Healthcare reform in the United States
Healthcare reform in the United States has a long history. Reforms have often been proposed but have rarely been accomplished. In 2010, landmark reform was passed through two federal statutes enacted in 2010: the Patient Protection and Affordable Care Act (PPACA), signed March 23, 2010,[1][2] and the Health Care and Education Reconciliation Act of 2010 (H.R. 4872), which amended the PPACA and became law on March 30, 2010.[3][4]
| This article is part of a series on |
| Healthcare reform in the United States |
|---|
 |
|
|
Future reforms of the American health care system continue to be proposed, with notable proposals including a single-payer system and a reduction in fee-for-service medical care.[5] The PPACA includes a new agency, the Center for Medicare and Medicaid Innovation (CMS Innovation Center), which is intended to research reform ideas through pilot projects.
History of national reform efforts
The following is a summary of reform achievements at the national level in the United States. For failed efforts, state-based efforts, native tribes services, and more details, see the history of health care reform in the United States article.
- 1965 President Lyndon Johnson enacted legislation that introduced Medicare, covering both hospital (Part A) and supplemental medical (Part B) insurance for senior citizens. The legislation also introduced Medicaid, which permitted the Federal government to partially fund a program for the poor, with the program managed and co-financed by the individual states.[6][7]
- 1985 The Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) amended the Employee Retirement Income Security Act of 1974 (ERISA) to give some employees the ability to continue health insurance coverage after leaving employment.[8]
- 1996 The Health Insurance Portability and Accountability Act (HIPAA) not only protects health insurance coverage for workers and their families when they change or lose their jobs, it also made health insurance companies cover pre-existing conditions. If such condition had been diagnosed before purchasing insurance, insurance companies are required to cover it after patient has one year of continuous coverage. If such condition was already covered on their current policy, new insurance policies due to changing jobs, etc... have to cover the condition immediately.[9]
- 1997 The Balanced Budget Act of 1997 introduced two new major Federal healthcare insurance programs, Part C of Medicare and the State Children's Health Insurance Program, or SCHIP. Part C formalized longstanding "Managed Medicare" (HMO, etc.) demonstration projects and SCHIP was established to provide health insurance to children in families at or below 200 percent of the federal poverty line. Many other "entitlement" changes and additions were made to Parts A and B of fee for service (FFS) Medicare and to Medicaid within an omnibus law that also made changes to the Food Stamp and other Federal programs.[10]
- 2000 The Medicare, Medicaid, and SCHIP Benefits Improvement and Protection Act (BIPA) effectively reversed some of the cuts to the three named programs in the Balanced Budget Act of 1997 because of Congressional concern that providers would stop providing services.
- 2003 The Medicare Prescription Drug, Improvement, and Modernization Act (also known as the Medicare Modernization Act or MMA) introduced supplementary optional coverage within Medicare for self-administered prescription drugs and as the name suggests also changed the other three existing Parts of Medicare law.
- 2010 The Patient Protection and Affordable Care Act, called PPACA or ACA but also known as Obamacare, was enacted, including the following provisions:[3]
- the phased introduction over multiple years of a comprehensive system of mandated health insurance reforms designed to eliminate "some of the worst practices of the insurance companies"—pre-existing condition screening and premium loadings, policy cancellations on technicalities when illness seems imminent, annual and lifetime coverage caps
- Expanded Medicaid to cover uninsured working-age adults (18-65) earning under 138% of the Federal Poverty Line (and therefore not eligible for subsidies on the health insurance marketplace) along with some whose existing insurance plans were too expensive based on their income. The ACA expanded Medicaid eligibility in all 50 states and the District of Columbia, however that provision was successfully challenged in NFIB v. Sebelius where the U.S. Supreme Court ruled that individual states could chose whether or not to expand coverage. Initially 25 states and D.C. expanded Medicaid with funding from the federal government provided by the ACA beginning in 2014, and as of 2022 there are 38 states that have expanded coverage.
- created health insurance marketplaces with three standard insurance coverage levels to enable like-for-like comparisons by consumers, and a web-based health insurance exchange where consumers can compare prices and purchase plans.
- mandates that insurers fully cover certain preventative services
- created high-risk pools for uninsureds
- tax credits for businesses to provide insurance to employees
- created an insurance company rate review program
- allowed dependents to remain on their plan until 26
- It also sets a minimum medical loss ratio of direct health care spending to premium income creates price competition
- created Patient-Centered Outcomes Research Institute to study comparative effectiveness research funded by a fee on insurers per covered life
- allowed for approval of generic biologic drugs and specifically allows for 12 years of exclusive use for newly developed biologic drugs
- many changes to the 1997, 2000, and 2003 laws that had previously changed Medicare and further expanded eligibility for Medicaid (that expansion was later ruled by the Supreme Court to be at the discretion of the states)
- explores some programs intended to increase incentives to provide quality and collaborative care, such as accountable care organizations. The Center for Medicare and Medicaid Innovation was created to fund pilot programs which may reduce costs;[11] the experiments cover nearly every idea healthcare experts advocate, except malpractice/tort reform.[12]
- requires for reduced Medicare reimbursements for hospitals with excess readmissions and eventually ties physician Medicare reimbursements to quality of care metrics.
- 2015 The Medicare Access and CHIP Reauthorization Act (MACRA) made significant changes to the process by which many Medicare Part B services are reimbursed and also extended SCHIP
- 2017 Donald Trump is sworn in as President, signs Executive Order 13765 in anticipation of a repeal of the Patient Protection and Affordable Care Act, one of his campaign promises. The American Health Care Act is introduced and passed in the House of Representatives and introduced but not voted upon in the Senate. President Donald Trump signs Executive Order 13813 which allows insurance companies to sell low-cost short-term plans with lesser coverage, enables small business to collectively purchase association health plans, and expands health savings accounts.
Motivation

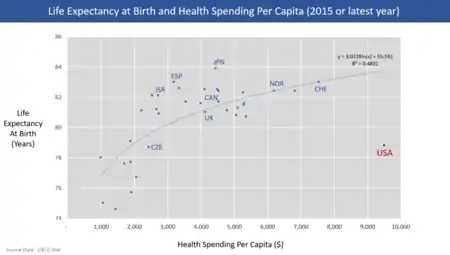
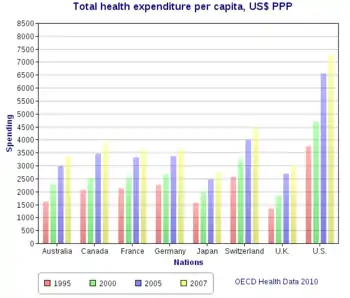
International comparisons of healthcare have found that the United States spends more per-capita than other similarly developed nations but falls below similar countries in various health metrics, suggesting inefficiency and waste. In addition, the United States has significant underinsurance and significant impending unfunded liabilities from its aging demographic and its social insurance programs Medicare and Medicaid (Medicaid provides free long-term care to the elderly poor). The fiscal and human impact of these issues have motivated reform proposals.
