Automated external defibrillator
An automated external defibrillator (AED) is a portable electronic device that automatically diagnoses the life-threatening cardiac arrhythmias of ventricular fibrillation (VF) and pulseless ventricular tachycardia,[1] and is able to treat them through defibrillation, the application of electricity which stops the arrhythmia, allowing the heart to re-establish an effective rhythm.
| Automated external defibrillator | |
|---|---|
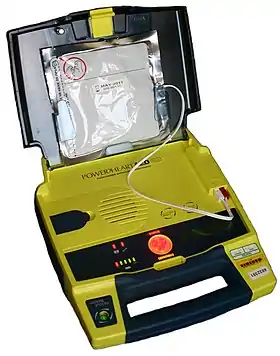 An opened and charged AED. This model is semi-automatic, due to the presence of a manual shock button. | |
| Acronym | AED |
| Synonyms | defibrillator, defib |
| Specialty | Cardiology |
| Inventor(s) | Frank Pantridge |
| Related items | Manual defibrillator |
With simple audio and visual commands, AEDs are designed to be simple to use for the layperson, and the use of AEDs is taught in many first aid, certified first responder, and basic life support (BLS) level cardiopulmonary resuscitation (CPR) classes.[2]
The portable version of the defibrillator was invented in the mid-1960s by Frank Pantridge in Belfast, Northern Ireland and the first automatic, public use, defibrillator was produced by the Cardiac Resuscitation Company in the late 1970s. The unit was launched under the name Heart-Aid.[3]
Indications

Conditions that the device treats
An automated external defibrillator is used in cases of life-threatening cardiac arrhythmias which lead to sudden cardiac arrest, which is not the same as a heart attack. The rhythms that the device will treat are usually limited to:
- Pulseless Ventricular tachycardia (shortened to VT or V-Tach)[1]
- Ventricular fibrillation (shortened to VF or V-Fib)
In each of these two types of shockable cardiac arrhythmia, the heart is electrically active, but in a dysfunctional pattern that does not allow it to pump and circulate blood. In ventricular tachycardia, the heart beats too fast to effectively pump blood. Ultimately, ventricular tachycardia leads to ventricular fibrillation. In ventricular fibrillation, the electrical activity of the heart becomes chaotic, preventing the ventricle from effectively pumping blood. The fibrillation in the heart decreases over time, and will eventually reach asystole.
AEDs, like all defibrillators, are not designed to shock asystole ('flat line' patterns) as this will not have a positive clinical outcome. The asystolic patient only has a chance of survival if, through a combination of CPR and cardiac stimulant drugs, one of the shockable rhythms can be established, which makes it imperative for CPR to be carried out prior to the arrival of a defibrillator.
Effect of delayed treatment
Uncorrected, these cardiac conditions (ventricular tachycardia, ventricular fibrillation, asystole) rapidly lead to irreversible brain damage and death, once cardiac arrest takes place. After approximately three to five minutes in cardiac arrest,[4] irreversible brain/tissue damage may begin to occur. For every minute that a person in cardiac arrest goes without being successfully treated (by defibrillation), the chance of survival decreases by 7 percent per minute in the first 3 minutes, and decreases by 10 percent per minute as time advances beyond ~3 minutes.[5]
Requirements for use

AEDs are designed to be used by laypersons who ideally should have received AED training. However, sixth-grade students have been reported to begin defibrillation within 90 seconds, as opposed to a trained operator beginning within 67 seconds.[6] This is in contrast to more sophisticated manual and semi-automatic defibrillators used by health professionals, which can act as a pacemaker if the heart rate is too slow (bradycardia) and perform other functions which require a skilled operator able to read electrocardiograms.
Bras with a metal underwire and piercings on the torso must be removed before using the AED on someone to avoid interference.[7][8] American television show MythBusters found evidence that use of a defibrillator on a woman wearing an underwire bra can lead to arcing or fire but only in unusual and unlikely circumstances.[9]
In a study analyzing the effects of having AEDs immediately present during Chicago's Heart Start program over a two-year period, of 22 individuals, 18 were in a cardiac arrhythmia which AEDs can treat. Of these 18, 11 survived. Of these 11 patients, 6 were treated by bystanders with absolutely no previous training in AED use.[10][11]
Implementation
Placement and availability
Automated external defibrillators are generally either kept where health professionals and first responders can use them (health facilities and ambulances) as well as public access units which can be found in public places including corporate and government offices, shopping centres, restaurants, public transport, and any other location where people may congregate.

