Health in Japan
The level of health in Japan is due to a number of factors including cultural habits, isolation, and a universal health care system. John Creighton Campbell, a professor at the University of Michigan and Tokyo University, told the New York Times in 2009 that Japanese people are the healthiest group on the planet.[1] Japanese visit a doctor nearly 14 times a year, more than four times as often as Americans. Life expectancy in 2013 was 83.3 years - among the highest on the planet. [2]
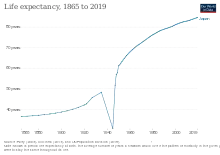
A new measure of expected human capital calculated for 195 countries from 1990 to 2016 and defined for each birth cohort as the expected years lived from age 20 to 64 years and adjusted for educational attainment, learning or education quality, and functional health status was published by the Lancet in September 2018. Japan had the highest level of expected human capital among the 20 largest countries: 24.1 health, education, and learning-adjusted expected years lived between age 20 and 64 years. [3]
Chronic illness
Obesity in Japan in 2014 was about 3.3%, about 10% of that in the United States, presumably because of the Japanese diet. It has the lowest rate of heart disease in the OECD, and the lowest level of dementia in the developed world.[4]
Suicide problem
Japan's suicide rate is high compared to the U.S. According to the systematic review Law in Everyday Japan : Sex, Sumo, Suicide, and Statutes, suicide rates have been at an elevated rate in Japan for 12 decades. In 1998, the suicide rate became more alarming as it increased, and it did not notably decrease until 2011.[5] The Yomiuri Shimbun reported in June 2008 that more than 30,000 people had killed themselves every year for the past decade, and the suicide count remained over 30,000 for the 14th year running in 2011. A study published in 2006 suspects that health problems were a factor in almost 50 percent of Japan's suicides in 2006. However, the Yomiuri's 2007 figures show 274 school children were among those who took their own lives, in which bullying was often a contributing factor. [6]
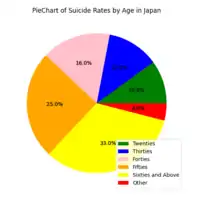
There are many factors to consider, but suicide rates overall appear to increase with age, as seen in the figure in this section.
As of 2003, suicides of people in their twenties made up about ten percent, those in their thirties made up about twelve percent, those in their forties made up about sixteen percent, those in their fifties made up about twenty-five percent, and those in their sixties or older made up about thirty-three percent.
Although suicide is a priority health issue, Japanese culture views the act as something different than morally wrong and unacceptable. In fact, according to Young's 2002 article, traditional Japanese culture accepts suicide as a positive moral act characterizing the person's sense of moral duty to others which is driven by social context.[7] Given that Japan is a collectivistic culture, moral duty to other members of society is important. Each individual is viewed as a part of the bigger group; everyone is considered a member of the group rather than as separated individuals. When a member feels that sacrificing their self would be best for the group as a whole, they are compelled to consider suicide as a viable option - they may believe that self-sacrifice is moral duty to the group. This is likely a part of the problem in trying to reduce the suicide rate. There is difficulty for psychiatrists and other mental health professionals in Japan to reduce the suicide rate when the act of suicide is, given the right circumstances, a completely rational and moral decision.
Smoking
_-_Korinsai.jpg.webp)
One of the biggest public health issues is smoking in Japan, which according to Tadao Kakizoe (honorary president of the National Cancer Center) kills more than 100,000 people per year and is responsible for one in ten deaths.[6]
Alcohol and health issues
A team led by Professor Osaki of Tottori University estimated the social cost of excessive drinking in Japan to be 4.15 trillion yen a year.[8]
Access to care
In Japan, services are provided either through regional/national public hospitals or through private hospitals/clinics, and patients have universal access to any facility, though hospitals tend to charge higher for those without a referral. However, space can be an issue in some regions. More than 14,000 emergency patients were rejected at least three times by Japanese hospitals before getting treatment in 2007, according to the latest government survey. In the worst case, a woman in her 70s with a breathing problem was rejected 49 times in Tokyo.[9] Public health insurance covers most citizens/residents and pays 70% or more cost for each care and each prescribed drug. Patients are responsible for the remainder (upper limits apply). The monthly insurance premium is 0–50,000 JPY per household (scaled to annual income). Supplementary private health insurance is available only to cover the co-payments or non-covered costs, and usually makes a fixed payment per days in a hospital or per surgery performed, rather than per actual expenditure. In 2005, Japan spent 8.2% of GDP on health care or US$2,908 per capita.[10] Of that, approximately 83% was government expenditure.
Cultural influences
Traditional Chinese medicine was introduced to Japan with other elements of Chinese culture during the 5th to 9th century. Since around 1900, Chinese-style herbalists have been required to be licensed medical doctors. Training was professionalized and, except for East Asian healers, was based on a biomedical model of the disease. However, the practice of biomedicine was influenced as well by Japanese social organization and cultural expectations concerning education, the organization of the workplace, and social relations of status and dependency, decision-making styles, and ideas about the human body, causes of illness, gender, individualism, and privacy. Anthropologist Emiko Ohnuki-Tierney notes that "daily hygienic behavior and its underlying concepts, which are perceived and expressed in terms of biomedical germ theory, in fact, are directly tied to the basic Japanese symbolic structure."