U.S. healthcare costs were approximately $3.2 trillion or nearly $10,000 per person on average in 2015. Major categories of expense include hospital care (32%), physician and clinical services (20%), and prescription drugs (10%).[14] U.S. costs in 2016 were substantially higher than other OECD countries, at 17.2% GDP versus 12.4% GDP for the next most expensive country (Switzerland).[15] For scale, a 5% GDP difference represents about $1 trillion or $3,000 per person. Some of the many reasons cited for the cost differential with other countries include: Higher administrative costs of a private system with multiple payment processes; higher costs for the same products and services; more expensive volume/mix of services with higher usage of more expensive specialists; aggressive treatment of very sick elderly versus palliative care; less use of government intervention in pricing; and higher income levels driving greater demand for healthcare.[16][17][18] Healthcare costs are a fundamental driver of health insurance costs, which leads to coverage affordability challenges for millions of families. There is ongoing debate whether the current law (ACA/Obamacare) and the Republican alternatives (AHCA and BCRA) do enough to address the cost challenge.[19]
According to 2009 World Bank statistics, the U.S. had the highest health care costs relative to the size of the economy (GDP) in the world, even though estimated 50 million citizens (approximately 16% of the September 2011 estimated population of 312 million) lacked insurance.[20] In March 2010, billionaire Warren Buffett commented that the high costs paid by U.S. companies for their employees' health care put them at a competitive disadvantage.[21]

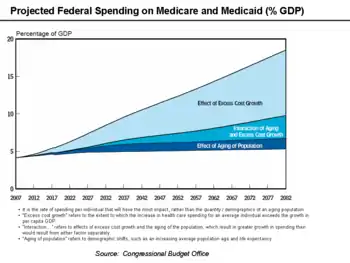
Further, an estimated 77 million Baby Boomers are reaching retirement age, which combined with significant annual increases in healthcare costs per person will place enormous budgetary strain on U.S. state and federal governments, particularly through Medicare and Medicaid spending (Medicaid provides long-term care for the elderly poor).[24] Maintaining the long-term fiscal health of the U.S. federal government is significantly dependent on healthcare costs being controlled.[25]
Insurance cost and availability
In addition, the number of employers who offer health insurance has declined and costs for employer-paid health insurance are rising: from 2001 to 2007, premiums for family coverage increased 78%, while wages rose 19% and prices rose 17%, according to the Kaiser Family Foundation.[26] Even for those who are employed, the private insurance in the US varies greatly in its coverage; one study by the Commonwealth Fund published in Health Affairs estimated that 16 million U.S. adults were underinsured in 2003. The underinsured were significantly more likely than those with adequate insurance to forgo health care, report financial stress because of medical bills, and experience coverage gaps for such items as prescription drugs. The study found that underinsurance disproportionately affects those with lower incomes—73% of the underinsured in the study population had annual incomes below 200% of the federal poverty level.[27] However, a study published by the Kaiser Family Foundation in 2008 found that the typical large employer preferred provider organization (PPO) plan in 2007 was more generous than either Medicare or the Federal Employees Health Benefits Program Standard Option.[28] One indicator of the consequences of Americans' inconsistent health care coverage is a study in Health Affairs that concluded that half of personal bankruptcies involved medical bills,[29] although other sources dispute this.[30]
There are health losses from insufficient health insurance. A 2009 Harvard study published in the American Journal of Public Health found more than 44,800 excess deaths annually in the United States due to Americans lacking health insurance.[31][32] More broadly, estimates of the total number of people in the United States, whether insured or uninsured, who die because of lack of medical care were estimated in a 1997 analysis to be nearly 100,000 per year.[33] A study of the effects of the Massachusetts universal health care law (which took effect in 2006) found a 3% drop in mortality among people 20–64 years old—1 death per 830 people with insurance. Other studies, just as those examining the randomized distribution of Medicaid insurance to low-income people in Oregon in 2008, found no change in death rate.[34]
The cost of insurance has been a primary motivation in the reform of the US healthcare system, and many different explanations have been proposed in the reasons for high insurance costs and how to remedy them. One critique and motivation for healthcare reform has been the development of the medical–industrial complex. This relates to moral arguments for health care reform, framing healthcare as a social good, one that is fundamentally immoral to deny to people based on economic status.[35] The motivation behind healthcare reform in response to the medical-industrial complex also stems from issues of social inequity, promotion of medicine over preventative care.[36] The medical-industrial complex, defined as a network of health insurance companies, pharmaceutical companies, and the like, plays a role in the complexity of the US insurance market and a fine line between government and industry within it.[37] Likewise, critiques of insurance markets being conducted under a capitalistic, free-market model also include that medical solutions, as opposed to preventative healthcare measures, are promoted to maintain this medical-industrial complex.[37] Arguments for a market-based approach to health insurance include the Grossman model, which is based on an ideal competitive model, but others have critiqued this, arguing that fundamentally, this means that people in higher socioeconomic levels will receive a better quality of healthcare.[36]
- Uninsured rate
With the implementation of the ACA, the level of uninsured rates severely decreased in the U.S. This is due to the expansion of qualifications for access to medicaid, subsidizing insurance, prevention of insurance companies from underwriting, as well as enforcing the individual mandate which requires citizens to purchase health insurance or pay a fee. In a research study which was conducted comparing the effects of the ACA before and after it was fully implemented in 2014, it was discovered that racial and ethnic minorities benefited more than whites with many gaining insurance coverage which they lacked before allowing for many to seek treatment improving their overall health.[38] In June 2014, Gallup–Healthways Well–Being conducted a survey and found that the uninsured rate is decreasing with 13 percent of U.S. adults uninsured in 2014 compared to 17 percent in January 2014 and translates to roughly 10 million to 11 million individuals who gained coverage. The survey also looked at the major demographic groups and found each is making progress towards getting health insurance. However, Hispanics, who have the highest uninsured rate of any racial or ethnic group, are lagging in their progress. Under the new health care reform, Latinos were expected to be major beneficiaries of the new health care law. Gallup found that the biggest drop in the uninsured rate (3 percentage points) was among households making less than $36,000 a year.[39][40][41]
