Marcus Gunn phenomenon
Marcus Gunn phenomenon is an autosomal dominant condition with incomplete penetrance, in which nursing infants will have rhythmic upward jerking of their upper eyelid. This condition is characterized as a synkinesis: when two or more muscles that are independently innervated have either simultaneous or coordinated movements.[1][2]
| Marcus Gunn phenomenon | |
|---|---|
| Other names | Marcus Gunn jaw-winking or Trigemino-oculomotor synkinesis |
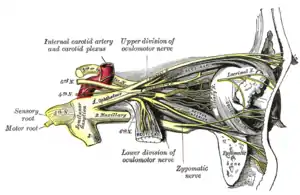 | |
| Nerves of the orbit, and the ciliary ganglion. Side view. (Trigeminal nerve and oculomotor nerve both visible) | |
| Specialty | Ophthalmology neurology |
Common physiologic examples of synkineses occur during sucking, chewing, or conjugate eye movements. There are also several abnormal cranial nerve synkineses, both acquired and congenital. Marcus Gunn jaw-winking is an example of a pathologic congenital synkinesis.
First described by the ophthalmologist Marcus Gunn in 1883,[3] this condition presents in approximately 5% of neonates with congenital ptosis. This condition has been associated with amblyopia (in 54% of cases), anisometropia (26%), and strabismus (56%).
Presentation

Behavioral and social implications
Although treatment may be unnecessary, there may be social implications, especially in young children when venturing from a supportive home environment to a public environment (e.g., starting school). Continued support, including monitoring behavior and educating the child about his or her appearance as seen by others, is encouraged. Gradual or sudden withdrawal from interaction with others is a sign that may or may not be related to such behavior. Studies are being conducted to elucidate these implications.
Pathophysiology
It has been postulated that the synkinesis is due to damage to cranial nerve nuclei, caused by peripheral nerve injury and the nuclear lesion releases evolutionarily older [neural] mechanisms with their tendency toward associated movements, and so primitive reflexes are not inhibited.
Marcus Gunn jaw-winking is an exaggeration of a very weak physiologic co-contraction that has been disinhibited secondary to a congenital brain stem lesion. The stimulation of the trigeminal nerve by contraction of the pterygoid muscles of jaw results in the excitation of the branch of the oculomotor nerve that innervates the levator palpebrae superioris ipsilaterally (on the same side of the face), so the patient will have rhythmic upward jerking of their upper eyelid.
There are two major groups of trigemino-oculomotor synkineses:
1) External pterygoid-levator synkinesis is when the eyelid raises upon:
- Jaw thrust to opposite side (homolateral external pterygoid)
- Jaw is projected forward (bilateral external pterygoid)
- Mouth is opened widely
2) Internal pterygoid-levator synkinesis is when the eyelid raises upon teeth clenching
External pterygoid-levator synkinesis is the more common group.
Treatment
Treatment is usually unnecessary. In severe cases, surgery with a bilateral levator excision and frontalis brow suspension may be used.[4]
Inverse Marcus Gunn phenomenon
Inverse Marcus Gunn phenomenon is a rare condition[5] that causes the eyelid to fall upon opening of the mouth. In this case, trigeminal innervation to the pterygoid muscles of the jaw is associated with an inhibition of the branch of the oculomotor nerve to the levator palpebrae superioris, as opposed to stimulation in Marcus Gunn jaw-winking.
References
- Yamada K, Hunter DG, Andrews C, Engle EC (September 2005). "A novel KIF21A mutation in a patient with congenital fibrosis of the extraocular muscles and Marcus Gunn jaw-winking phenomenon". Arch. Ophthalmol. 123 (9): 1254–9. doi:10.1001/archopht.123.9.1254. PMID 16157808.
- Cates CA, Tyers AG (2008). "Results of levator excision followed by fascia lata brow suspension in patients with congenital and jaw-winking ptosis". Orbit. 27 (2): 83–9. doi:10.1080/01676830701376072. PMID 18415867. S2CID 23268883.
- Gunn RM. Congenital ptosis with peculiar associated movements of the affected lid. Trans Ophthal Soc UK. 1883;3:283-7.
- Ibrahim HA (2007). "Use of the levator muscle as a frontalis sling". Ophthal Plast Reconstr Surg. 23 (5): 376–80. doi:10.1097/IOP.0b013e3181379e20. PMID 17881988. S2CID 13655363.
- Prakash MV, Radhakrishnan M, Yogeshwari A, Nazir W, Maragatham K, Natarajan K (June 2002). "Inverse Marcus Gunn phenomenon". Indian J Ophthalmol. 50 (2): 142–4. PMID 12194575.