Musculocutaneous nerve
The musculocutaneous nerve arises from the lateral cord of the brachial plexus, opposite the lower border of the pectoralis major, its fibers being derived from C5, C6 and C7.
| Musculocutaneous nerve | |
|---|---|
 Nerves of the left upper extremity. (Musculocutaneous labeled at upper right.) | |
| Details | |
| From | lateral cord (C5-C7) |
| To | lateral cutaneous nerve of forearm |
| Innervates | anterior compartment of the arm |
| Identifiers | |
| Latin | nervus musculocutaneus |
| MeSH | D009138 |
| TA98 | A14.2.03.024 |
| TA2 | 6421 |
| FMA | 37064 |
| Anatomical terms of neuroanatomy | |
Structure
The musculocutaneous nerve arises from the lateral cord of the brachial plexus, courses through the anterior part of the arm, and terminates at 2 cm above elbow as the lateral cutaneous nerve of the forearm.
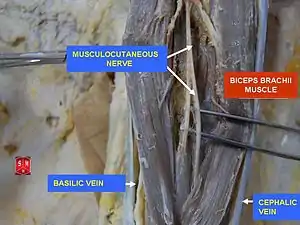
Musculocutaneous nerve arises from the lateral cord of the brachial plexus with root value of C5 to C7 of the spinal cord. It follows the course of the third part of the axillary artery (part of the axillary artery distal to the pectoralis minor) laterally and enters the frontal aspect of the arm where it penetrates the coracobrachialis muscle. It then passes downwards and laterally between the biceps brachii (above) and the brachialis muscles (below), to the lateral side of the arm; at 2 cm above the elbow it pierces the deep fascia lateral to the tendon of the biceps brachii and is continued into the forearm as the lateral cutaneous nerve of the forearm.[1]
In its course through the arm it innervates the coracobrachialis, biceps brachii, and the greater part of the brachialis. Its terminal branch, the lateral cutaneous nerve of the forearm, supplies the sensation of the lateral side of the forearm from the elbow to the wrist. Besides, the musculocutaneous nerve also gives articular branches to the elbow joint and to the humerus.[1]
Variations
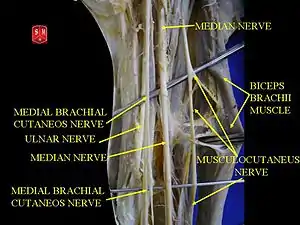
The musculocutaneous nerve presents frequent variations and communications with the median nerve.[2][3]
- It may adhere for some distance to the median and then pass outward, beneath the biceps brachii, instead of through the coracobrachialis.
- Some of the fibers of the median may run for some distance in the musculocutaneous and then leave it to join their proper trunk; less frequently the reverse is the case, and the median sends a branch to join the musculocutaneous.[4]
- The nerve may pass under the coracobrachialis or through the biceps brachii.
- Occasionally it gives a filament to the pronator teres, and it supplies the dorsal surface of the thumb when the superficial branch of the radial nerve is absent.
Nerve injuries
Injury to the musculocutaneous nerve can be caused by three mechanisms: repeated microtrauma, indirect trauma or direct trauma on the nerve. Overuse of coracobrachialis, biceps, and brachialis muscles can cause the stretching or compression of musculocutaneous nerve. Those who have it can complain of pain, tingling or reduced sensation over the lateral side of the forearm. This symptom can be reproduced by pressing over the region below the coracoid process (positive Tinel's sign). Pain can also be reproduced by flexing the arm against resistance. Other differential diagnoses that can mimick the symptoms of musculocutaneous palsy are: C6 radiculopathy (pain can be produced by movement of the neck), long head of biceps tendinopathy (no motor or sensory deficits), pain of the bicipital groove (relieved by shoulder joint injection). Electromyography test shows slight neural damage at the biceps and the brachialis muscles with slower motor and sensory conduction over the Erb's point.[5]
In indirect trauma, violent abduction and retroposition of the shoulder can stretch the nerve and result tension of the coracobrachialis with musculocutaneous nerve lesion. Those with this type of lesion is presented with pain, reduced sensation, and tingling of the lateral part of forearm (lateral antebrachial cutaneous nerve - terminal sensory only branch of Musculocutaneous nerve) with reduced strength of elbow flexion. Tinel's sign can be positive. Differential diagnosis includes C5 and C6 nerve root lesions of the brachial plexus where the abduction, external rotation, and elbow flexion is lost. On the other hand, rupture of the biceps can cause the loss of flexion of the elbow without sensory deficits. Rupture of the SHORT HEAD of the biceps can decrease elbow flexion strength, where the brachialis muscle is intact. Rupture of the LONG HEAD of the biceps results in mild weakening of forearm supination as long as the supinator muscle is intact. Electromyography test is negative.[5]
In direct trauma, fracture of the humerus, gun shot, glass pieces injuries and more, can cause the musculocutaneous nerve lesion.[5]
Iatrogenic nerve injuries (for example during orthopedic surgery involving an internal fixation of the humerus) are relatively common and in a certain percentage of cases probably inevitable, though an adequate knowledge of the surgical anatomy can help to reduce its frequency.[6]
Neurolysis and nerve grafting are the treatment options for the above lesions.[5]
References
![]() This article incorporates text in the public domain from page 935 of the 20th edition of Gray's Anatomy (1918)
This article incorporates text in the public domain from page 935 of the 20th edition of Gray's Anatomy (1918)
- Krishna, Garg (2010). "8 - Arm". BD Chaurasia's Human Anatomy (Regional and Applied Dissection and Clinical) Volume 1 - Upper limb and thorax (Fifth ed.). India: CBS Publishers and Distributors Pvt Ltd. p. 88. ISBN 978-81-239-1863-1.
- Choi D, Rodríguez-Niedenführ M, Vázquez T, Parkin I, Sañudo JR (January 2002). "Patterns of connections between the musculocutaneous and median nerves in the axilla and arm". Clin Anat. 15 (1): 11–7. doi:10.1002/ca.1085. PMID 11835538. S2CID 23969081.
- Guerri-Guttenberg RA, Ingolotti M (September 2009). "Classifying musculocutaneous nerve variations". Clin Anat. 22 (6): 671–83. doi:10.1002/ca.20828. PMID 19637305. S2CID 2457543.
- Guerri-Guttenberg, Roberto A.; Ingolotti, Mariana (2009). "Classifying musculocutaneous nerve variations". Clinical Anatomy. 22 (6): 671–83. doi:10.1002/ca.20828. PMID 19637305. S2CID 2457543.
- Celli, Andrea; Celli, Luigi; F Morrey, Bernard (25 January 2008). "28 - Traumatic isolated lesions of musculocutaneous nerve". Treatment of Elbow Lesions: New Aspects in Diagnosis and Surgical Techniques. Springer. pp. 299–302. ISBN 9788847005914. Retrieved 26 January 2018.
- Zhang J, Moore AE, Stringer MD (April 2011). "Iatrogenic upper limb nerve injuries: a systematic review". ANZ Journal of Surgery. 81 (4): 227–36. doi:10.1111/j.1445-2197.2010.05597.x. PMID 21418465. S2CID 25443502.
External links
- Musculocutaneous nerve at the Duke University Health System's Orthopedics program
- Hand kinesiology at the University of Kansas Medical Center