Waste and fraud
In December 2011 the outgoing Administrator of the Centers for Medicare & Medicaid Services, Donald Berwick, asserted that 20% to 30% of health care spending is waste. He listed five causes for the waste: (1) overtreatment of patients, (2) the failure to coordinate care, (3) the administrative complexity of the health care system, (4) burdensome rules and (5) fraud.[42]
An estimated 3–10% of all health care expenditures in the U.S. are fraudulent. In 2011, Medicare and Medicaid made $65 billion in improper payments (including both error and fraud). Government efforts to reduce fraud include $4 billion in fraudulent payments recovered by the Department of Justice and the FBI in 2012, longer jail sentences specified by the Affordable Care Act, and Senior Medicare Patrols—volunteers trained to identify and report fraud.[43]
In 2007, the Department of Justice and Health and Human Services formed the Medicare Fraud Strike Force to combat fraud through data analysis and increased community policing. As of May 2013, the Strike Force has charged more than 1,500 people for false billings of more than $5 billion. Medicare fraud often takes the form of kickbacks and money-laundering. Fraud schemes often take the form of billing for medically unnecessary services or services not rendered.[44]
Quality of care
There is significant debate regarding the quality of the U.S. healthcare system relative to those of other countries. Although there are advancements in the quality of care in America due to the acknowledgement of various health related topics such as how insurance plans are now mandated to include coverage for those with mental health and substance abuse disorders as well with the inability to deny a person who has preexisting conditions through the ACA,[45] there is still much that needs to be improved. Within the U.S., those who are a racial/ethnic minority along with those who poses a lower income have higher chances of experiencing a lower quality of care at higher cost. Despite the advancements with the ACA, this may discourage a person from seeking medical treatment.[46] Physicians for a National Health Program, a pro-universal single-payer system of health care advocacy group, has claimed that a free market solution to health care provides a lower quality of care, with higher mortality rates, than publicly funded systems.[47] The quality of health maintenance organizations and managed care have also been criticized by this same group.[48]
According to a 2000 study of the World Health Organization, publicly funded systems of industrial nations spend less on health care, both as a percentage of their GDP and per capita, and enjoy superior population-based health care outcomes.[49] However, conservative commentator David Gratzer and the Cato Institute, a libertarian think tank, have both criticized the WHO's comparison method for being biased; the WHO study marked down countries for having private or fee-paying health treatment and rated countries by comparison to their expected health care performance, rather than objectively comparing quality of care.[50][51]
Some medical researchers say that patient satisfaction surveys are a poor way to evaluate medical care. Researchers at the RAND Corporation and the Department of Veterans Affairs asked 236 elderly patients in two different managed care plans to rate their care, then examined care in medical records, as reported in Annals of Internal Medicine. There was no correlation. "Patient ratings of health care are easy to obtain and report, but do not accurately measure the technical quality of medical care," said John T. Chang, UCLA, lead author.[52][53][54]
Public opinion
Public opinion polls have shown a majority of the public supports various levels of government involvement in health care in the United States,[55] with stated preferences depending on how the question is asked.[56] Polls from Harvard University in 1988,[57] the Los Angeles Times in 1990,[58] and The Wall Street Journal in 1991[59] all showed strong support for a health care system compared to the system in Canada. More recently, however, polling support has declined for that sort of health care system,[55][56] with a 2007 Yahoo/AP poll showing 54% of respondents considered themselves supporters of "single-payer health care,"[60] a majority in favor of a number of reforms according to a joint poll with the Los Angeles Times and Bloomberg,[61] and a plurality of respondents in a 2009 poll for Time Magazine showed support for "a national single-payer plan similar to Medicare for all."[62] Polls by Rasmussen Reports in 2011[63] and 2012[64] showed pluralities opposed to single-payer health care. Many other polls show support for various levels of government involvement in health care, including polls from New York Times/CBS News[65][66] and Washington Post/ABC News,[67] showing favorability for a form of national health insurance. The Kaiser Family Foundation[68] showed 58% in favor of a national health plan such as Medicare-for-all in 2009, with support around the same level from 2017 to April 2019, when 56% said they supported it.[69][70] A Quinnipiac poll in three states in 2008 found majority support for the government ensuring "that everyone in the United States has adequate health-care" among likely Democratic primary voters.[71]
A 2001 article in the public health journal Health Affairs studied fifty years of American public opinion of various health care plans and concluded that, while there appears to be general support of a "national health care plan," poll respondents "remain satisfied with their current medical arrangements, do not trust the federal government to do what is right, and do not favor a single-payer type of national health plan."[55] Politifact rated a 2009 statement by Michael Moore "false" when he stated that "[t]he majority actually want single-payer health care." According to Politifact, responses on these polls largely depend on the wording. For example, people respond more favorably when they are asked if they want a system "like Medicare".[56]
.JPG.webp)
Alternatives and research directions
There are alternatives to the exchange-based market system which was enacted by the Patient Protection and Affordable Care Act which have been proposed in the past and continue to be proposed, such as a single-payer system and allowing health insurance to be regulated at the federal level.
In addition, the Patient Protection and Affordable Health Care Act of 2010 contained provisions which allows the Centers for Medicare and Medicaid Services (CMS) to undertake pilot projects which, if they are successful could be implemented in future.
