish pharmaceutical books during this time contain medicinal recipes consisting of spices, herbs, and other botanical products. For example, nutmeg oil was documented for curing stomach ailments and cardamom oil was believed to relieve intestinal ailments.[134] During the rise of the global trade market, spices and herbs, along with many other goods, that were indigenous to different territories began to appear in different locations across the globe. Herbs and spices were especially popular for their utility in cooking and medicines. As a result of this popularity and increased demand for spices, some areas in Asia, like China and Indonesia, became hubs for spice cultivation and trade.[135] The Spanish Empire also wanted to benefit from the international spice trade, so they looked towards their American colonies.
The Spanish American colonies became an area where the Spanish searched to discover new spices and indigenous American medicinal recipes. The Florentine Codex, a 16th-century ethnographic research study in Mesoamerica by the Spanish Franciscan friar Bernardino de Sahagún, is a major contribution to the history of Nahua medicine.[136] The Spanish did discover many spices and herbs new to them, some of which were reportedly similar to Asian spices. A Spanish physician by the name of Nicolás Monardes studied many of the American spices coming into Spain. He documented many of the new American spices and their medicinal properties in his survey Historia medicinal de las cosas que se traen de nuestras Indias Occidentales. For example, Monardes describes the "Long Pepper" (Pimienta luenga), found along the coasts of the countries that are now known Panama and Colombia, as a pepper that was more flavorful, healthy, and spicy in comparison to the Eastern black pepper.[134] The Spanish interest in American spices can first be seen in the commissioning of the Libellus de Medicinalibus Indorum Herbis, which was a Spanish-American codex describing indigenous American spices and herbs and describing the ways that these were used in natural Aztec medicines. The codex was commissioned in the year 1552 by Francisco de Mendoza, the son of Antonio de Mendoza, who was the first Viceroy of New Spain.[134] Francisco de Mendoza was interested in studying the properties of these herbs and spices, so that he would be able to profit from the trade of these herbs and the medicines that could be produced by them.
Francisco de Mendoza recruited the help of Monardez in studying the traditional medicines of the indigenous people living in what was then the Spanish colonies. Monardez researched these medicines and performed experiments to discover the possibilities of spice cultivation and medicine creation in the Spanish colonies. The Spanish transplanted some herbs from Asia, but only a few foreign crops were successfully grown in the Spanish Colonies. One notable crop brought from Asia and successfully grown in the Spanish colonies was ginger, as it was considered Hispaniola's number 1 crop at the end of the 16th Century.[134] The Spanish Empire did profit from cultivating herbs and spices, but they also introduced pre-Columbian American medicinal knowledge to Europe. Other Europeans were inspired by the actions of Spain and decided to try to establish a botanical transplant system in colonies that they controlled, however, these subsequent attempts were not successful.[135]
United Kingdom and the British Empire

The London Dispensary opened in 1696, the first clinic in the British Empire to dispense medicines to poor sick people. The innovation was slow to catch on, but new dispensaries were open in the 1770s. In the colonies, small hospitals opened in Philadelphia in 1752, New York in 1771, and Boston (Massachusetts General Hospital) in 1811.[137]

Guy's Hospital, the first great British hospital with a modern foundation opened in 1721 in London, with funding from businessman Thomas Guy. It had been preceded by St Bartholomew's Hospital and St Thomas's Hospital, both medieval foundations. In 1821 a bequest of £200,000 by William Hunt in 1829 funded expansion for an additional hundred beds at Guy's. Samuel Sharp (1709–78), a surgeon at Guy's Hospital from 1733 to 1757, was internationally famous; his A Treatise on the Operations of Surgery (1st ed., 1739), was the first British study focused exclusively on operative technique.[138]
English physician Thomas Percival (1740–1804) wrote a comprehensive system of medical conduct, Medical Ethics; or, a Code of Institutes and Precepts, Adapted to the Professional Conduct of Physicians and Surgeons (1803) that set the standard for many textbooks.[139]
19th century medicine
Germ theory and bacteriology
In the 1830s in Italy, Agostino Bassi traced the silkworm disease muscardine to microorganisms. Meanwhile, in Germany, Theodor Schwann led research on alcoholic fermentation by yeast, proposing that living microorganisms were responsible. Leading chemists, such as Justus von Liebig, seeking solely physicochemical explanations, derided this claim and alleged that Schwann was regressing to vitalism.
In 1847 in Vienna, Ignaz Semmelweis (1818–1865), dramatically reduced the death rate of new mothers (due to childbed fever) by requiring physicians to clean their hands before attending childbirth, yet his principles were marginalized and attacked by professional peers.[140] At that time most people still believed that infections were caused by foul odors called miasmas.

French scientist Louis Pasteur confirmed Schwann's fermentation experiments in 1857 and afterwards supported the hypothesis that yeast were microorganisms. Moreover, he suggested that such a process might also explain contagious disease. In 1860, Pasteur's report on bacterial fermentation of butyric acid motivated fellow Frenchman Casimir Davaine to identify a similar species (which he called bacteridia) as the pathogen of the deadly disease anthrax. Others dismissed "bacteridia" as a mere byproduct of the disease. British surgeon Joseph Lister, however, took these findings seriously and subsequently introduced antisepsis to wound treatment in 1865.
German physician Robert Koch, noting fellow German Ferdinand Cohn's report of a spore stage of a certain bacterial species, traced the life cycle of Davaine's bacteridia, identified spores, inoculated laboratory animals with them, and reproduced anthrax—a breakthrough for experimental pathology and germ theory of disease. Pasteur's group added ecological investigations confirming spores' role in the natural setting, while Koch published a landmark treatise in 1878 on the bacterial pathology of wounds. In 1881, Koch reported discovery of the "tubercle bacillus", cementing germ theory and Koch's acclaim.
Upon the outbreak of a cholera epidemic in Alexandria, Egypt, two medical missions went to investigate and attend the sick, one was sent out by Pasteur and the other led by Koch.[141] Koch's group returned in 1883, having successfully discovered the cholera pathogen.[141] In Germany, however, Koch's bacteriologists had to vie against Max von Pettenkofer, Germany's leading proponent of miasmatic theory.[142] Pettenkofer conceded bacteria's casual involvement, but maintained that other, environmental factors were required to turn it pathogenic, and opposed water treatment as a misdirected effort amid more important ways to improve public health.[142] The massive cholera epidemic in Hamburg in 1892 devastated Pettenkoffer's position, and yielded German public health to "Koch's bacteriology".[142]
On losing the 1883 rivalry in Alexandria, Pasteur switched research direction, and introduced his third vaccine—rabies vaccine—the first vaccine for humans since Jenner's for smallpox.[141] From across the globe, donations poured in, funding the founding of Pasteur Institute, the globe's first biomedical institute, which opened in 1888.[141] Along with Koch's bacteriologists, Pasteur's group—which preferred the term microbiology—led medicine into the new era of "scientific medicine" upon bacteriology and germ theory.[141] Accepted from Jakob Henle, Koch's steps to confirm a species' pathogenicity became famed as "Koch's postulates". Although his proposed tuberculosis treatment, tuberculin, seemingly failed, it soon was used to test for infection with the involved species. In 1905, Koch was awarded the Nobel Prize in Physiology or Medicine, and remains renowned as the founder of medical microbiology.[143]
Nursing
The breakthrough to professionalization based on knowledge of advanced medicine was led by Florence Nightingale in England. She resolved to provide more advanced training than she saw on the Continent. At Kaiserswerth, where the first German nursing schools were founded in 1836 by Theodor Fliedner, she said, "The nursing was nil and the hygiene horrible."[144]) Britain's male doctors preferred the old system, but Nightingale won out and her Nightingale Training School opened in 1860 and became a model. The Nightingale solution depended on the patronage of upper-class women, and they proved eager to serve. Royalty became involved. In 1902 the wife of the British king took control of the nursing unit of the British army, became its president, and renamed it after herself as the Queen Alexandra's Royal Army Nursing Corps; when she died the next queen became president. Today its Colonel In Chief is Sophie, Countess of Wessex, the daughter-in-law of Queen Elizabeth II. In the United States, upper-middle-class women who already supported hospitals promoted nursing. The new profession proved highly attractive to women of all backgrounds, and schools of nursing opened in the late 19th century. They were soon a function of large hospitals , where they provided a steady stream of low-paid idealistic workers. The International Red Cross began operations in numerous countries in the late 19th century, promoting nursing as an ideal profession for middle-class women.[145]
Statistical methods
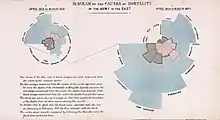
A major breakthrough in epidemiology came with the introduction of statistical maps and graphs. They allowed careful analysis of seasonality issues in disease incidents, and the maps allowed public health officials to identify critical loci for the dissemination of disease. John Snow in London developed the methods. In 1849, he observed that the symptoms of cholera, which had already claimed around 500 lives within a month, were vomiting and diarrhoea. He concluded that the source of contamination must be through ingestion, rather than inhalation as was previously thought. It was this insight that resulted in the removal of The Pump On Broad Street, after which deaths from cholera plummeted. English nurse Florence Nightingale pioneered analysis of large amounts of statistical data, using graphs and tables, regarding the condition of thousands of patients in the Crimean War to evaluate the efficacy of hospital services. Her methods proved convincing and led to reforms in military and civilian hospitals, usually with the full support of the government.[146][147]>[148]
By the late 19th and early 20th century English statisticians led by Francis Galton, Karl Pearson and Ronald Fisher developed the mathematical tools such as correlations and hypothesis tests that made possible much more sophisticated analysis of statistical data.[149]
During the U.S. Civil War the Sanitary Commission collected enormous amounts of statistical data, and opened up the problems of storing information for fast access and mechanically searching for data patterns. The pioneer was John Shaw Billings (1838–1913). A senior surgeon in the war, Billings built the Library of the Surgeon General's Office (now the National Library of Medicine), the centerpiece of modern medical information systems.[150] Billings figured out how to mechanically analyze medical and demographic data by turning facts into numbers and punching the numbers onto cardboard cards that could be sorted and counted by machine. The applications were developed by his assistant Herman Hollerith; Hollerith invented the punch card and counter-sorter system that dominated statistical data manipulation until the 1970s. Hollerith's company became International Business Machines (IBM) in 1911.[151]
Psychiatry

Until the nineteenth century, the care of the insane was largely a communal and family responsibility rather than a medical one. The vast majority of the mentally ill were treated in domestic contexts with only the most unmanageable or burdensome likely to be institutionally confined.[152] This situation was transformed radically from the late eighteenth century as, amid changing cultural conceptions of madness, a new-found optimism in the curability of insanity within the asylum setting emerged.[153] Increasingly, lunacy was perceived less as a physiological condition than as a mental and moral one[154] to which the correct response was persuasion, aimed at inculcating internal restraint, rather than external coercion.[155] This new therapeutic sensibility, referred to as moral treatment, was epitomised in French physician Philippe Pinel's quasi-mythological unchaining of the lunatics of the Bicêtre Hospital in Paris[156] and realised in an institutional setting with the foundation in 1796 of the Quaker-run York Retreat in England.[22]
From the early nineteenth century, as lay-led lunacy reform movements gained in influence,[157] ever more state governments in the West extended their authority and responsibility over the mentally ill.[158] Small-scale asylums, conceived as instruments to reshape both the mind and behaviour of the disturbed,[159] proliferated across these regions.[160] By the 1830s, moral treatment, together with the asylum itself, became increasingly medicalised[161] and asylum doctors began to establish a distinct medical identity with the establishment in the 1840s of associations for their members in France, Germany, the United Kingdom and America, together with the founding of medico-psychological journals.[22] Medical optimism in the capacity of the asylum to cure insanity soured by the close of the nineteenth century as the growth of the asylum population far outstripped that of the general population.[lower-alpha 1][162] Processes of long-term institutional segregation, allowing for the psychiatric conceptualisation of the natural course of mental illness, supported the perspective that the insane were a distinct population, subject to mental pathologies stemming from specific medical causes.[159] As degeneration theory grew in influence from the mid-nineteenth century,[163] heredity was seen as the central causal element in chronic mental illness,[164] and, with national asylum systems overcrowded and insanity apparently undergoing an inexorable rise, the focus of psychiatric therapeutics shifted from a concern with treating the individual to maintaining the racial and biological health of national populations.[165]
Emil Kraepelin (1856–1926) introduced new medical categories of mental illness, which eventually came into psychiatric usage despite their basis in behavior rather than pathology or underlying cause. Shell shock among frontline soldiers exposed to heavy artillery bombardment was first diagnosed by British Army doctors in 1915. By 1916, similar symptoms were also noted in soldiers not exposed to explosive shocks, leading to questions as to whether the disorder was physical or psychiatric.[166] In the 1920s surrealist opposition to psychiatry was expressed in a number of surrealist publications. In the 1930s several controversial medical practices were introduced including inducing seizures (by electroshock, insulin or other drugs) or cutting parts of the brain apart (leucotomy or lobotomy). Both came into widespread use by psychiatry, but there were grave concerns and much opposition on grounds of basic morality, harmful effects, or misuse.[167]
In the 1950s new psychiatric drugs, notably the antipsychotic chlorpromazine, were designed in laboratories and slowly came into preferred use. Although often accepted as an advance in some ways, there was some opposition, due to serious adverse effects such as tardive dyskinesia. Patients often opposed psychiatry and refused or stopped taking the drugs when not subject to psychiatric control. There was also increasing opposition to the use of psychiatric hospitals, and attempts to move people back into the community on a collaborative user-led group approach ("therapeutic communities") not controlled by psychiatry. Campaigns against masturbation were done in the Victorian era and elsewhere. Lobotomy was used until the 1970s to treat schizophrenia. This was denounced by the anti-psychiatric movement in the 1960s and later.