Western medicine was introduced to Japan with the Rangaku studies during the Edo period. A number of books on pharmacology and anatomy were translated from Dutch and Latin to Japanese. During the Meiji period (late 19th century), the Japanese health care system was modeled after the model of Western biomedicine. At that time, western doctors came to Japan to create medical faculties at the newly built Japanese universities, and students also went abroad. Innovations like vaccines were introduced to Japan, improving average life expectancy. From the Meiji period through the end of World War II, German was a mandatory foreign language for Japanese students of medicine. Patient charts in Japanese teaching hospitals were even written in German.
But even today, a person who becomes ill in Japan has a number of alternative options. One may visit a priest, or send a family member in his or her place. There are numerous folk remedies, including hot springs baths (onsen) and chemical and herbal over-the-counter medications. A person may seek the assistance of traditional healers, such as herbalists, masseurs, and acupuncturists.
AIDS
Although the number of AIDS cases remained small by international standards, public health officials were concerned in the late 1980s about the worldwide epidemic of acquired immune deficiency syndrome (AIDS). The first confirmed case of AIDS in Japan was reported in 1985. By 1991 there were 553 reported cases, and by April 1992 the number had risen to 2,077. While frightened by the deadliness of the disease yet sympathetic to the plight of hemophiliac AIDS patients, most Japanese are unconcerned with contracting AIDS themselves. Various levels of government responded to the introduction of AIDS awareness into the heterosexual population by establishing government committees, mandating AIDS education, and advising testing for the general public without targeting special groups. A fund, underwritten by pharmaceutical companies that distributed imported blood products, was established in 1988 to provide financial compensation for AIDS patients.
Environment and disease
See also
- 2009 flu pandemic in Japan
- Aging of Japan
- Erwin Bälz—an oyatoi gaikokujin and cofounder of modern medicine in Japan
- Health care compared—tabular comparisons with the U.S., Canada, and other countries not shown above.
- Health care system in Japan
- Hikikomori
- Public health centres in Japan
- Radiation effects from Fukushima Daiichi nuclear disaster
- Social welfare in Japan
References
- Arnquist, Sarah (25 August 2009). "Health Care Abroad: Japan". The New York Times.
- Britnell, Mark (2015). In Search of the Perfect Health System. London: Palgrave. p. 5. ISBN 978-1-137-49661-4.
- Lim, Stephen; et, al. "Measuring human capital: a systematic analysis of 195 countries and territories, 1990–2016". Lancet. Retrieved 5 November 2018.
- Britnell, Mark (2015). In Search of the Perfect Health System. London: Palgrave. p. 18. ISBN 978-1-137-49661-4.
- West, M. D. (2005). Law in everyday Japan. [electronic resource] : sex, sumo, suicide, and statutes. University of Chicago Press.
- Yomiuri Shimbun, 8/9/2008(?). Cited in Scott, Doug. "Japanese Delegation Visits AAPA to Learn about PA Profession" Archived 2010-12-03 at the Wayback Machine. AAPA News, July 15, 2008, p. 5. Accessed 2 December 2009.
- Young, J. (2002), Morals, Suicide, and Psychiatry: A View from Japan. Bioethics, 16: 412-424. https://doi.org/10.1111/1467-8519.00299
- "The Japan News - Breaking News from Japan by The Yomiuri Shimbun". Yomiuri.co.jp. Retrieved 2013-10-14.
- Yamaguchi, Mari. "Injured Man Dies After Rejection by 14 Hospitals". ABC News (Associated Press), February 4, 2009. Accessed 2 December 2009.
- "Japan Healthcare Spending 2000-2022". www.macrotrends.net. Retrieved 2022-03-04.
Further reading
- Campbell, John Creighton; Naoki Ikegami (1998). The Art of Balance in Health Policy: Maintaining Japan's Low-Cost, Egalitarian System. New York: Cambridge University Press. ISBN 0-521-57122-7. OCLC 486082265.
- "Law concerning Health and Medical Services for the Aged". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 881. ISBN 978-4-06-931098-0. OCLC 27812414.
- "Livelihood Protection Law". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 897. ISBN 978-4-06-931098-0. OCLC 27812414.
- "medical and health insurance". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 941. ISBN 978-4-06-931098-0. OCLC 27812414.
- "medical expenses". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 941. ISBN 978-4-06-931098-0. OCLC 27812414.
- "medicine". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. pp. 941–3. ISBN 978-4-06-931098-0. OCLC 27812414.
- "medicine, traditional". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 943. ISBN 978-4-06-931098-0.
- "National Health Insurance". Japan: An Illustrated Encyclopedia. Tokyo: Kodansha Ltd. 1993. p. 1058. ISBN 978-4-06-931098-0.
- Reid, T. R. (2009). The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care. New York: Penguin Press. ISBN 978-1-59420-234-6. OCLC 314597097. See in particular Chapter 6 "Japan: Bismark on Rice", pp. 82–124; this book is a further expansion of Reid's 2008 stories.
Health in Asia | |
|---|---|
| Sovereign states |
|
| States with limited recognition |
|
| Dependencies and other territories |
|
| |