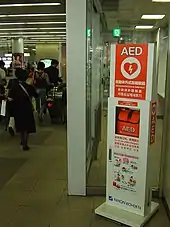
In order to make them highly visible, public access AEDs are often brightly coloured and are mounted in protective cases near the entrance of a building. When these protective cases are opened or the defibrillator is removed, some will sound a buzzer to alert nearby staff to their removal, though this does not necessarily summon emergency services; trained AED operators should know to phone for an ambulance when sending for or using an AED. In September 2008, the International Liaison Committee on Resuscitation issued a 'universal AED sign' to be adopted throughout the world to indicate the presence of an AED, and this is shown on the right.[12]
A trend that is developing is the purchase of AEDs to be used in the home, particularly by those with known existing heart conditions.[13] The number of devices in the community has grown as prices have fallen to affordable levels. There has been some concern among medical professionals that these home users do not necessarily have appropriate training,[14] and many advocate the more widespread use of community responders, who can be appropriately trained and managed.
Typically, an AED kit will contain a face shield for providing a barrier between patient and first aider during rescue breathing; a pair of nitrile rubber gloves; a pair of trauma shears for cutting through a patient's clothing to expose the chest; a small towel for wiping away any moisture on the chest, and a razor for shaving those with very hairy chests.[15]
Preparation for operation
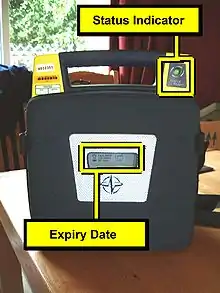
Most manufacturers recommend checking the AED before every period of duty or on a regular basis for fixed units. Some units need to be switched on in order to perform a self check; other models have a self check system built in with a visible indicator.
All manufacturers mark their electrode pads with an expiration date, and it is important to ensure that the pads are in date. The typical life expectancy of AED pads are between 18 and 30 months.[16] This is usually marked on the outside of the pads. Some models are designed to make this date visible through a 'window', although others will require the opening of the case to find the date stamp.
It is also important to ensure that the AED unit's batteries have not expired. The AED manufacturer will specify how often the batteries should be replaced. Each AED has a different recommended maintenance schedule outlined in the user manual. Common checkpoints on every checklist, however, also include a monthly check of the battery power by checking the green indicator light when powered on, condition and cleanliness of all cables and the unit, and check for the adequate supplies [17]
Mechanism of operation
An AED is "automatic" because of the unit's ability to autonomously analyse the patient's condition. To assist this, the vast majority of units have spoken prompts, and some may also have visual displays to instruct the user.
"External" refers to the fact that the operator applies the electrode pads to the bare chest of the victim (as opposed to internal defibrillators, which have electrodes surgically implanted inside the body of a patient).
When turned on or opened, the AED will instruct the user to connect the electrodes (pads) to the patient. Once the pads are attached, everyone should avoid touching the patient so as to avoid false readings by the unit. The pads allow the AED to examine the electrical output from the heart and determine if the patient is in a shockable rhythm (either ventricular fibrillation or ventricular tachycardia). If the device determines that a shock is warranted, it will use the battery to charge its internal capacitor in preparation to deliver the shock. The device system is not only safer - charging only when required, but also allows for a faster delivery of the electric current.
When charged, the device instructs the user to ensure no one is touching the patient and then to press a button to deliver the shock; human intervention is usually required to deliver the shock to the patient in order to avoid the possibility of accidental injury to another person (which can result from a responder or bystander touching the patient at the time of the shock). Depending on the manufacturer and particular model, after the shock is delivered most devices will analyze the patient and either instruct CPR to be performed, or prepare to administer another shock.
Many AED units have an 'event memory' which store the ECG of the patient along with details of the time the unit was activated and the number and strength of any shocks delivered. Some units also have voice recording abilities[18] to monitor the actions taken by the personnel in order to ascertain if these had any impact on the survival outcome. All this recorded data can be either downloaded to a computer or printed out so that the providing organisation or responsible body is able to see the effectiveness of both CPR and defibrillation. Some AED units even provide feedback on the quality of the compressions provided by the rescuer.[19][20]
The first commercially available AEDs were all of a monophasic type, which gave a high-energy shock, up to 360 to 400 joules depending on the model. This caused increased cardiac injury and in some cases second and third-degree burns around the shock pad sites. Newer AEDs (manufactured after late 2003) have tended to utilise biphasic algorithms which give two sequential lower-energy shocks of 120–200 joules, with each shock moving in an opposite polarity between the pads. Others may give a stepped approach to energy delivery, usually in a 200J, a second 200J, then 300J, and finally 360J shock, with any further shocks also being 360 Joules. This lower-energy waveform has proven more effective in clinical tests, as well as offering a reduced rate of complications and reduced recovery time.[21]
Usage
Simplicity of use

Unlike regular defibrillators, an automated external defibrillator (AED) requires minimal training to be used (or even no training). That is possible because all AEDs approved for use in the United States and many other countries use an electronic voice to prompt users through each step. And, in case of the user of an AED may be hearing impaired, many AEDs now include visual prompts as well. Most units are designed for use by non-medical operators. Their ease of use has given rise to the notion of public access defibrillation (PAD).