Women
It was very difficult for women to become doctors in any field before the 1970s. Elizabeth Blackwell became the first woman to formally study and practice medicine in the United States. She was a leader in women's medical education. While Blackwell viewed medicine as a means for social and moral reform, her student Mary Putnam Jacobi (1842–1906) focused on curing disease. At a deeper level of disagreement, Blackwell felt that women would succeed in medicine because of their humane female values, but Jacobi believed that women should participate as the equals of men in all medical specialties using identical methods, values and insights.[168] In the Soviet Union although the majority of medical doctors were women, they were paid less than the mostly male factory workers.[169]
Places
Japan
.jpg.webp)
European ideas of modern medicine were spread widely through the world by medical missionaries, and the dissemination of textbooks. Japanese elites enthusiastically embraced Western medicine after the Meiji Restoration of the 1860s. However they had been prepared by their knowledge of the Dutch and German medicine, for they had some contact with Europe through the Dutch. Highly influential was the 1765 edition of Hendrik van Deventer's pioneer work Nieuw Ligt ("A New Light") on Japanese obstetrics, especially on Katakura Kakuryo's publication in 1799 of Sanka Hatsumo ("Enlightenment of Obstetrics").[170][171] A cadre of Japanese physicians began to interact with Dutch doctors, who introduced smallpox vaccinations. By 1820 Japanese ranpô medical practitioners not only translated Dutch medical texts, they integrated their readings with clinical diagnoses. These men became leaders of the modernization of medicine in their country. They broke from Japanese traditions of closed medical fraternities and adopted the European approach of an open community of collaboration based on expertise in the latest scientific methods.[172]
Kitasato Shibasaburō (1853–1931) studied bacteriology in Germany under Robert Koch. In 1891 he founded the Institute of Infectious Diseases in Tokyo, which introduced the study of bacteriology to Japan. He and French researcher Alexandre Yersin went to Hong Kong in 1894, where; Kitasato confirmed Yersin's discovery that the bacterium Yersinia pestis is the agent of the plague. In 1897 he isolated and described the organism that caused dysentery. He became the first dean of medicine at Keio University, and the first president of the Japan Medical Association.[173][174]
Japanese physicians immediately recognized the values of X-Rays. They were able to purchase the equipment locally from the Shimadzu Company, which developed, manufactured, marketed, and distributed X-Ray machines after 1900.[175] Japan not only adopted German methods of public health in the home islands, but implemented them in its colonies, especially Korea and Taiwan, and after 1931 in Manchuria.[176] A heavy investment in sanitation resulted in a dramatic increase of life expectancy.[177]
Europe
The practice of medicine changed in the face of rapid advances in science, as well as new approaches by physicians. Hospital doctors began much more systematic analysis of patients' symptoms in diagnosis.[178] Among the more powerful new techniques were anaesthesia, and the development of both antiseptic and aseptic operating theatres.[179] Effective cures were developed for certain endemic infectious diseases. However, the decline in many of the most lethal diseases was due more to improvements in public health and nutrition than to advances in medicine.[180]
Medicine was revolutionized in the 19th century and beyond by advances in chemistry, laboratory techniques, and equipment. Old ideas of infectious disease epidemiology were gradually replaced by advances in bacteriology and virology.[112]
The Russian Orthodox Church sponsored seven orders of nursing sisters in the late 19th century.
They ran hospitals, clinics, almshouses, pharmacies, and shelters as well as training schools for nurses. In the Soviet era (1917–1991), with the aristocratic sponsors gone, nursing became a low-prestige occupation based in poorly maintained hospitals.[181]
Places
France
Paris (France) and Vienna were the two leading medical centers on the Continent in the era 1750–1914.
In the 1770s–1850s Paris became a world center of medical research and teaching. The "Paris School" emphasized that teaching and research should be based in large hospitals and promoted the professionalization of the medical profession and the emphasis on sanitation and public health. A major reformer was Jean-Antoine Chaptal (1756–1832), a physician who was Minister of Internal Affairs. He created the Paris Hospital, health councils, and other bodies.[182]
Louis Pasteur (1822–1895) was one of the most important founders of medical microbiology. He is remembered for his remarkable breakthroughs in the causes and preventions of diseases. His discoveries reduced mortality from puerperal fever, and he created the first vaccines for rabies and anthrax. His experiments supported the germ theory of disease. He was best known to the general public for inventing a method to treat milk and wine in order to prevent it from causing sickness, a process that came to be called pasteurization. He is regarded as one of the three main founders of microbiology, together with Ferdinand Cohn and Robert Koch. He worked chiefly in Paris and in 1887 founded the Pasteur Institute there to perpetuate his commitment to basic research and its practical applications. As soon as his institute was created, Pasteur brought together scientists with various specialties. The first five departments were directed by Emile Duclaux (general microbiology research) and Charles Chamberland (microbe research applied to hygiene), as well as a biologist, Ilya Ilyich Mechnikov (morphological microbe research) and two physicians, Jacques-Joseph Grancher (rabies) and Emile Roux (technical microbe research). One year after the inauguration of the Institut Pasteur, Roux set up the first course of microbiology ever taught in the world, then entitled Cours de Microbie Technique (Course of microbe research techniques). It became the model for numerous research centers around the world named "Pasteur Institutes.[183][184]
Vienna
The First Viennese School of Medicine, 1750–1800, was led by the Dutchman Gerard van Swieten (1700–1772), who aimed to put medicine on new scientific foundations—promoting unprejudiced clinical observation, botanical and chemical research, and introducing simple but powerful remedies. When the Vienna General Hospital opened in 1784, it at once became the world's largest hospital and physicians acquired a facility that gradually developed into the most important research centre.[185] Progress ended with the Napoleonic wars and the government shutdown in 1819 of all liberal journals and schools; this caused a general return to traditionalism and eclecticism in medicine.[186]
Vienna was the capital of a diverse empire and attracted not just Germans but Czechs, Hungarians, Jews, Poles and others to its world-class medical facilities. After 1820 the Second Viennese School of Medicine emerged with the contributions of physicians such as Carl Freiherr von Rokitansky, Josef Škoda, Ferdinand Ritter von Hebra, and Ignaz Philipp Semmelweis. Basic medical science expanded and specialization advanced. Furthermore, the first dermatology, eye, as well as ear, nose, and throat clinics in the world were founded in Vienna. The textbook of ophthalmologist Georg Joseph Beer (1763–1821) Lehre von den Augenkrankheiten combined practical research and philosophical speculations, and became the standard reference work for decades.[187]
Berlin
After 1871 Berlin, the capital of the new German Empire, became a leading center for medical research. Robert Koch (1843–1910) was a representative leader. He became famous for isolating Bacillus anthracis (1877), the Tuberculosis bacillus (1882) and Vibrio cholerae (1883) and for his development of Koch's postulates. He was awarded the Nobel Prize in Physiology or Medicine in 1905 for his tuberculosis findings. Koch is one of the founders of microbiology, inspiring such major figures as Paul Ehrlich and Gerhard Domagk.[184]
Events
American Civil War
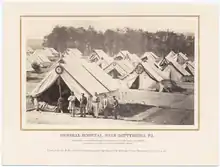
In the American Civil War (1861–65), as was typical of the 19th century, more soldiers died of disease than in battle, and even larger numbers were temporarily incapacitated by wounds, disease and accidents.[188][189] Conditions were poor in the Confederacy, where doctors and medical supplies were in short supply.[190] The war had a dramatic long-term impact on medicine in the U.S., from surgical technique to hospitals to nursing and to research facilities. Weapon development -particularly the appearance of Springfield Model 1861, mass-produced and much more accurate than muskets led to generals underestimating the risks of long range rifle fire; risks exemplified in the death of John Sedgwick and the disastrous Pickett's Charge. The rifles could shatter bone forcing amputation and longer ranges meant casualties were sometimes not quickly found. Evacuation of the wounded from Second Battle of Bull Run took a week.[191] As in earlier wars, untreated casualties sometimes survived unexpectedly due to maggots debriding the wound -an observation which led to the surgical use of maggots -still a useful method in the absence of effective antibiotics.
The hygiene of the training and field camps was poor, especially at the beginning of the war when men who had seldom been far from home were brought together for training with thousands of strangers. First came epidemics of the childhood diseases of chicken pox, mumps, whooping cough, and, especially, measles. Operations in the South meant a dangerous and new disease environment, bringing diarrhea, dysentery, typhoid fever, and malaria. There were no antibiotics, so the surgeons prescribed coffee, whiskey, and quinine. Harsh weather, bad water, inadequate shelter in winter quarters, poor policing of camps, and dirty camp hospitals took their toll.[192]
This was a common scenario in wars from time immemorial, and conditions faced by the Confederate army were even worse. The Union responded by building army hospitals in every state. What was different in the Union was the emergence of skilled, well-funded medical organizers who took proactive action, especially in the much enlarged United States Army Medical Department,[193] and the United States Sanitary Commission, a new private agency.[194] Numerous other new agencies also targeted the medical and morale needs of soldiers, including the United States Christian Commission as well as smaller private agencies.[195]
The U.S. Army learned many lessons and in August 1886, it established the Hospital Corps.
Institutions
Johns Hopkins Hospital, founded in 1889, originated several modern medical practices, including residency and rounds.
People
 Louis Pasteur (1822-1895) known for their modern founding of bacteriology, contributions to germ theory, and pasteurization.
Louis Pasteur (1822-1895) known for their modern founding of bacteriology, contributions to germ theory, and pasteurization. Rebecca Lee Crumpler (1831-1895) known as the first African-American woman to become a physician.
Rebecca Lee Crumpler (1831-1895) known as the first African-American woman to become a physician.
