Endoscopic foreign body retrieval
Endoscopic foreign body retrieval refers to the removal of ingested objects from the esophagus, stomach and duodenum by endoscopic techniques. It does not involve surgery, but rather encompasses a variety of techniques employed through the gastroscope for grasping foreign bodies, manipulating them, and removing them while protecting the esophagus and trachea.[1] It is of particular importance with children,[2] people with mental illness,[3] and prison inmates[4] as these groups have a high rate of foreign body ingestion.
| Endoscopic foreign body retrieval | |
|---|---|
 | |
| Specialty | gastroenterology |
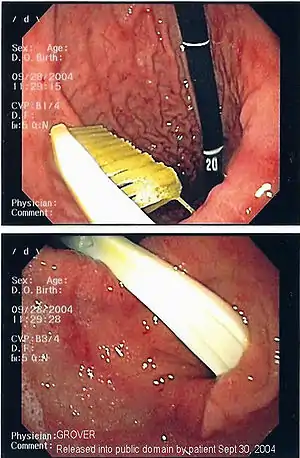
Commonly swallowed objects include coins, buttons, batteries, and small bones (such as fish bones),[1] but can include more complex objects, such as eyeglasses,[5] spoons,[6] and toothbrushes[5] (see image).
Indications and contraindications
Some patients at risk for foreign body ingestion may not be able to give an accurate medical history of ingestion, either due to age or mental illness. It is important that physicians treating these patients recognize the symptoms of esophageal foreign body impaction requiring urgent intervention. Most frequently, these include drooling and the inability to swallow saliva, neck tenderness, regurgitation of food, stridor and shortness of breath if there is compression of the trachea.[1][7]
There are several situations in which endoscopic techniques are not indicated, such as for small blunt objects less than 2.5 cm which have already passed into the stomach (as these usually do not obstruct anywhere else), when there is perforation of the esophagus or mediastinitis (inflammation of structures around the esophagus), and for narcotic-containing bags or condoms that have been ingested, because of the risk of overdose if they are ruptured.[1]
Foreign bodies should be removed from the esophagus within 24 hours of ingestion because of a high risk of complication.[8]
Non-invasive testing

Prior to undertaking endoscopy, attempts should be made to locate the foreign body with x-rays or other non-invasive techniques.[1] For radio-opaque objects, x-rays of the neck, chest and abdomen can be used to locate the foreign body and assist endoscopy.[9] Alternative approaches, including the use of metal detectors, have also been described.[10]
X-rays are also useful for identifying the type of foreign body ingested and complications of foreign body ingestion, including mediastinitis and perforation of the esophagus.[1]
Endoscopy
Endoscopic retrieval involves the use of a gastroscope or an optic fiber charge-coupled device camera. This instrument is shaped as a long tube, which is inserted through the mouth into the esophagus and stomach to identify the foreign body or bodies. This procedure is typically performed under conscious sedation. Many techniques have been described to remove foreign bodies from the stomach and esophagus. Usually the esophagus is protected with an overtube (a plastic tube of varying length), through which the gastroscope and retrieved objects are passed.[11]
Once the foreign body has been identified with the gastroscope, various devices can be passed through the gastroscope to grasp or manipulate the foreign body. Devices used include forceps, which come in varying shapes, sizes and grips,[12] snares, and oval loops that can be retracted from outside the gastroscope to lasso objects,[13] as well as Roth baskets (mesh nets that can be closed to trap small objects),[14] and magnets placed at the end of the scope or at the end of orogastric tubes.[12][15] Some techniques have been described that use foley catheters to trap objects, or use two snares to orient foreign bodies.[6]
Alternative methods
In veterinary medicine or when there is no endoscope available to extract foreign bodies economically without operation very often the Hartmann alligator forceps is used
See also
References
- Eisen, GM; Baron, TH; Dominitz, JA; Faigel, DO; Goldstein, JL; Johanson, JF; Mallery, JS; Raddawi, HM; et al. (2002). "Guideline for the management of ingested foreign bodies". Gastrointestinal Endoscopy. 55 (7): 802–6. doi:10.1016/S0016-5107(02)70407-0. PMID 12024131.