Besides, the AED automatically diagnoses the heart rhythm and determines if a shock is needed. Automatic models will administer the shock without the user's command. Semi-automatic models will tell the user that a shock is needed, but the user must tell the machine to do so, usually by pressing a button. In most circumstances, the user cannot override a "no shock" advisory by an AED. Some AEDs may be used on children – those under 55 lbs (25 kg) in weight or under age 8. If a particular model of AED is approved for pediatric use, all that is required is the use of more appropriate pads.[22]
Benefit
Observational studies have shown that in out of hospital cardiac arrest, public access defibrillators when used were associated with 40% median survival. When operated by non-dispatched lay first responders they have the highest likelihood of leading to survival.[23]
United States
Automated external defibrillators are now easy enough to use that most states in the United States include the "good faith" use of an AED by any person under Good Samaritan laws.[24] "Good faith" protection under a Good Samaritan law means that a volunteer responder (not acting as a part of one's occupation) cannot be held civilly liable for the harm or death of a victim by providing improper or inadequate care, given that the harm or death was not intentional and the responder was acting within the limits of their training and in good faith. In the United States, Good Samaritan laws provide some protection for the use of AEDs by trained and untrained responders.[25] AEDs create little liability if used correctly;[26] NREMT-B and many state Emergency Medical Technician (EMT) training and many CPR classes incorporate or offer AED education as a part of their program.
Canada
In addition to Good Samaritan laws, Ontario, Canada also has the "Chase McEachern Act (Heart Defibrillator Civil Liability), 2007 (Bill 171 – Subsection N)", passed in June, 2007,[27] which protects individuals from liability for damages that may occur from their use of an AED to save someone's life at the immediate scene of an emergency unless damages are caused by gross negligence.
Australia
Legislation in Australia varies by state, with separate liability issues relating to providing and using AED equipment. Each state and territory has enacted "Good Samaritan" laws that offer legal protection to a person who gives assistance in a medical emergency - the standard of care expected corresponds to their training (or lack of training).[28] In New South Wales, the Work Health and Safety Regulation (2011) requires an employer to use a risk assessment to ensure that there is adequate provision for first aid; when there is a sufficient risk it warrants providing a defibrillator.[29]
Reliability
In 2012, AED's (automated external defibrillators) were under scrutiny by the U.S. Food and Drug Administration (FDA) which considered reclassifying AEDs as class III premarket approval devices. Technical malfunctions likely contributed to more than 750 deaths in the 5-year period between 2004 and 2009, in most cases by component failures or design errors. During the same period, up to 70 types of AEDs were recalled, including recalls from every AED manufacturer in the world. [30]
In January and February 2015, the FDA issued this news release: "The FDA issued a final order that will require AED manufacturers to submit premarket approval applications (PMAs), which undergo a more rigorous review than what was required to market these devices in the past. The agency's strengthened review will focus on the critical requirements needed to ensure the safety and reliability of AEDs and their necessary accessories, including batteries, pad electrodes, adapters and hardware keys for pediatric use."[31][32]
In the United Kingdom there is concern that poor maintenance may make public defibrillators unreliable. The Henley Standard reported on 21 July 2017 that more than half the defibrillators in Henley-on-Thames and the surrounding area were at risk of failing, either because of low battery power or because adhesive pads had deteriorated.[33]
History
The first use of an external defibrillator on a human was in 1947 by Claude Beck.[34] The portable version of the external defibrillator was invented in the mid-1960s by Frank Pantridge in Belfast, Northern Ireland, a pioneer in emergency medical treatment.[35][36] Pantridge's defibrillator required a trained operator to perform the shock procedure and charted a course for many new innovations in external defibrillation.[37]
In the late 1970s the Heart-Aid was developed as the first truly automated external defibrillator that was designed for the public. The principles of ABC assessment and a human voice relaying instructions helped bystanders respond to a sudden cardiac event while waiting for the first responders to get to scene.[3] Many of the early innovations in the Heart-Aid model are still part of the current generation of AEDs, although some innovations, like the airway electrode have fallen from use.