20th century medicine
Blood groups
The ABO blood group system was discovered in 1901 by Karl Landsteiner at the University of Vienna. Landsteiner experimented on his staff, mixing their various blood components together, and found that some people's blood agglutinated (clumped together) with other blood, whilst some did not. This then lead him identifying three blood groups, ABC, which would later be renamed to ABO.[196] The less frequently found blood group AB was discovered later in 1902 by Alfred Von Decastello and Adriano Sturli.[197] In 1937 Landsteiner and Alexander S. Wiener further discovered the Rh factor (misnamed from early thinking that this blood group was similar to that found in rhesus monkies) whose antigens further determine blood reaction between people.[197] This was demonstrated in a 1939 case study by Phillip Levine and Rufus Stetson where a mother who had recently given birth had reacted to their partner's blood, highlighting the Rh factor.[198]
Blood transfusion
Canadian physician Norman Bethune, M.D. developed a mobile blood-transfusion service for frontline operations in the Spanish Civil War (1936–1939), but ironically, he himself died of sepsis.[199]
Pacemaker
In 1958, Arne Larsson in Sweden became the first patient to depend on an artificial cardiac pacemaker. He died in 2001 at age 86, having outlived its inventor, the surgeon, and 26 pacemakers.
Cancer
Cancer treatment has been developed with radiotherapy, chemotherapy and surgical oncology.
Diagnosis
X-ray imaging was the first kind of medical imaging, and later ultrasonic imaging, CT scanning, MR scanning and other imaging methods became available.
Disabilities

Prosthetics have improved with lightweight materials as well as neural prosthetics emerging in the end of the 20th century.
Diseases
Oral rehydration therapy has been extensively used since the 1970s to treat cholera and other diarrhea-inducing infections.
As infectious diseases have become less lethal, and the most common causes of death in developed countries are now tumors and cardiovascular diseases, these conditions have received increased attention in medical research.
Malaria eradication
Starting in World War II, DDT was used as insecticide to combat insect vectors carrying malaria, which was endemic in most tropical regions of the world.[200][201][202] The first goal was to protect soldiers, but it was widely adopted as a public health device. In Liberia, for example, the United States had large military operations during the war and the U.S. Public Health Service began the use of DDT for indoor residual spraying (IRS) and as a larvicide, with the goal of controlling malaria in Monrovia, the Liberian capital. In the early 1950s, the project was expanded to nearby villages. In 1953, the World Health Organization (WHO) launched an antimalaria program in parts of Liberia as a pilot project to determine the feasibility of malaria eradication in tropical Africa. However these projects encountered a spate of difficulties that foreshadowed the general retreat from malaria eradication efforts across tropical Africa by the mid-1960s.[203]
1918 influenza pandemic (1918-1920)
The 1918 influenza pandemic was a global pandemic in the early 20th century that occurred between 1918 to 1920. Sometimes known as Spanish Flu due to popular opinion at the time thinking the flu originated from Spain, this pandemic caused close to 50 million deaths around the world.[204] Spreading at the end of World War I.[205]
Public health
Public health measures became particularly important during the 1918 flu pandemic, which killed at least 50 million people around the world.[206] It became an important case study in epidemiology.[207] Bristow shows there was a gendered response of health caregivers to the pandemic in the United States. Male doctors were unable to cure the patients, and they felt like failures. Women nurses also saw their patients die, but they took pride in their success in fulfilling their professional role of caring for, ministering, comforting, and easing the last hours of their patients, and helping the families of the patients cope as well.
Research
Evidence-based medicine is a modern concept, not introduced to literature until the 1990s.
Sexual and reproductive health
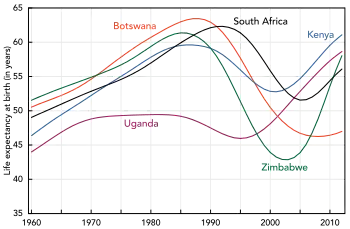
The sexual revolution included taboo-breaking research in human sexuality such as the 1948 and 1953 Kinsey reports, invention of hormonal contraception, and the normalization of abortion and homosexuality in many countries. Family planning has promoted a demographic transition in most of the world. With threatening sexually transmitted infections, not least HIV, use of barrier contraception has become imperative. The struggle against HIV has improved antiretroviral treatments.
Smoking
Tobacco smoking as a cause of lung cancer was first researched in the 1920s, but was not widely supported by publications until the 1950s.
Surgery
Cardiac surgery was revolutionized in 1948 as open-heart surgery was introduced for the first time since 1925. In 1954 Joseph Murray, J. Hartwell Harrison and others accomplished the first kidney transplantation. Transplantations of other organs, such as heart, liver and pancreas, were also introduced during the later 20th century. The first partial face transplant was performed in 2005, and the first full one in 2010. By the end of the 20th century, microtechnology had been used to create tiny robotic devices to assist microsurgery using micro-video and fiber-optic cameras to view internal tissues during surgery with minimally invasive practices.[208] Laparoscopic surgery was broadly introduced in the 1990s. Natural orifice surgery has followed.
Mexican Revolution (1910-1920)
During the 19th century, large-scale wars were attended with medics and mobile hospital units which developed advanced techniques for healing massive injuries and controlling infections rampant in battlefield conditions. During the Mexican Revolution (1910–1920), General Pancho Villa organized hospital trains for wounded soldiers. Boxcars marked Servicio Sanitario ("sanitary service") were re-purposed as surgical operating theaters and areas for recuperation, and staffed by up to 40 Mexican and U.S. physicians. Severely wounded soldiers were shuttled back to base hospitals.[209]
World War I (1914-1918)
Thousands of scarred troops provided the need for improved prosthetic limbs and expanded techniques in plastic surgery or reconstructive surgery. Those practices were combined to broaden cosmetic surgery and other forms of elective surgery.
Interwar period (1918-1939)
From 1917 to 1932, the American Red Cross moved into Europe with a battery of long-term child health projects. It built and operated hospitals and clinics, and organized antituberculosis and antityphus campaigns. A high priority involved child health programs such as clinics, better baby shows, playgrounds, fresh air camps, and courses for women on infant hygiene. Hundreds of U.S. doctors, nurses, and welfare professionals administered these programs, which aimed to reform the health of European youth and to reshape European public health and welfare along American lines.[210][211]
World War II (1939-1945)

The advances in medicine made a dramatic difference for Allied troops, while the Germans and especially the Japanese and Chinese suffered from a severe lack of newer medicines, techniques and facilities. Harrison finds that the chances of recovery for a badly wounded British infantryman were as much as 25 times better than in the First World War. The reason was that:
- "By 1944 most casualties were receiving treatment within hours of wounding, due to the increased mobility of field hospitals and the extensive use of aeroplanes as ambulances. The care of the sick and wounded had also been revolutionized by new medical technologies, such as active immunization against tetanus, sulphonamide drugs, and penicillin."[212]
During the second World War, Alexis Carrel and Henry Dakin developed the Carrel-Dakin method of treating wounds with an irrigation, Dakin's solution, a germicide which helped prevent gangrene.[213]
The War spurred the usage of Roentgen's X-ray, and the electrocardiograph, for the monitoring of internal bodily functions. This was followed in the inter-war period by the development of the first anti-bacterial agents such as the sulpha antibiotics.
Nazi and Japanese medical research
Unethical human subject research, and killing of patients with disabilities, peaked during the Nazi era, with Nazi human experimentation and Aktion T4 during the Holocaust as the most significant examples. Many of the details of these and related events were the focus of the Doctors' Trial. Subsequently, principles of medical ethics, such as the Nuremberg Code, were introduced to prevent a recurrence of such atrocities.[214] After 1937, the Japanese Army established programs of biological warfare in China. In Unit 731, Japanese doctors and research scientists conducted large numbers of vivisections and experiments on human beings, mostly Chinese victims.[215]
World Health Organization

The World Health Organization was founded in 1948 as a United Nations agency to improve global health. In most of the world, life expectancy has improved since then, and was about 67 years as of 2010, and well above 80 years in some countries. Eradication of infectious diseases is an international effort, and several new vaccines have been developed during the post-war years, against infections such as measles, mumps, several strains of influenza and human papilloma virus. The long-known vaccine against Smallpox finally eradicated the disease in the 1970s, and Rinderpest was wiped out in 2011. Eradication of polio is underway. Tissue culture is important for development of vaccines. Though the early success of antiviral vaccines and antibacterial drugs, antiviral drugs were not introduced until the 1970s. Through the WHO, the international community has developed a response protocol against epidemics, displayed during the SARS epidemic in 2003, the Influenza A virus subtype H5N1 from 2004, the Ebola virus epidemic in West Africa and onwards.
People
 Mary Putnam Jacobi (1842-1906) known for debunking myths around menstration and female intelligence.
Mary Putnam Jacobi (1842-1906) known for debunking myths around menstration and female intelligence. Florence Nightingale (1820-1910) known for their social action and reforms to nursing.
Florence Nightingale (1820-1910) known for their social action and reforms to nursing. Elizabeth Blackwell (1821-1910) known as the first women to gain a medical degree in the United States.
Elizabeth Blackwell (1821-1910) known as the first women to gain a medical degree in the United States. Susan La Flesche Picotte (1865-1915) known for their activism and as the first indigenous woman to gain a medical degree in the United States.
Susan La Flesche Picotte (1865-1915) known for their activism and as the first indigenous woman to gain a medical degree in the United States..jpg.webp) Linda Richards (1841-1930) known for their pioneering work in nursing.
Linda Richards (1841-1930) known for their pioneering work in nursing. Karl Landsteiner (1868-1943) known for discovering the ABO blood group system.
Karl Landsteiner (1868-1943) known for discovering the ABO blood group system. Alexander Fleming (1881-1955) known for the discovery of penicillin and lysozyme.
Alexander Fleming (1881-1955) known for the discovery of penicillin and lysozyme. Gerty Cori (1896-1957) known for their discovery of the catalytic conversion of glycogen and first woman awarded a Nobel Prize in Physiology or Medicine.
Gerty Cori (1896-1957) known for their discovery of the catalytic conversion of glycogen and first woman awarded a Nobel Prize in Physiology or Medicine. Virginia Apgar (1909-1974) known for the Apgar score and improving infant mortality.
Virginia Apgar (1909-1974) known for the Apgar score and improving infant mortality.
21st century medicine
Antibiotics and antibiotic resistance
The discovery of penicillin in the 20th century by Alexander Fleming provided a vital line of defence against baterical infections that, without them, often cause patients to suffer prelonged recovery periods and highly increased chances of death. Its discovery and application within medicine allowed previously impossible treatments to take place, including cancer treatments, organ transplants, to open heart surgery.[216] Throughout the 20th century, though, their overprescribed use to humans,[217] as well as to animals that need them due to the conditions of intensive animal farming,[218] has led to the development of antibiotic resistant bacteria.[216]
Robotics

Pandemics


The early 21st century, facilitated by extensive global connections, international travel, and unprecedented human disruption of ecological systems,[219][220] has been defined by a number of noval as well as continuing global pandemics from the 20th century.[221]
Past
The SARS 2002 to 2004 outbreak affected a number of countries around the world and killed hundreds. This outbreak gave rise to a number of lessons learnt from viral infection control, including more effective isolation room protocols to better hand washing techniques for medical staff.[222] A mutated strain of SARS would go on to develop into COVID-19, causing the future COVID-19 pandemic. A significant influenza strain, H1N1, caused a further pandemic between 2009 to 2010. Known as swine flu, due to its indirect source from pigs, it went on to infect over 700 million people.[223]
Ongoing
The continuing HIV pandemic, starting in 1981, has infected and led to the deaths of millions of people around the world.[224] Emerging and improved pre-exposure prophylaxis (PrEP) and post-exposure prophylaxis (PEP) treatments that aim to reduce the spread of the disease have proven effective in limiting the spread of HIV[225] alongside combined use of safe sex methods, sexual health education, needle exchange programmes, and sexual health screenings.[226] Efforts to find a HIV vaccine are ongoing whilst health inequities have left certain population groups, like trans women,[227] as well as resource limited regions, like sub-Saharan Africa, at greater risk of contracting HIV compared with, for example, developed countries.[228]
The outbreak of COVID-19, starting in 2019, and subsequent declaration of the COVID-19 pandemic by the WHO[229] is a major pandemic event within the early 21st century. Causing global disruptions, millions of infections and deaths, the pandemic has caused suffering throughout communities. The pandemic has also seen some of the largest logistical organisations of goods, medical equipment, medical professionals, and military personnel since World War II that highlights its far-reaching impact.[230][231]
Personalised medicine
The rise of personalised medicine in the 21st century has generated the possibility to develop diagnosis and treatments based on the individual characteristics of a person, rather than through generic practices that defined 20th century medicine. Areas like DNA sequencing, genetic mapping, gene therapy, imaging protocols, proteomics, stem cell therapy, and wireless health monitoring devices[232] are all rising innovations that can help medical professionals fine tune treatment to the individual.[233][234]
Telemedicine
Remote surgery is another recent development, with the transatlantic Lindbergh operation in 2001 as a groundbreaking example.