- Kay, M; Wyllie, R (2005). "Pediatric foreign bodies and their management". Current Gastroenterology Reports. 7 (3): 212–8. doi:10.1007/s11894-005-0037-6. PMID 15913481.
- Webb, WA (1995). "Management of foreign bodies of the upper gastrointestinal tract: update". Gastrointestinal Endoscopy. 41 (1): 39–51. doi:10.1016/S0016-5107(95)70274-1. PMID 7698623.
- O'Sullivan, S. T.; Reardon, C. M.; McGreal, G. T.; Hehir, D. J.; Kirwan, W. O.; Brady, M. P. (1996). "Deliberate ingestion of foreign bodies by institutionalised psychiatric hospital patients and prison inmates". Irish Journal of Medical Science. 165 (4): 294–6. doi:10.1007/BF02943095. PMID 8990660.
- Grover SC, Kim YI, Kortan PP, Marcon NE. Endoscopic removal of eight gastric foreign bodies ingested sequentially in twelve days: a case of creative endoscopy. Abstract presented at World Congress of Gastroenterology, Montreal, Canada, September 2005.
- Aoyagi, K; Maeda, K; Morita, I; Eguchi, K; Nishimura, H; Sakisaka, S (2003). "Endoscopic removal of a spoon from the stomach with a double-snare and balloon". Gastrointestinal Endoscopy. 57 (7): 990–1. doi:10.1016/S0016-5107(03)70044-3. PMID 12776067.
- Nandi, P; Ong, GB (1978). "Foreign body in the oesophagus: review of 2394 cases". The British Journal of Surgery. 65 (1): 5–9. doi:10.1002/bjs.1800650103. PMID 623968.
- Chaikhouni, A; Kratz, JM; Crawford, FA (1985). "Foreign bodies of the esophagus". The American Surgeon. 51 (4): 173–9. PMID 3985482.
- Lane, JE; Boltri, JM (2005). "Imaging gastric pennies in children". Emergency Radiology. 11 (3): 180–2. doi:10.1007/s10140-004-0372-1. PMID 16028326.
- Ramlakhan, SL; Burke, DP; Gilchrist, J (2006). "Things that go beep: experience with an ED guideline for use of a handheld metal detector in the management of ingested non‐hazardous metallic foreign bodies". Emergency Medicine Journal. 23 (6): 456–60. doi:10.1136/emj.2005.029553. PMC 2564343. PMID 16714508.
- Smith, M. T.; Wong, R. K. (2006). "Esophageal foreign bodies: Types and techniques for removal". Current Treatment Options in Gastroenterology. 9 (1): 75–84. doi:10.1007/s11938-006-0026-3. PMID 16423316.
- Seo, JK (1999). "Endoscopic management of gastrointestinal foreign bodies in children". Indian Journal of Pediatrics. 66 (1 Suppl): S75–80. PMID 11132474.
- Chen, SC; Yu, SC; Yuan, RH; Chang, KJ (1997). "Endoscopic removal of a large gastric metallic watch with a polypectomy snare loop". Endoscopy. 29 (9): S55–6. doi:10.1055/s-2007-1004333. PMID 9476781.
- Neustater, B; Barkin, JS (1996). "Extraction of an esophageal food impaction with a Roth retrieval net". Gastrointestinal Endoscopy. 43 (1): 66–7. doi:10.1016/s0016-5107(96)70265-1. PMID 8903823.
- Yamauchi, K; Kobayashi, T; Shinomiya, T; Fujiwara, D; Ito, W; Onoda, T; Yozai, K; Ishii, T; et al. (2001). "Device for the removal of button batteries". Internal Medicine (Tokyo, Japan). 40 (1): 9–13. doi:10.2169/internalmedicine.40.9. PMID 11201377.
External links
- Esophageal Coin MedPix Topic