Single-payer health care
A number of proposals have been made for a universal single-payer healthcare system in the United States, most recently the United States National Health Care Act, (popularly known as H.R. 676 or "Medicare for All") but none have achieved more political support than 20% congressional co-sponsorship. Advocates argue that preventative health care expenditures can save several hundreds of billions of dollars per year because publicly funded universal health care would benefit employers and consumers, that employers would benefit from a bigger pool of potential customers and that employers would likely pay less, and would be spared administrative costs of health care benefits. It is also argued that inequities between employers would be reduced.[72][73][74] Also, for example, cancer patients are more likely to be diagnosed at Stage I where curative treatment is typically a few outpatient visits, instead of at Stage III or later in an emergency room where treatment can involve years of hospitalization and is often terminal.[75][76] Others have estimated a long-term savings amounting to 40% of all national health expenditures due to preventative health care,[77] although estimates from the Congressional Budget Office and The New England Journal of Medicine have found that preventative care is more expensive.[78]
Any national system would be paid for in part through taxes replacing insurance premiums, but advocates also believe savings would be realized through preventative care and the elimination of insurance company overhead and hospital billing costs.[79] An analysis of a single-payer bill by the Physicians for a National Health Program estimated the immediate savings at $350 billion per year.[80] The Commonwealth Fund believes that, if the United States adopted a universal health care system, the mortality rate would improve and the country would save approximately $570 billion a year.[81]
Recent enactments of single-payer systems within individual states, such as in Vermont in 2011, may serve as living models supporting federal single-payer coverage, however in 2014 then Governor Peter Shumlin announced that his administration would not move forward with the creation of a single-payer system in the states.[82] [83][84]
On June 1, 2017, in light of the recent Trump Administration’s efforts to repeal the Affordable Care Act, California Democratic Senator Ricardo Lara proposed a bill to establish single-payer healthcare within the state of California (SB 562), calling on fellow senators to act quickly in defense of healthcare. The legislation would implement “Medicare for All,” placing all levels of healthcare in the hands of the state. The bill proposed to the California Senate by Senator Lara lacked a method of funding required to finance the $400 billion-dollar policy. Despite this lack of foresight, the bill gained approval from the senate and will move on to await approval by the state assembly.[85]
In wake of the Affordable Care Act, the state of California has experienced the greatest rise in newly insured people compared to other states. Subsequently, the number of physicians under MediCal are not enough to meet the demand, therefore 25% of physicians care for 80% of patients who are covered through MediCal[86]
In the past, California has struggled to maintain healthcare effectiveness, due in part to its unstable budget and complex regulations. The state has a policy in place known as the Gann Limit, otherwise entitled proposition 98, which ensures that a portion of state funds are directed towards the education system. This limit would be exceeded if California raises taxes to fund the new system which would require $100 billion in tax revenue. In order to avoid legal dispute, voters would be required to amend proposition 98 and exempt healthcare funding from required educational contributions.[87] The state announced on August 1, 2017 that coverage for health insurance will increase by 12.5% in next year, threatening the coverage of 1.5 million people [88]
Public option
In January 2013, Representative Jan Schakowsky and 44 other U.S. House of Representatives Democrats introduced H.R. 261, the "Public Option Deficit Reduction Act" which would amend the 2010 Affordable Care Act to create a public option. The bill would set up a government-run health insurance plan with premiums 5% to 7% percent lower than private insurance. The Congressional Budget Office estimated it would reduce the United States public debt by $104 billion over 10 years.[89]
Balancing doctor supply and demand
The Medicare Graduate Medical Education program regulates the supply of medical doctors in the U.S.[90] By adjusting the reimbursement rates to establish more income equality among the medical professions, the effective cost of medical care can be lowered.
Bundled payments
A key project is one that could radically change the way the medical profession is paid for services under Medicare and Medicaid. The current system, which is also the prime system used by medical insurers is known as fee-for-service because the medical practitioner is paid only for the performance of medical procedures which, it is argued means that doctors have a financial incentive to do more tests (which generates more income) which may not be in the patients' best long-term interest. The current system encourages medical interventions such as surgeries and prescribed medicines (all of which carry some risk for the patient but increase revenues for the medical care industry) and does not reward other activities such as encouraging behavioral changes such as modifying dietary habits and quitting smoking, or follow-ups regarding prescribed regimes which could have better outcomes for the patient at a lower cost. The current fee-for-service system also rewards bad hospitals for bad service. Some have noted that the best hospitals have fewer re-admission rates than others, which benefits patients, but some of the worst hospitals have high re-admission rates which is bad for patients but is perversely rewarded under the fee-for-service system.
Projects at CMS are examining the possibility of rewarding health care providers through a process known as "bundled payments"[91] by which local doctors and hospitals in an area would be paid not on a fee for service basis but on a capitation system linked to outcomes. The areas with the best outcomes would get more. This system, it is argued, makes medical practitioners much more concerned to focus on activities that deliver real health benefits at a lower cost to the system by removing the perversities inherent in the fee-for-service system.
Though aimed as a model for health care funded by CMS, if the project is successful it is thought that the model could be followed by the commercial health insurance industry also.
Centers for Medicare and Medicaid Innovation
With the ACA improving the health of many by increasing the number of people who are insured, this is not the final stage for the ACA due to the push for a medicaid expansion reform. With the Democrats supporting the expansion and the Republicans against it, it was denied in the Supreme Court in the trial of NFIB vs Sebelius. The Court ruled that implementing taxes in order to pay for health insurance for all citizens was an unconstitutional exercise of Congress’s power under Article I.[92] If the expansion eventually succeeds, Medicaid would become a fully federal program with new federal eligibility standards. This would alleviate the responsibility of state governments to fund Medicaid.[93]
In addition to the reform for the medicaid expansion, there are additional reforms focused on addressing social determinants in the healthcare system through various programs and initiatives in order to reduce healthcare expenditures and improve health outcomes.