People
 Patricia Goldman-Rakic (1937-2003) known for research around the prefrontal cortex and working memory.
Patricia Goldman-Rakic (1937-2003) known for research around the prefrontal cortex and working memory. Luc Montagnier (1932-2022) known as one of the co-discoverers of HIV.
Luc Montagnier (1932-2022) known as one of the co-discoverers of HIV. 屠呦呦 [Tu Youyou] (1930-present) known for discovering malaria treatments.
屠呦呦 [Tu Youyou] (1930-present) known for discovering malaria treatments. Joycelyn Elders (1933-present) known as the first Black American women to serve as the Surgeon General of the United States.
Joycelyn Elders (1933-present) known as the first Black American women to serve as the Surgeon General of the United States. Antonia Novello (1944-present) known as the first woman and first Hispanic to serve as the Surgeon General of the United States.
Antonia Novello (1944-present) known as the first woman and first Hispanic to serve as the Surgeon General of the United States. Françoise Barré-Sinoussi (1947-present) known as one of the co-discoverers of HIV.
Françoise Barré-Sinoussi (1947-present) known as one of the co-discoverers of HIV._(cropped).jpg.webp) Tedros Adhanom Ghebreyesus (1965-present) first African Director-General of the World Health Organization.
Tedros Adhanom Ghebreyesus (1965-present) first African Director-General of the World Health Organization.
Themes in medical history
Racism in medicine
Racism has a long history in how medicine has evolved and established itself, both in terms of racism experience upon patients, professionals, and wider systematic violence within medical institutions and systems.[235][236] See: medical racism in the United States, race and health, and scientific racism.
Women in medicine
Women have always served as healers and midwives since ancient times. However, the professionalization of medicine forced them increasingly to the sidelines. As hospitals multiplied they relied in Europe on orders of Roman Catholic nun-nurses, and German Protestant and Anglican deaconesses in the early 19th century. They were trained in traditional methods of physical care that involved little knowledge of medicine.
See also
- Health care in the United States
- History of dental treatments
- History of herbalism
- History of hospitals
- History of medicine in Canada
- History of medicine in the United States
- History of nursing
- History of pathology
- History of pharmacy
- History of surgery
- Timeline of nursing history
- Timeline of medicine and medical technology
- History of health care (disambiguation)
Explanatory notes
- England and Wales had nine county and borough asylums in 1827 with an average capacity of a little over 100 patients, but by 1890 there were 66 such asylums containing on average 800 patients each;[lower-alpha 2] the total number of patients so confined increased from 1,027 in 1827 to 74,004 in 1900.[lower-alpha 3] Similarly, in Germany, between 1852 and 1898 the asylum population increased seven-fold from 11,622 to 74,087 patients during a period when the total population had only grown by ten per cent.[lower-alpha 4] In America the asylum population had risen to almost 250,000 on the eve of the First World War.[lower-alpha 5]
- Scull A (2005). Most Solitary of Afflictions: Madness And Society in Britain, 1700–1900. Yale University Press. p. 281. ISBN 978-0300107548.
- Jones K (1993). Asylums and after: a revised history of the mental health services: from the early 18th century to the 1990s. Athlone Press. p. 116. ISBN 978-0485120912.
- Wright D (April 1997). "Getting out of the asylum: understanding the confinement of the insane in the nineteenth century". Social History of Medicine. 10 (1): 137–155. doi:10.1093/shm/10.1.137. PMID 11619188.
References
- Paterson GR, Neilson JB, Roland CG (November 1982). "History of medicine". Canadian Medical Association Journal. 127 (10): 948. PMC 1862317. PMID 7139436.
- Kushner HI (August 2008). "Medical historians and the history of medicine". Lancet. 372 (9640): 710–711. doi:10.1016/S0140-6736(08)61293-3. PMID 18767211. S2CID 32704754.
- Spikins P, Needham A, Tilley L, Hitchens G (22 February 2018). "Calculated or caring? Neanderthal healthcare in social context". World Anthropology. 50 (3): 384–403. doi:10.1080/00438243.2018.1433060.
- Datta S, Bhattacherjee S, Bhattacherjee D. "Contribution of India in Medical Sciences" (PDF). In Muruganathan A, Bansode BR (eds.). Progress in MedicineEdition. The Association of Physicians of India. Archived from the original (PDF) on 2018-04-08. Retrieved 2018-04-07.
- "Stone age man used dentist drill". BBC News. 6 April 2006.
- Walker AA (September–October 1997). "Neolithic Surgery". Archaeology Magazine Archive. 50 (5).
- Buquet-Marcon C, Charlier P, Samzun A (December 2009). "A possible Early Neolithic amputation at Buthiers-Boulancourt (Seine-et-Marne), France". Antiquity. 3 (322).
- Unschuld PU (2003). Huang Di Nei Jing Su Wen: nature, knowledge, imagery in an ancient Chinese medical text, with an appendix, the doctrine of the five periods and six qi in the Huang Di Nei Jing Su Wen. Berkeley: University of California Press. ISBN 978-0-520-92849-7.
- Dikotter F (2003). "China". In Porter R (ed.). The Cambridge History of Science. Vol. 4: 18th-century Science. pp. 695–697. ISBN 978-0-521-57243-9.
- Barnes LL (2012). "Eighteenth-Century European Views of Gongfu (Kungfu)". In Hinrichs TJ, Barnes LL (eds.). Chinese Medicine and Healing: An Illustrated History. Harvard University Press. p. 197. ISBN 978-0674047372.
- James ET, James GW, Boyer PS, eds. (1971). "Fulton". Notable American Women, 1607–1950: A Biographical Dictionary. Vol. 2. Harvard University Press. pp. 685–86. ISBN 978-0674627345.
- Furth C (1999). A Flourishing Yin: Gender in China's Medical History, 960–1665. Berkeley: University of California Press.
- Zysk KG (1991). Asceticism and Healing in Ancient India: Medicine in the Buddhist Monastery. New York: Oxford University Press. ISBN 978-0-19-505956-4.
- Wujastyk D, ed. (2003). The Roots of Ayurveda: selections from Sankskrit medical writings (Rev. ed.). London: Penguin Books. ISBN 978-0-14-044824-5.
- Rahman HS (1996). "Arab Medicine During the Ages". Studies in History of Medicine and Science. New Delhi: IHMMR. m 14 (1–2): 1–39.
- Kumar D (2003). "India". In Porter R, Ross D (eds.). The Cambridge History of Science. Vol. 4: 18th-century Science. Cambridge: Cambridge University Press. pp. 680–683. ISBN 978-0-521-57243-9.
- Herodotus. "Chapter 77, Book II". The Histories.
- Nunn JF (2002). "Ancient Egyptian medicine". Transactions of the Medical Society of London. University of Oklahoma Press. 113: 57–68. PMID 10326089.
- Breasted JH (1930). \The Edwin Smith Surgical Papyrus. University of Chicago Press.
- "Edwin Smith papyrus – Britannica Online Encyclopedia". Britannica.com. Retrieved 2022-10-12.
- Griffith FL (1898). The Petrie Papyri: Hieratic Papyri from Kahun and Gurob (principally of the Middle Kingdom). B. Quaritch.
- Bynum WF, Hardy A, Jacyna S, Lawrence C, Tansey EM (2006). "The Rise of Science in Medicine, 1850–1913". The Western Medical Tradition: 1800–2000. Cambridge University Press. pp. 198–99. ISBN 978-0-521-47565-5.
- "The Kahun Gynaecological Papyrus". Reshafim.org.il. Archived from the original on 19 April 2012. Retrieved 2012-04-21.
- "Museum: House of Life". www.ucl.ac.uk. Retrieved 2017-02-17.
- Magner L (1992). A History of Medicine. Boca Raton, Florida: CRC Press. p. 31. ISBN 978-0-8247-8673-1.
- Selin H, Shapiro H, eds. (2003). Medicine Across Cultures: History and Practice of Medicine in Non-Western Cultures. Dordrecht: Springer Science & Business Media. p. 35. ISBN 978-0-306-48094-2.
- Ghalioungui P (1975). "Les plus anciennes femmes-médecins de l'histoire". Bulletin de l'Institut Français d'Archéologie Orientale. Institut Français d'Archéologie Orientale du Caire. 75: 159–164.
- Black J, Anthony G (1992). Gods, Demons and Symbols of Ancient Mesopotamia: An Illustrated Dictionary. The British Museum Press. p. 102. ISBN 978-0-7141-1705-8.
- McIntosh JR (2005). Ancient Mesopotamia: New Perspectives. Santa Barbara, California, Denver, Colorado, and Oxford, England: ABC-CLIO. pp. 273–76. ISBN 978-1576079669.
- Farber W (1995). Witchcraft, Magic, and Divination in Ancient Mesopotamia. Civilizations of the Ancient Near East. Vol. 3. New York: Charles Schribner's Sons, MacMillan Library Reference, Simon & Schuster MacMillan. pp. 1891–908. ISBN 978-0-684-19279-6. Retrieved 2018-05-12.
- Abusch T (2002). Mesopotamian Witchcraft: Towards a History and Understanding of Babylonian Witchcraft Beliefs and Literature. Leiden, The Netherlands: Brill. p. 56. ISBN 978-90-04-12387-8.
- Brown M (1995). Israel's Divine Healer. Grand Rapids, Michigan: Zondervan. p. 42. ISBN 978-0-310-20029-1.
- Biggs RD (2005). "Medicine, Surgery, and Public Health in Ancient Mesopotamia". Journal of Assyrian Academic Studies. 19 (1): 7–18.
- "Geography – Mesopotamia". History of Humanity. Archived from the original on 2018-11-27. Retrieved 2018-12-19.
- Horstmanshoff HF, Van Tilburg CR, Stol M (2004). Magic and Rationality in Ancient Near Eastern and Graeco-Roman Medicine. Leiden: Brill. ISBN 978-90-04-13666-3.
- Heeßel NP (2004). "Diagnosis, Divination, and Disease: Towards an Understanding of the Rationale Behind the Babylonian Diagonostic Handbook". In Horstmanshoff HF, Stol M, Tilburg C (eds.). Magic and Rationality in Ancient Near Eastern and Graeco-Roman Medicine. Studies in Ancient Medicine. Vol. 27. Leiden, The Netherlands: Brill. pp. 97–116. ISBN 978-90-04-13666-3.
- Stol M (1993). Epilepsy in Babylonia. Groningen: STYX Publications. p. 55. ISBN 978-90-72371-63-8.
- Nemet-Nejat KR (1998). Daily Life in Ancient Mesopotamia. Daily Life. Santa Barbara, California: Greenwood. pp. 80–81. ISBN 978-0-313-29497-6.
- Syros V (2013). "Galenic Medicine and Social Stability in Early Modern Florence and the Islamic Empires". Journal of Early Modern History. 17 (2): 161–213. doi:10.1163/15700658-12342361 – via Academic Search Premier.
- Stelmack RM, Stalikas A (1991). "Galen and the Humor Theory of Temperament". University of Ottawa. 12: 255–63 – via Science Direct.
- Barber N (2012). Medieval Medicine. Heinemann-Raintree Library. p. 13. ISBN 978-1-4109-4661-4.
- Pormann PE, Savage-Smith E (2007). Medieval Islamic Medicine. pp. 41–75. ISBN 978-1-58901-160-1.
- Homer. Iliad. p. Bk XI:804–48.
- Risse GB (1990). Mending bodies, saving souls: a history of hospitals. Oxford University Press. p. 56. ISBN 978-0-19-974869-3.
- Askitopoulou H, Konsolaki E, Ramoutsaki I, Anastassaki E (2002). Carlos Diz J, Franco A, Bacon DR, Julián Alvarez JR (eds.). Surgical cures by sleep induction as the Asclepieion of Epidaurus. The history of anesthesia: proceedings of the Fifth International Symposium. - International Congress Series 1242. Elsevier Science B.V. pp. 11–17. ISBN 978-0-444-51293-2.
- "Alcmaeon". Stanford University. 10 June 2013. Retrieved 30 December 2015.
- Hanson AE. "Hippocrates: The "Greek Miracle" in Medicine". www.medicinaantiqua.org.uk. Ann Arbor: The University of Michigan. Archived from the original on 2008-02-15. Retrieved 2008-03-08.
- "The Father of Modern Medicine: Hippocrates". 2008-02-28. Archived from the original on 2008-02-28. Retrieved 2012-04-21.
- Porter R (1998) [1997]. The greatest benefit to mankind : a medical history of humanity 1946–2002 (1st American ed.). New York: W.W. Norton. ISBN 978-0-393-04634-2. OCLC 38410525.
- "What is finger clubbing?". Cancer Research UK. Retrieved 30 December 2015.
- Shakespeare W. Henry V. p. Act II, Scene 3.
- Silverberg R (1967). The dawn of medicine. Putnam. Retrieved 16 January 2013.
- Loudon I (2002). Western Medicine: An Illustrated History. Oxford University Press. ISBN 978-0-19-924813-1. Retrieved 16 January 2013.
- Hajar R (July 2012). "The air of history: early medicine to galen (part I)". Heart Views. 13 (3): 120–8. doi:10.4103/1995-705X.102164. PMC 3503359. PMID 23181186.
- Aird WC (July 2011). "Discovery of the cardiovascular system: from Galen to William Harvey". Journal of Thrombosis and Haemostasis. 9 (Suppl 1): 118–29. doi:10.1111/j.1538-7836.2011.04312.x. PMID 21781247. S2CID 12092592.
- Mattern SP (2013). The Prince of Medicine: Galen in the Roman Empire. ISBN 978-0-19-998615-6.
- Siegel RE (1968). Galen's System of Physiology and Medicine: an analysis of his doctrines and observations on bloodflow, respiration, humors and internal diseases. Basel: S. Karger. ISBN 978-3-8055-1016-5.
- Wallis F (2010). Medieval Medicine: A Reader. pp. 14, 26, 222. ISBN 978-1-4426-0103-1.
- Numbers R (2009). Galileo Goes to Jail and Other Myths About Science and Religion. Harvard University Press. p. 45. ISBN 978-0-674-03327-6.
- Shwayder M (7 April 2011). "Debunking a myth". The Harvard Gazette.
- "Surgical Instruments from Ancient Rome". Healthsystem.virginia.edu. Archived from the original on 2008-01-31. Retrieved 2012-04-21.
- "Roman period surgery set on show". BBC.
- Greenhill WA (1875). "Chirurgia". In Smith W (ed.). A Dictionary of Greek and Roman Antiquities. London: John Murray.]
- Elliott J (9 February 2008). "The Romans carried out cataract ops". BBC News.
- "Greek Medicine". US National Institutes of Health. 16 September 2002. Retrieved 29 August 2014.
- "Project MUSE – Journal of Late Antiquity – Volume 8, Number 2, Fall 2015". muse.jhu.edu. Retrieved 2020-01-12.
- Day CL (1967). Quipus and Witches' Knots. Lawrence, Kansas: University of Kansas Press. pp. 86–89, 124–26.
- Longrigg J (1993). Greek Rational Medicine: Philosophy and Medicine from Alcmaeon to the Alexandrians. Psychology Press. ISBN 978-0-415-02594-2. Retrieved 16 January 2013.
- Galen (2000). On the Natural Faculties, Books I, II, and III. Harvard: Loeb Classical Library.
- Vallance JT (April 1993). "Herophilus: The Art of Medicine in Early Alexandria". Ancient Philosophy (1): 237–241. doi:10.5840/ancientphil199313163.
- "Herophilus (Alexandrian physician)". Encyclopædia Britannica Online. Encyclopædia Britannica Inc. 2020.
- Mason SF (1962). A History of the Sciences (New rev. ed.). New York: Collier Books. p. 57. ISBN 978-0-02-093400-4.
- "The Case of Conjoined Twins in 10th Century Byzantium". Medievalists.net. 4 January 2014.
- Montandon D (2015). "The unspeakable history of thoracopagus twins' separation" (PDF). ISAPS News. 3: 46–49.
- Cambridge History of Iran Volume 4. Cambridge University Press. 1968. p. 396. ISBN 978-0-521-20093-6.
- Cyril E (1951). A medical history of Persia. Cambridge University Press. p. 173.
- Dols MW (1987). "The origins of the Islamic hospital: myth and reality". Bulletin of the History of Medicine. 61 (3): 367–390. JSTOR 44442098. PMID 3311248.
- Hamarneh S (July 1962). "Development of hospitals in Islam". Journal of the History of Medicine and Allied Sciences. 17 (3): 366–384. doi:10.1093/jhmas/xvii.3.366. PMID 13904051.
- Khalidi T. "Abd al-Malik | Caliph, Achievements, Coinage, & Dome of the Rock". Britannica. Retrieved 2021-11-23.
- Lapidus IM (October 1975). "The Separation of State and Religion in the Development of Early Islamic Society". International Journal of Middle East Studies. 6 (4): 363–385. doi:10.1017/s0020743800025344. ISSN 0020-7438. S2CID 162409061.
- Hajar R (January 2013). "The Air of History Part III: The Golden Age in Arab Islamic Medicine An Introduction". Heart Views. 14 (1): 43–46. doi:10.4103/1995-705X.107125. PMC 3621228. PMID 23580929.
- Masoud MT, Masoud F (January 2006). "How Islam changed medicine: Ibn al-Haytham and optics". BMJ. 332 (7533): 120. doi:10.1136/bmj.332.7533.120-a. PMC 1326979. PMID 16410601.
- Meri JW, Bacharach JL (2016). Medieval Islamic civilization: an encyclopedia. Volume I, A-K, Index. Abingdon, Oxon: Routledge. p. 783. ISBN 978-1-315-16244-7.
- Sarton G. Introduction to the History of Science.
(cf. Zahoor A, Haq Z (1997). "Quotations From Famous Historians of Science". Cyberistan. - Parker S (2013). Kill or cure: an illustrated history of medicine (First American ed.). New York, New York. ISBN 978-1-4654-0842-6.
- Becka J (January 1980). "[The father of medicine, Avicenna, in our science and culture. Abu Ali ibn Sina (980-1037)]". Casopis Lekaru Ceskych (in Czech). 119 (1): 17–23. PMID 6989499.
- "Avicenna 980–1037". Hcs.osu.edu. Archived from the original on October 7, 2008. Retrieved 2010-01-19.
- ""The Canon of Medicine" (work by Avicenna)". Encyclopædia Britannica. 2008. Archived from the original on 28 May 2008. Retrieved 11 Jun 2008.
- Musallam B (30 December 2012). "Avicenna: Medicine and Biology". Encyclopedia Iranica. pp. 94–99. Retrieved 20 December 2013.
- Tschanz DW (2003). "Arab(?) Roots of European Medicine". Heart Views. 4 (2). Archived from the original on 2004-05-03. Retrieved 2019-03-04.
- Pormann PE, Savage-Smith (2007). "On the dominance of the Greek humoral theory, which was the basis for the practice of bloodletting, in medieval Islamic medicine". Medieval Islamic medicine. Washington DC: Georgetown University. pp. 10, 43–45. OL 12911905W.
- Iskandar A (2006). "Al-Rāzī". Encyclopaedia of the history of science, technology, and medicine in non-western cultures (2nd ed.). Springer. pp. 155–56.
- Ganchy S (2009). Islam and Science, Medicine, and Technology (1st ed.). New York, NY: Rosen Pub. ISBN 978-1-4358-5679-0.
- Tschanz DW (2003). "Arab(?) Roots of European Medicine". Heart Views. 4 (2).
- Elgood C (2010). A Medical History of Persia and The Eastern Caliphate (1st ed.). London: Cambridge. pp. 202–03. ISBN 978-1-108-01588-2.
By writing a monograph on 'Diseases in Children' he may also be looked upon as the father of paediatrics.
- Majeed A (December 2005). "How Islam changed medicine". BMJ (Clinical Research Ed.). 331 (7531): 1486–7. doi:10.1136/bmj.331.7531.1486. PMC 1322233. PMID 16373721.
- Speziale F, ed. (2012). "The Hospital and Other Muslim Institutions [Introduction]". Hospitals in Iran and India, 1500-1950s. Leiden, NV: Brill. pp. 2–4. ISBN 978-90-04-22829-0.
- Barker P (2020). History of Science in the Persianate World. Lecture (Report).
- Porter R (October 1999). The Greatest Benefit to Mankind. A medical history of humanity. The Norton History of Science. WW Norton & Company. pp. 106–134. ISBN 978-0-393-31980-4.
- Sharpe WD (January 1964). "Isidore of Seville: The Medical Writings, An English Translation with an Introduction and Commentary". Transactions of the American Philosophical Society. 54 (2): 1–75. doi:10.2307/1005938. JSTOR 1005938.
- McKitterick R (2005). "The Carolingian Renaissance of Culture and Learning". In Story J (ed.). Charlemagne: Empire and Society. Manchester: Manchester University Press. ISBN 978-0-7190-7089-1.
- Wallis F (2010). Medieval Medicine: A Reader. Toronto: University of Toronto Press. p. 361. ISBN 978-1-4426-0423-0.
- Vecchio I, Tornali C, Rampello L, Rampello L, Migliore M, Silvia G, Rigo GA (January 2013). "Jewish medicine and surgery in Catania, Italy before 1492" (PDF). Acta Medica Mediterranea. 29: 359–362.
- Vecchio I, Di Mauro S, Tornali C, Rampello L, Migliore M, Rampello L, Rigo GS, Castellino P (January 2012). "Jewish medicine and surgery in sicily before 1492" (PDF). Acta Medica Mediterranea. 28: 77–82.
- Siraisi NG (May 2009). M Medieval and Early Renaissance Medicine: An Introduction to Knowledge and Practice. University of Chicago Press. p. 21. ISBN 978-0-226-76131-2.
- Bylebyl JJ (1979). "Chapter 10: The School of Padua: humanistic medicine in the 16th century". Health, Medicine and Mortality in the Sixteenth Century. Cambridge [England]: Cambridge University Press. ISBN 978-0-521-22643-1.
- Lo Presti R (2010). "Anatomy as Epistemology: The Body of Man and the Body of Medicine in Vesalius and his Ancient Sources (Celsus, Galen)". Renaissance and Reformation/Renaissance et Reforme. 33 (3): 27–60.
- Taitz E, Henry S, Tallan C (2003). The JPS Guide to Jewish Women: 600 B.C.E.to 1900 C.E. Philadelphia: The Jewish Publication Society. ISBN 978-0-8276-0752-1.
- Pelling M, Webster C (November 1979). "Medical Practitioners". Health, Medicine, and Mortality in the Sixteenth Century. CUP Archive. p. 183.
- Siraisi NG (September 2012). "Medicine, 1450-1620, and the history of science". Isis. 103 (3): 491–514. doi:10.1086/667970. PMID 23286188. S2CID 6954963.