Programs and initiatives recognizing and addressing non-medical social needs have sprung from various sectors within healthcare, with emerging efforts made by multi-payer federal and state initiatives, medicaid initiatives led by states, or by health plans, as well as provider level actions. State and federal initiatives, primarily sponsored CMMI (Center for Medicare and Medicaid Innovation) a division of CMS, seek to address basic social needs within the context of the healthcare delivery system. CMMI initiatives like the 2016 "Accountable Health Communities" (AHC) model have been created to focus on connecting Medicare and Medicaid beneficiaries with community services to address health-related social needs, while providing funds to organizations so that they can systematically identify and address the health-related social needs of Medicare and Medicaid recipients through screening, referral, and community navigation services.[94] The model was officially implemented in 2017 and will be evaluated for its ability to affect cost of healthcare spending and reduce inpatient/outpatient utilization in 2022.[94][95] Under the AHC model, funds have been allocated towards developing a 10-item screening tool to identify 5 different patient need domains that can be addressed through community resources (housing instability, food insecurity, transportation difficulties, utility assistance needs, and interpersonal safety).[96] Increasing bodies of evidence suggest that addressing social needs can help stop their damaging health effects, but screening for social needs is not yet standard clinical practice. Applying this tool in the AHC model will help CMS evaluate the impact of local partnerships between healthcare providers and community organizations in advancing the aims of addressing the cost and quality of health care across all settings.[96] National recommendations around multi-dimension screening for social risk are not yet available since the evidence base to support such recommendations is highly under-developed at present. More research is still needed in this area to be able to demonstrate whether screening for social risk, and especially for multiple domains of social risk, will succeed in meeting the Wilson and Jungner screening criteria.[97]
Health plan specific initiatives
Due to how new CMMI initiatives are, evidence supporting the effectiveness of its various initiatives of reducing healthcare spending and improving health outcomes of patients is relatively small, but is expected to grow within the coming years as many of CMMI's programs and initiatives will be due for their programmatic performance evaluation.[95] However, it remains that there is more evidence of smaller scale initiatives in individual health plans/hospitals/clinics, as several health plans, hospitals, and clinics have sought out to address social determinants of health within their scope of care.[97]
Transportation
Transportation is a key social determinant impacting patient outcomes with approximately 3.6 million individuals unable to receive the necessary medical care due to transportation barrier, according to recent study.[98] In addition, these 3.6 million experience multiple conditions at a much higher rate than those who have stable access to transportation. Many conditions that they face, however, can be managed if appropriate care is made available. For some conditions, this care is cost-effective and results in health care cost savings that outweigh added transportation costs.[98] without access to reliable, affordable, and convenient transportation, patients miss appointments and end up costing clinics money. According to a cross-study analysis, missed appointments and care delays cost the healthcare industry $150 billion each year.[99] Patients without transportation are also less likely to take medications as directed.[100] One study found that 65 percent of patients felt transportation assistance would enable them to fill prescriptions as directed after discharge.[100] According to a recent article published in the Journal of the American Medical Association, ridesharing services such as Lyft and Uber can improve that healthcare disparity and cut down on the $2.7 million the federal government spends each year on non-emergency medical transportation services.[101] To recover revenue and improve care quality, some health systems like MedStar Health and Denver Health Medical Center are teaming up with Uber, Lyft, and other ridesharing companies to connect patients with transportation.[101]
Housing
The University of Illinois Hospital, part of the University of Illinois Hospital & Health Sciences System, identified that large portion of the individuals with high rates of emergency department were also chronically homeless, and that these individuals were in the 10th decile for patient cost, with annual per patient expenses ranging from $51,000 to $533,000.[102] The University of Illinois partnered with a community group called the Center for Housing and Health to initiate the Better Health Through Housing initiative in 2015, an initiative that connected chronically homeless individuals with transitional housing and case managers. In partnering with the Center for Housing and Health, the University of Illinois Hospital saw participant healthcare costs fall 42 percent, and more recent studies have found that costs dropped by 61 percent. The hospital's emergency department reported a 35% reduction in use.[102]
Malnutrition
Some health plans have chosen to address some SDOH within their own means by establishing programs that directly deal with a single risk factor. Studies show that malnutrition can lead to higher costs of care and extended hospital states with the average hospital stay costing nearly $2,000 per day.[103] Advocate Health Care, an accountable care organization in Chicago, Illinois, implemented a nutrition care program at four of its Chicago area hospitals, an initiative that resulted in more than $4.8 million in cost savings within 6 months due to shorter hospital states and lower readmission rates (reduced 30 day readmission rates by 27% and the average hospital stay by nearly two days).[103]
Trump administration efforts
In 2016, Donald Trump was elected president on a platform that included a pledge to "repeal and replace" the Patient Protection and Affordable Care Act (commonly called the Affordable Care Act or Obamacare). Trump proposed the American Health Care Act (AHCA), which was drafted and passed by the House of Representatives in 2017 but did not pass the Senate. Had the AHCA become law, it would have returned insurance and healthcare to the market, leaving around 18 million Americans uninsured.[104]
Incentivizing health reimbursement arrangements is another goal.[105]
See also
- Broccoli argument
- Comparison of the healthcare systems in Canada and the United States
- Health care reform
- Health care reforms proposed during the Obama administration
- Health care system § International comparisons
- Health economics
- Health policy
- List of healthcare reform advocacy groups in the United States
- McCarran–Ferguson Act
- Medicare Sustainable Growth Rate
References
- Stolberg, Sheryl Gay; Pear, Robert (March 24, 2010). "Obama signs health care overhaul bill, with a flourish". The New York Times. p. A19. Retrieved March 23, 2010.
- Pear, Robert; Herszenhorn, David M. (March 22, 2010). "Obama hails vote on health care as answering 'the call of history'". The New York Times. p. A1. Retrieved March 22, 2010.
With the 219-to-212 vote, the House gave final approval to legislation passed by the Senate on Christmas Eve.
- Smith, Donna; Alexander, David; Beech, Eric (March 19, 2010). "Factbox – U.S. healthcare bill would provide immediate benefits". Reuters. Retrieved March 24, 2010.
- "Timeline: when healthcare reform will affect you". CNN. March 26, 2010. Retrieved March 24, 2010.
- Rosenthal, Elisabeth (December 21, 2013). "News Analysis – Health Care's Road to Ruin". The New York Times. Retrieved December 22, 2013.
- "Brief history of the Medicare program". San Antonio, Tex.: New Tech Media. 2010. Archived from the original on June 28, 2010. Retrieved August 31, 2010.
- Ball, Robert M. (October 24, 1961). "The role of social insurance in preventing economic dependency (address at the Second National Conference on the Churches and Social Welfare, Cleveland, Ohio)". Washington, D.C.: U.S. Social Security Administration. Retrieved August 31, 2010.
- Robert M. Ball, the then Deputy Director of the Bureau of Old-Age and Survivors Insurance in the Social Security Administration, had defined the major obstacle to financing health insurance for the elderly several years earlier: the high cost of care for the aged and the generally low incomes of retired people. Because retired older people use much more medical care than younger, employed people, an insurance premium related to the risk for older people needed to be high, but if the high premium had to be paid after retirement, when incomes are low, it was an almost impossible burden for the average person. The only feasible approach, he said, was to finance health insurance in the same way as cash benefits for retirement, by contributions paid while at work, when the payments are least burdensome, with the protection furnished in retirement without further payment.
- "An employee's guide to health benefits under COBRA – The Consolidated Omnibus Budget Reconciliation Act of 1986" (PDF). Washington, D.C.: Employee Benefits Security Administration, U.S. Department of Labor. 2010. Archived from the original (PDF) on December 27, 2013. Retrieved November 8, 2009.
- http://www.gpo.gov/fdsys/pkg/PLAW-104publ191/html/PLAW-104publ191.htm
- "What is SCHIP?". Washington, D.C.: National Center for Public Policy Research. 2007. Retrieved September 1, 2010.
- Kuraitis V. (2010). Pilots, Demonstrations & Innovation in the PPACA Healthcare Reform Legislation. e-CareManagement.com.
- Gawande A (December 2009). "Testing, Testing". The New Yorker. Retrieved March 22, 2010.