- Lane N (April 2015). "The unseen world: reflections on Leeuwenhoek (1677) 'Concerning little animals'". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 370 (1666): 20140344. doi:10.1098/rstb.2014.0344. PMC 4360124. PMID 25750239.
- Madigan M, Martinko J, eds. (2006). Brock Biology of Microorganisms (11th ed.). Prentice Hall. ISBN 978-0131443297.
- Lines DA (2012). "Reorganizing the Curriculum: Teaching and Learning in the University of Bologna, c. 1560–1590". History of Universities. 25 (2): 1–59.
- Gurunluoglu R, Shafighi M, Gurunluoglu A, Cavdar S (May 2011). "Giulio Cesare Aranzio (Arantius) (1530-89) in the pageant of anatomy and surgery". Journal of Medical Biography. 19 (2): 63–69. doi:10.1258/jmb.2010.010049. PMID 21558532. S2CID 10833758.
- Fissell ME (2008). "Introduction: women, health, and healing in early modern Europe". Bulletin of the History of Medicine. 82 (1): 1–17. doi:10.1353/bhm.2008.0024. PMID 18344583. S2CID 37622681.
- Green M (1989). "Women's Medical Practice and Health Care in Medieval Europe". Signs. 14 (2): 434–74. doi:10.1086/494516. PMID 11618104. S2CID 38651601.
- Dixon CS, Freist D, Greengrass M, eds. (2009). Living With Religious Diversity in Early-Modern Europe. Ashgate. pp. 128–130. ISBN 978-0-7546-6668-4.
- Leonard AE (2006). "Female Religious Orders". In Hsia RP (ed.). A companion to the Reformation world. Oxford: Blackwell. pp. 237–254. ISBN 978-1-4051-7865-5.
- Cunningham A, Grell OP (2002). Health Care and Poor Relief in Protestant Europe 1500–1700. Routledge. pp. 130–33. ISBN 978-0-203-43134-4.
- Mäkinen V (2006). Lutheran Reformation and the Law. Brill. pp. 227–29. ISBN 978-90-04-14904-5.
- Waddington K (2003). Medical Education at St. Bartholomew's Hospital, 1123–1995. Boydell & Brewer. p. 18. ISBN 978-0-85115-919-5.
- Harkness DE (2008). "A view from the streets: women and medical work in Elizabethan London". Bulletin of the History of Medicine. 82 (1): 52–85. doi:10.1353/bhm.2008.0001. PMID 18344585. S2CID 5695475.
- McHugh T (July 2012). "Expanding women's rural medical work in early modern Brittany: the Daughters of the Holy Spirit". Journal of the History of Medicine and Allied Sciences. 67 (3): 428–456. doi:10.1093/jhmas/jrr032. PMC 3376001. PMID 21724643.
- Broman TH (2003–2020). "The Medical Sciences". The Cambridge History of Science. Vol. 4, Eighteenth-Century Science. Cambridge. pp. 465–468. ISBN 978-0-521-57243-9.
- Rosner L (1991). Medical Education in the Age of Improvement: Edinburgh Students and Apprentices 1760-1826. Edinburgh: Edinburgh University Press. ISBN 978-0-7486-0245-2.
- Altman I (2003). The Early History of Greater Mexico. Upper Saddle River, N.J.: Prentice Hall. p. 99. ISBN 978-0-13-091543-6.
- Cook SF (1946). "The Incidence of Disease Among the Aztecs and Related Tribes". Hispanic American Historical Review. 36: 32–35.
- Cook ND (1998). Born to Die: Disease and New World Conquest, 1492-1650. Cambridge: Cambridge University Press. ISBN 978-0-521-62730-6.
- Schendel G, Amézquita JA, Bustamante ME (2014). Medicine in Mexico: From Aztec Herbs to Betatrons. University of Texas Press. p. 99. ISBN 978-1-4773-0636-9.
- Lanning JT (1985). The Royal Protomedicato: The Regulation of the Medical Professions in the Spanish Empire. Durham: Duke University Press. ISBN 978-0-8223-0651-1.
- Burke ME (1977). The Royal College of San Carlos: surgery and Spanish medical reform in the late eighteenth century. Durham, N.C.: Duke University Press. ISBN 978-0-8223-0382-4.
- Cooper DB (1965). Epidemic Disease in Mexico City, 1761–1813: An Administrative, Social, and Medical Study (LLILAS Latin American Monograph Series). Austin: University of Texas Press. ISBN 978-1-4773-0575-1.
- Voekel P (2002). "Chapter 7: The Rise of Medical Empiricism". Alone Before God: The Religious Origins of Modernity in Mexico. Durham: Duke University Press. ISBN 978-0-8223-8429-8.
- De Vos P (2006). "The Science of Spices: Empiricism and Economic Botany in the Early Spanish Empire". Journal of World History. 17 (4): 399–427. doi:10.1353/jwh.2006.0054. ISSN 1045-6007. JSTOR 20079398. S2CID 201793405.
- Frank AG (1998). ReOrient: global economy in the Asian Age. Berkeley: University of California Press. pp. 96–100. ISBN 978-0-520-92131-3. OCLC 42922426.
- de Bernardino S (2006). Historia general de las cosas de Nueva España [General History of the Things of New Spain]. The Florentine Codex (in Spanish) (11th ed.). México: Editorial Porrúa. ISBN 978-9-70-07649-24.
- Davis MM, Warner AR (1918). Dispensaries, Their Management and Development: A Book for Administrators, Public Health Workers, and All Interested in Better Medical Service for the People. MacMillan. pp. 2–5.
- Kirkup J (February 1996). "Samuel Sharp and the Operations of Surgery, 1739". Journal of Medical Biography. 4 (1): 1–7. doi:10.1177/096777209600400101. PMID 11615341. S2CID 26133970.
- Waddington I (January 1975). "The development of medical ethics -a sociological analysis". Medical History. 19 (1): 36–51. doi:10.1017/s002572730001992x. PMC 1081608. PMID 1095851.
- "The Global Public–Private Partnership for Handwashing". globalhandwashing.org. 19 March 2015. Retrieved 2015-04-18.
- Guénel A (January 1999). "The creation of the first overseas Pasteur Institute, or the beginning of Albert Calmette's Pastorian career". Medical History. 43 (1): 1–25. doi:10.1017/s0025727300064693. PMC 1044108. PMID 10885131.
- Morabia A (December 2007). "Epidemiologic interactions, complexity, and the lonesome death of Max von Pettenkofer". American Journal of Epidemiology. 166 (11): 1233–1238. doi:10.1093/aje/kwm279. PMID 17934200.
Oppenheimer GM, Susser E (December 2007). "Invited commentary: The context and challenge of von Pettenkofer's contributions to epidemiology". American Journal of Epidemiology. 166 (11): 1239–41, discussion 1241–43. doi:10.1093/aje/kwm284. PMID 17934199. - Blevins SM, Bronze MS (September 2010). "Robert Koch and the 'golden age' of bacteriology". International Journal of Infectious Diseases. 14 (9): e744–e751. doi:10.1016/j.ijid.2009.12.003. PMID 20413340.
- Baly MF (2002). Nursing and Social Change. Routledge. p. 113. ISBN 978-0203424872.
- Donahue MP (2011). Nursing, The Finest Art: An Illustrated History (3rd ed.). Maryland Heights, Mo.: Mosby Elsevier. pp. 112–125. ISBN 978-0-323-05305-1.
- Magnello ME (2012). "Victorian statistical graphics and the iconography of Florence Nightingale's polar area graph". BSHM Bulletin. 27 (1): 13–37. doi:10.1080/17498430.2012.618102. S2CID 121655727.
- Gunn SW, Masellis M (2008). Concepts and Practice of Humanitarian Medicine. New York: Springer Science & Business Media. pp. 87–. ISBN 978-0-387-72264-1.
- Ball L (May 2009). "Cholera and the pump on Broad Street: The life and legacy of John Snow" (PDF). The History Teacher. 43 (1): 105–119.
- Everitt BS, Palmer C (2011). Encyclopaedic Companion to Medical Statistics. Wiley. pp. 447–48. ISBN 978-1119957409.
- He also built the New York Public Library
- Cassedy JH (1992). "Numbering the North's medical events: humanitarianism and science in Civil War statistics". Bulletin of the History of Medicine. 66 (2): 210–233. PMID 1290489.
- Porter R (1999). The Greatest Benefit to Mankind: A Medical History of Humanity from Antiquity to the Present. London: Fontana. p. 493. ISBN 978-0393319804.; Porter R (1992). "Madness and its Institutions". In Wear A (ed.). Medicine in Society: Historical Essays. Cambridge: Cambridge University Press. pp. 277–302. ISBN 978-0521336390.; Suzuki A (December 1991). "Lunacy in seventeenth- and eighteenth-century England: analysis of Quarter Sessions records. Part I". History of Psychiatry. 2 (8): 437–456. doi:10.1177/0957154X9100200807. PMID 11612606. S2CID 2250614.; Suzuki A (March 1992). "Lunacy in seventeenth- and eighteenth-century England: analysis of Quarter Sessions records. Part II". History of Psychiatry. 3 (9): 29–44. doi:10.1177/0957154X9200300903. PMID 11612665. S2CID 28734153.
- Porter R (1992). "Madness and its Institutions". In Wear A (ed.). Medicine in Society: Historical Essays. Cambridge: Cambridge University Press. pp. 277–302. ISBN 978-0521336390.; Goldstein J (2001) [1987]. Console and Classify: The French Psychiatric Profession in the Nineteenth Century. Chicago & London: University of Chicago Press. p. 42. ISBN 978-0226301600.; Grob GN (1994). Mad Among Us. Simon and Schuster. pp. 25–30. ISBN 978-1439105719.
- Porter R (2004). Madmen: a social history of madhouses, mad-doctors & lunatics. Tempus. pp. 57–76, 239–44, 257–312. ISBN 978-0752437309.; Hayward R (2011). "Medicine and the Mind". In Jackson M (ed.). The Oxford Handbook of the History of Medicine. Oxford University Press. pp. 524–42. ISBN 978-0199546497.
- Bynum WF (October 1974). "Rationales for therapy in British psychiatry: 1780-1835". Medical History. 18 (4): 317–334. doi:10.1017/s0025727300019761. PMC 1081592. PMID 4618306.; Digby A (1988). "Moral Treatment at the Retreat 1796–1846". In Porter R, Bynum WF, Shepherd M (eds.). The Anatomy of Madness: Essays in the History of Psychiatry. Vol. 2. London & New York: Tavistock. pp. 52–71. ISBN 978-0415008594.
- Weiner DB (1994). " 'La geste du Pinel': The History of a Psychiatric Myth". In Micale MS, Porter R (eds.). Discovering the History of Psychiatry. New York & Oxford: Oxford University Press. pp. 232–47. ISBN 978-0195077391.
- Porter R (1992). "Madness and its Institutions". In Wear A (ed.). Medicine in Society: Historical Essays. Cambridge: Cambridge University Press. pp. 277–302. ISBN 978-0521336390.
- Marx OM (1994). "The Beginning of Psychiatric Historiography in Nineteenth-Century Germany". In Micale MS, Porter R (eds.). Discovering the History of Psychiatry. New York & Oxford: Oxford University Press. pp. 39–51. ISBN 978-0195077391.
- Hayward R (2011). "Medicine and the Mind". In Jackson M (ed.). The Oxford Handbook of the History of Medicine. Oxford University Press. pp. 524–42. ISBN 978-0199546497.
- Andrews J (2004). "The Rise of the Asylum in Britain". In Brunton D (ed.). Medicine Transformed: Health, Disease and Society in Europe 1800–1930. Manchester University Press. pp. 298–330. ISBN 978-0719067358.; Porter R (2003). "Introduction". In Porter R, Wright D (eds.). The Confinement of the Insane: International Perspectives, 1800–1965. Cambridge University Press. pp. 1–19. ISBN 978-1139439626.
- Cooter RJ (January 1976). "Phrenology and British alienists, c. 1825-1845. Part I: Converts to a doctrine". Medical History. 20 (1): 1–21. doi:10.1017/s0025727300021761. PMC 1081688. PMID 765647.; Cooter RJ (April 1976). "Phrenology and British alienists, c.1825-1845. Part II: Doctrine and practice". Medical History. 20 (2): 135–151. doi:10.1017/s0025727300022195. PMC 1081733. PMID 781421.
- Shorter E (1997). A history of psychiatry: from the era of the asylum to the age of Prozac. John Wiley & Sons. pp. 46–48. ISBN 978-0471157496.; Bynum WF, Hardy A, Jacyna S, Lawrence C, Tansey EM (2006). "The Rise of Science in Medicine, 1850–1913". The Western Medical Tradition: 1800–2000. Cambridge University Press. pp. 198–99. ISBN 978-0521475655.
- Pick D (1993). Faces of Degeneration: A European Disorder, c. 1848–1918. Cambridge University Press. ISBN 978-0521457538.
- Ray LJ (1981). "Models of madness in Victorian asylum practice". European Journal of Sociology. 22 (2): 229–264. doi:10.1017/S0003975600003714. PMID 11630885. S2CID 33924282.; Cox C (2012). Negotiating Insanity in the Southeast of Ireland, 1820–1900. Manchester University Press. pp. 54–55. ISBN 978-0719075032.; Malcolm E (2003). "'Ireland's Crowded Madhouses': The Institutional Confinement of the Insane in Nineteenth- and Twentieth-Century Ireland". In Porter R, Wright D (eds.). The Confinement of the Insane: International Perspectives, 1800–1965. Cambridge University Press. pp. 315–33. ISBN 978-1139439626.
- Hayward R (2011). "Medicine and the Mind". In Jackson M (ed.). The Oxford Handbook of the History of Medicine. Oxford University Press. pp. 524–42. ISBN 978-0199546497.; Scull A (2005). Most Solitary of Afflictions: Madness And Society in Britain, 1700–1900. Yale University Press. pp. 324–28. ISBN 978-0300107548.; Dowbiggin I (October 1992). ""An exodus of enthusiasm": G. Alder Blumer, eugenics, and US psychiatry, 1890-1920". Medical History. 36 (4): 379–402. doi:10.1017/S002572730005568X. PMC 1036631. PMID 1435019.; Snelders S, Meijman FJ, Pieters T (April 2007). "Heredity and alcoholism in the medical sphere: the Netherlands, 1850-1900". Medical History. 51 (2): 219–236. doi:10.1017/S0025727300001204. PMC 1871693. PMID 17538696.; Turda M (January 2009). ""To end the degeneration of a nation": debates on eugenic sterilization in inter-war Romania". Medical History. 53 (1): 77–104. doi:10.1017/S002572730000332X. PMC 2629178. PMID 19190750.
- Alexander C (2010). "The Shock of War". Smithsonian. 41 (5): 58–66.
- Berrios G, Porter R (1995). The History of Clinical Psychiatry:: The Origin and History of Psychiatric Disorders. London: Athlone Press. ISBN 978-0-485-24211-9.
- Markell Morantz R (1982). "Feminism, Professionalism and Germs: The Thought of Mary Putnam Jacobi and Elizabeth Blackwell". American Quarterly. 34 (5): 461–78. doi:10.2307/2712640. JSTOR 2712640.
- Eisler R (2007). The Real Wealth of Nations: Creating a Caring Economics. p. 78.
- van der Weiden RM, Uhlenbeck GC (May 2010). "European 18th-century obstetrical pioneers in Japan: a new light in the empire of the sun". Journal of Medical Biography. 18 (2): 99–101. doi:10.1258/jmb.2010.010006. PMID 20519709. S2CID 22701750.
- Ciriacono S (2010). "Scientific Transfer between Europe and Japan: The Influence of Dutch and German Medicine from the Edo Period to the Meiji Restoration". Comparativ: Leipziger Beiträge zur Universalgeschichte und Vergleichenden Gesellschaftsforschung. 20 (6): 134–53.
- Jannetta AB (2007). The Vaccinators: Smallpox, Medical Knowledge, and the 'Opening' of Japan. Stanford, California: Stanford University Press. ISBN 978-0-8047-7949-4.
- Byrne JP (2008). Encyclopedia of Pestilence, Pandemics, and Plagues. ABC-CLIO. p. 339. ISBN 978-0-313-34101-4.
- Linton DS (2005). Emil Von Behring: Infectious Disease, Immunology, Serum Therapy. American Philosophical Society. p. 57. ISBN 978-0871692559.
- Donzé PY (2010). "Making medicine a business in Japan: Shimadzu Co. and the diffusion of radiology (1900-1960)". Gesnerus. 67 (2): 241–262. doi:10.1163/22977953-06702004. PMID 21417169.
- Lynteris C (July 2011). "From Prussia to China: Japanese colonial medicine and Gotō Shinpei's combination of medical police and local self-administration". Medical History. 55 (3): 343–347. doi:10.1017/s0025727300005378. PMC 3143861. PMID 21792258.
- Liu MS (2009). Prescribing colonization : the role of medical practices and policies in Japan-ruled Taiwan, 1895-1945. Ann Arbor, Michigan: Association for Asian Studies. p. 286. ISBN 978-0-924304-57-6.
- Fissell ME (1991). "The Disappearance of the Patient's Narrative and the Invention of Hospital Medicine". In French R, Wear A (eds.). British Medicine in an Age of Reform. Routledge. ISBN 978-1-134-93531-4.
- Risse GB (1999). Mending bodies, saving souls: a history of hospitals. New York: Oxford University Press. ISBN 978-0-19-974869-3.
- Orr BJ (2013). Children of the Fasti. Lulu.com. p. 247. ISBN 978-1291389296.
- Morton HW (1984). The Contemporary Soviet City. M.E. Sharpe. pp. 142–45. ISBN 978-0873322485.
- Weiner DB, Sauter MJ (2003). "The city of Paris and the rise of clinical medicine". Osiris. 18 (1): 23–42. doi:10.1086/649375. PMID 12964569. S2CID 10692225.
- Reynolds MD (1994). How Pasteur Changed History: The Story of Louis Pasteur and the Pasteur Institute. Bradenton, Florida: McGuinn & McGuire. ISBN 978-1-881117-05-6.
- Weindling P (1992). "Scientific elites and laboratory organization in fin de siècle Paris and Berlin: The Pasteur Institute and Robert Koch's Institute for Infectious Diseases compared". In Cunningham A, Williams P (eds.). he Laboratory revolution in medicine. Cambridge: Cambridge University Press. pp. 170–188. ISBN 978-0-521-40484-6.
- Fichtner PS (2009). Historical Dictionary of Austria. Scarecrow Press. pp. 326–27. ISBN 978-0810863101.
- Lesky E (1988). "[Cabanis and certainty of medicine]". Gesnerus. 11 (3–4): 152–182. doi:10.1017/S0025727300070800. PMC 2557344. PMID 14366253.
- Lesky E (1976). The Vienna Medical School of the 19th century. Baltimore: Johns Hopkins University Press. ISBN 978-0-8018-1908-7.
- Adams GW, Wose CT (1999). "Doctors in Blue: The Medical History of the Union Army in the Civil War". RN Nursing History Review. 7 (1): 191–193. doi:10.1891/1062-8061.7.1.191. S2CID 154115154.
- Schroeder-Lein GR (2008). The encyclopedia of Civil War medicine. Armonk, N.Y.: M.E. Sharpe, Inc. ISBN 978-1-317-45710-7.
- Cunningham HH (November 2015). Doctors in Gray: The Confederate Medical Service. San Francisco: Golden Springs Publishing. ISBN 978-1-78625-121-3.
- Keegan J (17 Sep 2009). "The American Civil War: the gruesome suffering of soldiers exposed". Daily Telegraph. Archived from the original on 2022-01-12. Retrieved 4 March 2017.
- Link K (1983). "Potomac fever: the hazards of camp life" (PDF). Vermont History. 51 (2): 69–88. PMID 11633534.
- Gillett MC (1987). The Army Medical Department, 1818-1865. Center of Military History, US Army (Report).
- Gates A (February 1957). "Lincoln's Fifth Wheel: The Political History of the US Sanitary Commission". Civil War History. 3 (1): 97–98. doi:10.1353/cwh.1957.0048.
- Martin J (May 2011). "Heros Along with the Rest: Civil War Service, 1861–1863". Genius of place: the life of Frederick Law Olmsted. Da Capo Press. pp. 178–230. ISBN 978-0-306-82148-6.
- Farhud DD, Zarif Yeganeh M (2013). "A brief history of human blood groups". Iranian Journal of Public Health. 42 (1): 1–6. PMC 3595629. PMID 23514954.
- Legese B, Shiferaw M, Tamir W, Tiruneh T (2021). "Distribution of ABO and Rhesus Blood Group Phenotypes Among Blood Donors at Bahir Dar Blood Bank, Amhara, Northwest Ethiopia: A Retrospective Cross-Sectional Study". Journal of Blood Medicine. 12: 849–854. doi:10.2147/JBM.S329360. PMC 8454416. PMID 34557052.
- Levine P, Stetson RE (8 July 1939). "An unusual case of intra-group agglutination". Journal of the American Medical Association. 113 (2): 126. doi:10.1001/jama.1939.72800270002007a. ISSN 0002-9955.
- "Henry Norman Bethune Biography". Encyclopedia of World Biography. Thomson Corporation.
- Webb Jr LA (2009). Humanity's Burden: A Global History of Malaria. Cambridge: Cambridge University Press. ISBN 978-0-521-67012-8.
- Packard RM (2021). The Making of a Tropical Disease: A Short History of Malaria. Johns Hopkins Biographies of Disease (Second ed.). Baltimore. ISBN 978-1-4214-4179-5.
- Slater LB (2009). War and Disease: Biomedical Research on Malaria in the Twentieth Century. Critical Issues in Health and Medicine. New Brunswick, N.J.: Rutgers University Press. ISBN 978-0-8135-4438-0.
- Webb JL (July 2011). "The first large-scale use of synthetic insecticide for malaria control in tropical Africa: lessons from Liberia, 1945-1962". Journal of the History of Medicine and Allied Sciences. 66 (3): 347–76. doi:10.1093/jhmas/jrq046. PMID 20624820.
- Taubenberger JK, Morens DM (January 2006). "1918 Influenza: the mother of all pandemics". Emerging Infectious Diseases. 12 (1): 15–22. doi:10.3201/eid1209.05-0979. PMC 3291398. PMID 16494711.
- Bristow NK (2012). American Pandemic: The Lost Worlds of the 1918 Influenza Epidemic. Oxford University Press. ISBN 978-0-19-981151-9.
- Barry JM (2020). The Great Influenza: The Story of the Deadliest Pandemic in History. Penguin Books. ISBN 978-0-241-99157-2.
- Van Hartesveldt FR (2010). "The Doctors and the 'Flu': The British Medical Profession's Response to the Influenza Pandemic of 1918–19". International Social Science Review. 85 (1): 28–39. JSTOR 41887429.
- Murray JE (January 2005). "The first successful organ transplants in man". Journal of the American College of Surgeons. 200 (1): 5–9. doi:10.1016/j.jamcollsurg.2004.09.033. PMID 15631913.
- Katz F (1998). The life and times of Pancho Villa. Stanford, California: Stanford University Press. ISBN 978-0-8047-3046-4.
- Hutchinson JF (1996). Champions of charity: war and the rise of the Red Cross. Bulletin of the History of Medicine. Vol. 86. Boulder: Westview Press. pp. 37–65. doi:10.1353/bhm.2012.0011. ISBN 978-0-429-50177-7. PMID 22643983. S2CID 10431895.
- Irwin JF (2012). "Sauvons les Bébés: child health and U.S. humanitarian aid in the First World War era". Bulletin of the History of Medicine. 86 (1): 37–65. doi:10.1353/bhm.2012.0011. PMID 22643983. S2CID 10431895.