- "Health at a Glance 2017 - OECD Indicators - en - OECD". www.oecd.org.
- "FastStats". www.cdc.gov. July 18, 2017.
- "OECD Health Statistics 2017 - OECD". www.oecd.org.
- "Why does health care cost so much in America? Ask Harvard's David Cutler". PBS NewsHour. November 19, 2013.
- Hixon, Todd. "Why Are U.S. Health Care Costs So High?". forbes.com.
- Fuchs, Victor R. (July 23, 2014). "Why Do Other Rich Nations Spend So Much Less on Healthcare?". theatlantic.com.
- "The Senate bill does nothing to fix America's biggest health care problem". vox.com. June 30, 2017.
- WHO (May 2009). "World Health Statistics 2009". World Health Organization. Archived from the original on May 25, 2009. Retrieved August 2, 2009.
- Funk, Josh (March 1, 2010). "Buffett says economy recovering but at slow rate". San Francisco Chronicle. SFGate.com. Archived from the original on March 6, 2010. Retrieved April 3, 2010.
- Link between health spending and life expectancy: US is an outlier. May 26, 2017. By Max Roser at Our World in Data. Click the sources tab under the chart for info on the countries, healthcare expenditures, and data sources. See the later version of the chart here.
- Kenworthy, Lane (July 10, 2011). "America's inefficient health-care system: another look". Consider the Evidence (blog). Retrieved September 11, 2012.
- "coming_gen_storm_e.indd" (PDF). The Economist. Retrieved January 12, 2012.
- "Charlie Rose-Peter Orszag Interview Transcript". November 3, 2009. Archived from the original on January 11, 2012. Retrieved January 12, 2012.
- "Health Insurance Premiums Rise 6.1% In 2007, Less Rapidly Than In Recent Years But Still Faster Than Wages And Inflation" (Press release). Kaiser Family Foundation. September 11, 2007. Archived from the original on March 29, 2013. Retrieved September 13, 2007.
- Cathy Schoen; Michelle M. Doty; Sara R. Collins; Alyssa L. Holmgren (June 14, 2005). "Insured But Not Protected: How Many Adults Are Underinsured?". Health Affairs Web Exclusive. Suppl Web Exclusives: W5–289–W5–302. doi:10.1377/hlthaff.w5.289. PMID 15956055.
- Dale Yamamoto, Tricia Neuman and Michelle Kitchman Strollo, How Does the Benefit Value of Medicare Compare to the Benefit Value of Typical Large Employer Plans?, Kaiser Family Foundation, September 2008
- Himmelstein DU, Warren E, Thorne D, Woolhandler S (2005). "Illness and injury as contributors to bankruptcy". Health Aff (Millwood). Suppl Web Exclusives: W5–63–W5–73. doi:10.1377/hlthaff.w5.63. PMID 15689369. S2CID 73034397.
- Todd Zywicki, "An Economic Analysis of the Consumer Bankruptcy Crisis", 99 NWU L. Rev. 1463 (2005)
- "American Journal of Public Health | December 2009, Vol 99, No. 12" (PDF).
- "State-by-state breakout of excess deaths from lack of insurance" (PDF).
- A 1997 study carried out by Professors David Himmelstein and Steffie Woolhandler (New England Journal of Medicine 336, no. 11 1997) "concluded that almost 100,000 people died in the United States each year because of lack of needed care—three times the number of people who died of AIDs." The Inhuman State of U.S. Health Care, Monthly Review, Vicente Navarro, September 2003. Retrieved September 10, 2009
- "Study calls wide Mass. coverage a lifesaver". Boston Globe. May 5, 2014.
- Craig, David M. (January 1, 2014). CRAIG, DAVID M. (ed.). Health Care as a Social Good. Health Care as a Social Good. Religious Values and American Democracy. Georgetown University Press. pp. 85–120. ISBN 9781626160774. JSTOR j.ctt7zswmt.7.
- Chernomas, Robert; Hudson, Ian (January 1, 2013). To Live and Die in America: Class, Power, Health and Healthcare. Pluto Books. ISBN 9780745332123. JSTOR j.ctt183p79j.
- Ehrenreich, John (January 1, 2016). "The Health of Nations". In Ehrenreich, John (ed.). Third Wave Capitalism. Third Wave Capitalism. How Money, Power, and the Pursuit of Self-Interest Have Imperiled the American Dream. Cornell University Press. pp. 39–77. doi:10.7591/9781501703591-004. ISBN 9781501702310. JSTOR 10.7591/j.ctt1h4mjdm.6.
- Chen, Jie; Vargas-Bustamante, Arturo; Mortensen, Karoline; Ortega, Alexander N. (February 2016). "Racial and Ethnic Disparities in Health Care Access and Utilization Under the Affordable Care Act". Medical Care. 54 (2): 140–146. doi:10.1097/MLR.0000000000000467. ISSN 0025-7079. PMC 4711386. PMID 26595227.
- Alonso-Zaldivar, Ricardo (March 10, 2014). "Survey: Uninsured Rate Drops; Health Law Cited". The Associated Press. Archived from the original on March 10, 2014. Retrieved March 10, 2014.
- Easley, Jason (March 10, 2014). "Republicans Darkest Fears Realized: ACA Causes Number of Uninsured to Drop Across All Ages". Politicus USA. Retrieved March 10, 2014.
- Howell, Tom (March 10, 2014). "Rate of uninsured Americans is dropping: Gallup". Washington Times. Retrieved March 10, 2014.
- Pear, Robert (December 3, 2011). "Health Official Takes Parting Shot at 'Waste'". New York Times. Retrieved December 20, 2011.
- Phipps, Jennie L. (February 21, 2013). "How big is Medicare fraud?". Retirement Blog. Bankrate. Retrieved November 28, 2013.
- "Medicare Fraud Strike Force Charges 89 Individuals for Approximately $223 Million in False Billing". U.S. Department of Justice. May 14, 2013. Retrieved November 28, 2013.
- Skinner, Daniel (2013). "Defining Medical Necessity under the Patient Protection and Affordable Care Act". Public Administration Review. 73: S49–S59. doi:10.1111/puar.12068. ISSN 0033-3352. JSTOR 42003021.
- SOMMERS, BENJAMIN D.; McMURTRY, CAITLIN L.; BLENDON, ROBERT J.; BENSON, JOHN M.; SAYDE, JUSTIN M. (2017). "Beyond Health Insurance: Remaining Disparities in US Health Care in the Post-ACA Era". The Milbank Quarterly. 95 (1): 43–69. doi:10.1111/1468-0009.12245. ISSN 0887-378X. JSTOR 26300309. PMC 5339398. PMID 28266070.