- Harrison M (2004). Medicine and Victory: British Military Medicine in the Second World War. Oxford: Oxford University Press. p. 275. ISBN 978-0-19-151496-8.
- Harrison M (2010). The medical war: British military medicine in the First World War. Oxford: Oxford University Press. ISBN 978-0-19-957582-4.
- Freyhofer HH (2004). The Nuremberg Medical Trial: the Holocaust and the origin of the Nuremberg medical code. New York: P. Lang. ISBN 978-0-8204-6797-9.
- Nie JB, Guo N, Selden M, Kleinman A (2010). Japan's Wartime Medical Atrocities: Comparative Inquiries in Science, History, and Ethics. London: Routledge. ISBN 978-1-136-95260-9.
- Hutchings MI, Truman AW, Wilkinson B (October 2019). "Antibiotics: past, present and future". Current Opinion in Microbiology. 51: 72–80. doi:10.1016/j.mib.2019.10.008. PMID 31733401. S2CID 208086151.
- Dadgostar P (2019-12-20). "Antimicrobial Resistance: Implications and Costs". Infection and Drug Resistance. 12: 3903–3910. doi:10.2147/IDR.S234610. PMC 6929930. PMID 31908502.
- Soulsby L (August 2007). "Antimicrobials and animal health: a fascinating nexus". The Journal of Antimicrobial Chemotherapy. 60 (suppl_1): i77–i78. doi:10.1093/jac/dkm164. PMID 17656389.
- Gibb R, Redding DW, Chin KQ, Donnelly CA, Blackburn TM, Newbold T, Jones KE (August 2020). "Zoonotic host diversity increases in human-dominated ecosystems". Nature. 584 (7821): 398–402. Bibcode:2020Natur.584..398G. doi:10.1038/s41586-020-2562-8. PMID 32759999. S2CID 220975813.
- Tollefson J (August 2020). "Why deforestation and extinctions make pandemics more likely". Nature. 584 (7820): 175–176. Bibcode:2020Natur.584..175T. doi:10.1038/d41586-020-02341-1. PMID 32770149. S2CID 221109844.
- Spernovasilis N, Markaki I, Papadakis M, Tsioutis C, Markaki L (December 2021). "Epidemics and pandemics: Is human overpopulation the elephant in the room?". Ethics, Medicine, and Public Health. 19: 100728. doi:10.1016/j.jemep.2021.100728. PMC 8530531. PMID 34703871.
- Hui DS (August 2013). "Severe acute respiratory syndrome (SARS): lessons learnt in Hong Kong". Journal of Thoracic Disease. 5 (Suppl 2): S122–S126. doi:10.3978/j.issn.2072-1439.2013.06.18. PMC 3747521. PMID 23977432.
- Garske T, Legrand J, Donnelly CA, Ward H, Cauchemez S, Fraser C, et al. (July 2009). "Assessing the severity of the novel influenza A/H1N1 pandemic". BMJ. 339 (jul14 3): b2840. doi:10.1136/bmj.b2840. PMID 19602714. S2CID 26484486.
- The Lancet (June 2021). "40 years of HIV/AIDS: a painful anniversary". Lancet. 397 (10290): 2125. doi:10.1016/S0140-6736(21)01213-7. PMID 34087107.
- Thoueille P, Choong E, Cavassini M, Buclin T, Decosterd LA (February 2022). "Long-acting antiretrovirals: a new era for the management and prevention of HIV infection". The Journal of Antimicrobial Chemotherapy. 77 (2): 290–302. doi:10.1093/jac/dkab324. PMC 8809192. PMID 34499731.
- Abdool Karim Q, Sibeko S, Baxter C (May 2010). "Preventing HIV infection in women: a global health imperative". Clinical Infectious Diseases. 50 (Suppl 3): S122–S129. doi:10.1086/651483. PMC 3021824. PMID 20397940.
- Deutsch MB (October 2018). "Pre-Exposure Prophylaxis in Trans Populations: Providing Gender-Affirming Prevention for Trans People at High Risk of Acquiring HIV". LGBT Health. 5 (7): 387–390. doi:10.1089/lgbt.2018.0086. PMID 30272493. S2CID 52891606.
- Challacombe SJ (September 2020). "Global inequalities in HIV infection". Oral Diseases. 26 (Suppl 1): 16–21. doi:10.1111/odi.13386. PMID 32862524. S2CID 221385357.
- Cucinotta D, Vanelli M (March 2020). "WHO Declares COVID-19 a Pandemic". Acta Bio-Medica. 91 (1): 157–160. doi:10.23750/abm.v91i1.9397. PMC 7569573. PMID 32191675.
- Chowdhury JM, Patel M, Zheng M, Abramian O, Criner GJ (August 2020). "Mobilization and Preparation of a Large Urban Academic Center during the COVID-19 Pandemic". Annals of the American Thoracic Society. 17 (8): 922–925. doi:10.1513/AnnalsATS.202003-259PS. PMC 7393784. PMID 32315201.
- Pearce AP, Naumann DN, O'Reilly D (February 2021). "Mission command: applying principles of military leadership to the SARS-CoV-2 (COVID-19) crisis". BMJ Military Health. 167 (1): 3–4. doi:10.1111/1468-5973.12328. PMC 7537208. PMID 32303574.
- Goetz LH, Schork NJ (June 2018). "Personalized medicine: motivation, challenges, and progress". Fertility and Sterility. 109 (6): 952–963. doi:10.1016/j.fertnstert.2018.05.006. PMC 6366451. PMID 29935653.
- Denford S, Frost J, Dieppe P, Cooper C, Britten N (March 2014). "Individualisation of drug treatments for patients with long-term conditions: a review of concepts". BMJ Open. 4 (3): e004172. doi:10.1136/bmjopen-2013-004172. PMC 3975745. PMID 24670429.
- Arjmand B, Goodarzi P, Mohamadi-Jahani F, Falahzadeh K, Larijani B (March 2017). "Personalized Regenerative Medicine". Acta Medica Iranica. 55 (3): 144–149. PMID 28282715.
- Williams DR, Rucker TD (2000). "Understanding and addressing racial disparities in health care". Health Care Financing Review. 21 (4): 75–90. PMC 4194634. PMID 11481746.
- Hamed S, Bradby H, Ahlberg BM, Thapar-Björkert S (May 2022). "Racism in healthcare: a scoping review". BMC Public Health. 22 (1): 988. doi:10.1186/s12889-022-13122-y. PMC 9112453. PMID 35578322.
Further reading
- Bowers BS, ed. (2007). The Medieval Hospital and Medical Practice. Ashgate. p. 258. ISBN 978-0-7546-5110-9.
- Breslaw EG (2014). Lotions, Potions, Pills, and Magic: Health Care in Early America. ISBN 978-1479807048.
- Brockliss LW, Jone C (1997). The Medical World of Early Modern France. Oxford: Clarendon Press. ISBN 978-0-19-822750-2.
- Burnham JC, ed. (2015). Health Care in America: A History. Baltimore: JHU Press. ISBN 978-1-4214-1609-0.
- Bynum WF, Porter R, eds. (1993). Companion Encyclopedia of the History of Medicine. London: Routledge. ISBN 978-1-136-11036-8.
- Bynum WF, Hardy A, Jacyna S, Lawrence C, Tansey EM (2006). The Western Medical Tradition. New York, NY: Cambridge University Press. ISBN 978-0-521-47565-5.
- Conrad LI, Neve M, Nutton V, Porter R, Wear A (1995). The Western Medical Tradition: 800 BC to AD 1800. Cambridge, Eng.: Cambridge University Press. ISBN 978-0-521-47564-8.
- Cooter R, Pickstone JV, eds. (2003). Companion to Medicine in the 20th Century. Taylor & Francis. 756 pp. ISBN 978-0415286039.
- Donahue, M. Patricia. Nursing, The Finest Art: An Illustrated History (3r ed. 2010) excerpt and text search
- Jackson M, ed. (2011). The Oxford Handbook of the History of Medicine. Oxford University Press. 672 pp. ISBN 978-0-19-954649-7.
- Kessel G (2019). "Syriac Medicine". The Syriac World. London: Routledge. pp. 438–59. ISBN 978-1-138-89901-8.
- Loudon I, ed. (1997). Western Medicine: An Illustrated History. Oxford: Oxford University Press. ISBN 978-0-19-924813-1.
- Majno G (1991). The Healing Hand: Man and Wound in the Ancient World. Harvard University Press. ISBN 978-0674383319.
- McGrew RE, McGrew MP (1985). Encyclopedia of Medical History. New York: McGraw-Hill. ISBN 978-0-07-045087-5.
- Porter R (1997). The Greatest Benefit to Mankind: A Medical History of Humanity from Antiquity to the Present. Harper Collins. ISBN 978-0-393-31980-4.
- Nutton V (2012). Ancient Medicine (2nd ed.). London: Routledge. ISBN 978-0-415-52094-2.
- Porter R (1996). The Cambridge Illustrated History of Medicine. Cambridge: Cambridge University Press. ISBN 978-0-521-00252-3.
- Porter R (2006). The Cambridge History of Medicine (Rev. ed.). Cambridge: Cambridge University Press. ISBN 978-0-521-86426-8.
- Porter R (2004). Blood and Guts: A Short History of Medicine. WW Norton & Company. ISBN 978-0-393-32569-0.
- Rosenberg CE, ed. (1992). Framing Disease: Studies in Cultural History. Rutgers University Press. 326 pp. ISBN 978-0813517575.
- Rousseau GS, Gill M, Haycock D, Herwig M, eds. (2003). Framing and Imagining Disease in Cultural History. Basingstoke: Palgrave Macmillan. ISBN 978-1-4039-1292-3.
- Singer CJ, Underwood AE (2006). A Short History of Medicine (Rev. ed.). Cambridge: Cambridge University Press. ISBN 978-0-521-86426-8.
- Siraisi NG (September 2012). "Medicine, 1450-1620, and the history of science". Isis; an International Review Devoted to the History of Science and Its Cultural Influences. 103 (3): 491–514. doi:10.1086/667970. PMID 23286188. S2CID 6954963.
- Siraisi NG (1990). Medieval and Early Renaissance Medicine: An Introduction to Knowledge and Practice. Chicago: University of Chicago Press. ISBN 978-0-226-76130-5.
- Watts SJ (2003). Disease and Medicine in World History. Themes in World History. New York: Routledge. ISBN 978-0-415-27817-1.
- Wear A, ed. (1992). Medicine in Society: Historical Essays. Cambridge University Press. 397 pp. ISBN 978-0-521-33639-0.
- Weatherall M (1990). In Search of a Cure: A History of Pharmaceutical Discovery. Oxford: Oxford University Press. ISBN 978-0-19-261747-7.
External links
- The history of medicine and surgery as portrayed by various artists
- Directory of History of Medicine Collections, Index to the major collections in the United States and Canada, selected by the US National Institute of Health
 Texts on Wikisource:
Texts on Wikisource:
- Senfelder L (1911). "History of Medicine". Catholic Encyclopedia. Vol. 10.
Timeline of medicine and medical technology | ||
| Histories of basic sciences |
|  |
| Histories of medical specialties |
| |
| Medicine in ancient societies |
| |
| History of methods in medicine |
| |
| Disasters and plagues |
| |
| ||
History of biology | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fields, disciplines |
| ||||||||||||||||||||||||||
| Institutions |
| ||||||||||||||||||||||||||
| Theories, concepts |
| ||||||||||||||||||||||||||
| History |
| ||||||||||||||||||||||||||
| Related |
| ||||||||||||||||||||||||||
| |||||||||||||||||||||||||||
History of science | ||
|---|---|---|
| Background |
|  |
| By era |
| |
| By culture |
| |
| Natural sciences |
| |
| Mathematics |
| |
| Social sciences |
| |
| Technology |
| |
| Medicine |
| |
| ||