- For-Profit Hospitals Cost More and Have Higher Death Rates, Physicians for a National Health Program
- For-Profit HMOs Provide Worse Quality Care, Physicians for a National Health Program
- "Prelims i-ixx/E" (PDF). Retrieved January 12, 2012.
- David Gratzer, Why Is not Government Health Care The Answer? Archived March 12, 2009, at the Wayback Machine, Free Market Cure, July 16, 2007
- Glen Whitman, "WHO's Fooling Who? The World Health Organization's Problematic Ranking of Health Care Systems", Cato Institute, February 28, 2008
- Capital: In health care, consumer theory falls flat David Wessel, Wall Street Journal, September 7, 2006.
- "Rand study finds patients' ratings of their medical care do not reflect the technical quality of their care" (Press release). RAND Corporation. May 1, 2006. Retrieved August 27, 2007.
- Chang JT, Hays RD, Shekelle PG, et al. (May 2006). "Patients' global ratings of their health care are not associated with the technical quality of their care". Ann. Intern. Med. 144 (9): 665–72. CiteSeerX 10.1.1.460.3525. doi:10.7326/0003-4819-144-9-200605020-00010. PMID 16670136. S2CID 53091172.
- Health Affairs, Volume 20, No. 2. "Americans' Views on Health Policy: A Fifty-Year Historical Perspective." March/April 2001. http://content.healthaffairs.org/content/20/2/33.full.pdf+html
- "Michael Moore claims a majority favor a single-payer health care system". PolitiFact. Retrieved November 20, 2011.
- Blendon Robert J.; et al. (1989). "Views on health care: Public opinion in three nations". Health Affairs. 8 (1): 149–57. doi:10.1377/hlthaff.8.1.149. PMID 2707718.
- Los Angeles Times poll: "Health Care in the United States," Poll no. 212, Storrs, Conn.: Administered by the Roper Center for Public Opinion Research, March 1990
- Wall Street Journal-NBC poll: Michael McQueen, "Voters, sick of the current health –care systems, want federal government to prescribe remedy," The Wall Street Journal, June 28, 1991
- AP/Yahoo poll: Administered by Knowledge Networks, December 2007: http://surveys.ap.org/data/KnowledgeNetworks/AP-Yahoo_2007-08_panel02.pdf Archived October 5, 2013, at the Wayback Machine
- Los Angeles Times/Bloomberg: President Bush, Health Care, The Economy. Archived September 8, 2015, at the Wayback Machine October 25, 2007.
- TIME MAGAZINE/ABT SRBI – July 27–28, 2009 Survey: "Archived copy" (PDF). Archived from the original (PDF) on December 31, 2010. Retrieved September 13, 2009.
{{cite web}}: CS1 maint: archived copy as title (link) - Rasmussen Reports: Rasmussen Reports. January 1, 2010. Retrieved November 20, 2011.
- Rasmussen Reports: Rasmussen Reports. Retrieved December 30, 2012.
- Sack, Kevin (June 20, 2009). "In Poll, Wide Support for Government-Run Health". The New York Times. Retrieved January 12, 2012.
- "CBS News/New York Times Poll, For Release: Sunday, February 1, 2009, 9:00 AM, American Public Opinion: Today Vs. 30 Years Ago, January 11–15, 2009" (PDF). CBS News. Retrieved February 19, 2015.
- "Here's an initial summary of headlines from our health care poll, followed by the full trended results" (PDF). ABC News. Retrieved January 12, 2012.
- "Kaiser Health Tracking Poll: July 2009 – Topline" (PDF). July 2, 2009. Retrieved January 12, 2012.
- "Tracking Public Opinion on National Health Plan: Interactive". The Henry J. Kaiser Family Foundation. April 24, 2019. Retrieved May 7, 2019.
- "Public Opinion on Single-Payer, National Health Plans, and Expanding Access to Medicare Coverage". The Henry J. Kaiser Family Foundation. April 24, 2019. Retrieved May 7, 2019.
- Quinnipiac University – Office of Public Affairs (April 2, 2008). "Question 9: "Do you think it's the government's responsibility to make sure that everyone in the United States has adequate health-care, or don't you think so?"". Quinnipiac.edu. Archived from the original on October 31, 2011. Retrieved January 12, 2012.
- Institute of Medicine, Committee on the Consequences of Uninsurance; Board on Health Care Services (2003). Hidden Costs, Value Lost: Uninsurance in America. Washington, DC: The National Academies Press. doi:10.17226/10719. ISBN 9780309089319. PMID 25057665.
- Lincoln, Taylor (April 8, 2014). "Severing the Tie That Binds: Why a Publicly Funded, Universal Health Care System Would Be a Boon to U.S. Businesses" (PDF). Public Citizen. Retrieved May 20, 2014.
- Ungar, Rick (April 6, 2012). "A Dose Of Socialism Could Save Our States – State Sponsored, Single Payer Healthcare Would Bring In Business & Jobs". Forbes. Retrieved May 20, 2014.
- Hogg, W.; Baskerville, N.; Lemelin, J. (2005). "Cost savings associated with improving appropriate and reducing inappropriate preventive care: Cost-consequences analysis". BMC Health Services Research. 5 (1): 20. doi:10.1186/1472-6963-5-20. PMC 1079830. PMID 15755330.
- Kao-Ping Chua; Flávio Casoy (June 16, 2007). "Single Payer 101". American Medical Student Association. Archived from the original on December 12, 2010. Retrieved May 20, 2014.
- Hogg, W.; Baskerville, N; Lemelin, J (2005). "Cost savings associated with improving appropriate and reducing inappropriate preventive care: cost-consequences analysis". BMC Health Services Research. 5 (1): 20. doi:10.1186/1472-6963-5-20. PMC 1079830. PMID 15755330.
- PolitiFact: Barack Obama says preventive care 'saves money'. February 10, 2012.
- Krugman, Paul (June 13, 2005). "One Nation, Uninsured". The New York Times. Retrieved December 4, 2011.
- Physicians for a National Health Program (2008) "Single Payer System Cost?" Archived December 6, 2010, at the Wayback Machine PNHP.org
- Friedman, Gerald. "Funding a National Single-Payer System "Medicare for All" Would save Billions, and Could Be Redistributive". Dollars & Sense.
{{cite web}}: Missing or empty|url=(help) - "State-Based Single-Payer Health Care – A Solution for the United States?" Archived September 21, 2013, at the Wayback Machine New England Journal of Medicine 364;13:1188–90, March 31, 2011
- http://www.politico.com/story/2014/12/single-payer-vermont-113711.html Politico (20 Dec 2014). Accessed 20 May 2015.
- "Shumlin: It's 'Not The Right Time' For Single Payer". Vermont Public. December 17, 2014. Retrieved July 23, 2022.
- "Single- Payer healthcare plan advances in California Senate- without a way to pay its $400 billion tab". Los Angeles Times. ISSN 0458-3035. Retrieved August 6, 2017.
- Bindman, Andrew B.; Schneider, Andreas G. (April 21, 2011). "Catching a Wave — Implementing Health Care Reform in California". New England Journal of Medicine. 364 (16): 1487–1489. doi:10.1056/NEJMp1014109. ISSN 0028-4793. PMID 21449773.
- "Can California Implement a Single-Payer Health Care System Without Going to the Ballot? - California Budget & Policy Center". California Budget & Policy Center. July 21, 2017. Retrieved August 6, 2017.
- Karlamangla, Soumya (August 1, 2017). "Covered California premiums will rise 12.5%, and Anthem Blue Cross cuts coverage". Los Angeles Times. ISSN 0458-3035. Retrieved August 6, 2017.
- "House Dems push again for creation of government-run health insurance option" The Hill, January 16, 2013
- "Graduate Medical Education Funding Is Not Helping Solve Primary Care, Rural Provider Shortages, Study Finds". Robert Wood Johnson Foundation. June 19, 2013.
- The Medicare Bundled Payment Pilot Program: Participation Considerations
- Sunkara, Vasu; Rosenbaum, Sara (2016). "The Constitution and the Public's Health: The Consequences of the US Supreme Court's Medicaid Decision in NFIB v Sebelius". Public Health Reports. 131 (6): 844–846. doi:10.1177/0033354916670870. ISSN 0033-3549. JSTOR 26374030. PMC 5230834. PMID 28123233.
- Brecher, Charles (October 2013). "Medicaid's Next Metamorphosis". Public Administration Review. 73, The Health Care-Crucible Post-Reform: Challenges for Public Administration: S60–S68. doi:10.1111/puar.12116. JSTOR 42003022.
- "Beyond Health Care: The Role of Social Determinants in Promoting Health and Health Equity". The Henry J. Kaiser Family Foundation. May 10, 2018. Retrieved October 10, 2018.
- "Accountable Health Communities Model | Center for Medicare & Medicaid Innovation". innovation.cms.gov. Retrieved November 12, 2018.
- Billioux, A., K. Verlander, S. Anthony, and D. Alley. 2017. Standardized screening for health-related social needs in clinical settings: The accountable health communities screening tool. Discussion Paper, National Academy of Medicine, Washington, DC. https://nam.edu/wp-content/uploads/2017/05/ Standardized-Screening-for-Health-Related-Social-Needsin-Clinical-Settings.pdf
- Andermann, Anne (June 22, 2018). "Screening for social determinants of health in clinical care: moving from the margins to the mainstream". Public Health Reviews. 39: 19. doi:10.1186/s40985-018-0094-7. ISSN 0301-0422. PMC 6014006. PMID 29977645.
- Wallace, Richard; Hughes-Cromwick, Paul; Mull, Hillary; Khasnabis, Snehamay (January 2005). "Access to Health Care and Nonemergency Medical Transportation: Two Missing Links". Transportation Research Record: Journal of the Transportation Research Board. 1924: 76–84. CiteSeerX 10.1.1.114.4660. doi:10.1177/0361198105192400110. ISSN 0361-1981. S2CID 220737225.
- "How Behavioral Economics Can Help Cure the Health Care Crisis". Harvard Business Review. March 1, 2010. Retrieved November 12, 2018.
- Syed, Samina T.; Gerber, Ben S.; Sharp, Lisa K. (October 2013). "Traveling Towards Disease: Transportation Barriers to Health Care Access". Journal of Community Health. 38 (5): 976–993. doi:10.1007/s10900-013-9681-1. ISSN 0094-5145. PMC 4265215. PMID 23543372.
- Powers, Brian W.; Rinefort, Scott; Jain, Sachin H. (September 6, 2016). "Nonemergency Medical Transportation". JAMA. 316 (9): 921–2. doi:10.1001/jama.2016.9970. ISSN 0098-7484. PMID 27599325.
- "Case Study: University of Illinois Hospital & Health Sciences System's Better Health Through Housing Program | AHA News". American Hospital Association | AHA News. Retrieved November 12, 2018.
- Sriram, Krishnan; Sulo, Suela; VanDerBosch, Gretchen; Partridge, Jamie; Feldstein, Josh; Hegazi, Refaat A.; Summerfelt, Wm. Thomas (December 6, 2016). "A Comprehensive Nutrition-Focused Quality Improvement Program Reduces 30-Day Readmissions and Length of Stay in Hospitalized Patients". Journal of Parenteral and Enteral Nutrition. 41 (3): 384–391. doi:10.1177/0148607116681468. ISSN 0148-6071. PMID 27923890. S2CID 3792309.
- Galea, Sandro (2017). "How the Trump Administration's Policies May Harm the Public's Health". The Milbank Quarterly. 95 (2): 229–232. doi:10.1111/1468-0009.12255. ISSN 0887-378X. JSTOR 26300321. PMC 5461388. PMID 28589597.
- Keith, Katie (2018). "Administration Moves To Incentivize Health Reimbursement Arrangements". Health Affairs Forefront. doi:10.1377/forefront.20181026.832732.
Further reading
- Christensen, Clayton Hwang, Jason, Grossman, Jerome, The Innovator's Prescription, McGraw Hill, 2009. ISBN 978-0-07-159208-6.
- Terry L. Leap, Phantom Billing, Fake Prescriptions, and the High Cost of Medicine: Health Care Fraud and What to do about It (Cornell University Press, 2011).
- Mahar, Maggie, Money-Driven Medicine: The Real Reason Health Care Costs So Much, HarperCollins, 2006. ISBN 978-0-06-076533-0
- Starr, Paul, The Social Transformation of American Medicine, Basic Books, 1982. ISBN 0-465-07934-2
- Reid, T. R. (2009). The Healing of America: A Global Quest for Better, Cheaper and Fairer Health Care. Penguin Books. ISBN 978-1-59420-234-6.
External links
- Healthcare reform in the United States at Curlie