Case studies
In a study published in 2017, researchers in Poland selected the main entrances of buildings which had AEDs, although the researchers themselves did not know the exact locations of the devices. In drills of pretend heart attack, the average time to bring the AED to the patient was 96 seconds, with a time that ranged from 52 to 144 seconds. This met the three minute goal. In some cases, the use of the AED required the continuous presence of building personnel. Future improvements include more obvious signage and public-access AEDs which do not require a staff member of the building to either retrieve or use the device.[38] [39]
See also
- Cardiopulmonary resuscitation
- Defibrillation
- Advanced cardiac life support
- Cardioversion
References
- Kerber, Richard E; Becker, Lance B; Bourland, Joseph D; Cummins, Richard O; Hallstrom, Alfred P; Michos, Mary B; Nichol, Graham; Ornato, Joseph P; Thies, William H; White, Roger D; Zuckerman, Bram D (March 18, 1997). "Automatic External Defibrillators for Public Access Defibrillation". Circulation. American Heart Association. 95 (1677–1682): 1677–82. doi:10.1161/01.cir.95.6.1677. PMID 9118556.
- "CPR Adult Courses". American Red Cross. Archived from the original on 3 July 2007. Retrieved 2007-06-28.
- "Heart-Aid Defibrillator". EMS Museum. Retrieved 2021-07-13.
- "Cardiopulmonary Resuscitation (CPR) Statistics". American Red Cross. Archived from the original on 19 November 2008. Retrieved 2008-10-27.
- American Red Cross. CPR/AED for the Professional Rescuer (participant's manual). Yardley, PA: StayWell, 2006. p. 63.
- U.S. Department of Labor Occupational Safety and Health Administration (2001). "Cardiac arrest a automated external defibrillators (AEDs)". OSHA Publication No. TIB 01-12-17.
- "How To Use an Automated External Defibrillator". National Heart Lung and Blood Institute. Archived from the original on 23 June 2011. Retrieved 24 May 2011.
- de Vries, Lloyd (2006-03-22). "Breathing Easier". CBS News. Archived from the original on 29 April 2009. Retrieved 2009-04-22.
We got a short lesson in using an AED, which is an Automated External Defibrillator. We had the thrill of yelling, "Clear!" Unfortunately this also brought on a little anxiety when Sean mentioned if the patient were a woman with a metal underwire in her bra or with metal piercings on her torso, we'd have to remove them.
- "Underwire Bra Can Mess with Defibrillator". 2012-04-11.
- Caffrey SL, Willoughby PJ, Pepe PE, Becker LB (October 2002). "Public use of automated external defibrillators". N. Engl. J. Med. 347 (16): 1242–47. doi:10.1056/NEJMoa020932. PMID 12393821.
- "Look for me in airports/Hockey arenas". 2010-02-10.
- "ILCOR presents a universal AED sign". European Resuscitation Council. Archived from the original on 2016-08-11. Retrieved 2019-10-07.
- "Heartstart Home Defibrillator". Philips Electronics. Archived from the original on 13 June 2007. Retrieved 2007-06-15.
- Barnaby, Barnaby J (2005-05-03). "Do It Yourself: The Home Heart Defibrillator". New York Times. Retrieved 2007-06-15.
- CPR/AED for the Professional Rescuer, supra, p. 65 ("[a] safety surgical razor should be included in the AED kit.") The other items not directly mentioned in this text but are used in AED preparation, such as the gloves (used throughout patron assessment) and the towel, as the chest should be dried prior to AED pad attachment (id, at p. 64).
- "Why Do AED Defibrillator Pads Expire". AED Brands. Retrieved 2021-07-28.
- Northwest Health; Safety Inc. "AED Universe: A Northwest Health and Safety Company". Retrieved 21 January 2013.
- "ZOLL® AED Plus® Package w/Voice Recording". AED Superstore. Retrieved 2016-05-12.
- "Zoll AED Plus Provides Compression Feedback". Archived from the original on 2021-03-07. Retrieved 2018-08-21.
- HeartSine AED CPR Advisor detects Compressions depth and rate feedback
- "AED Plus Biphasic Waveform". ZOLL Medical Corporation. Archived from the original on 2009-04-29. Retrieved 2008-10-27.
- "AEDS Guide". Monday, March 16, 2020
- Bækgaard, Josefine S.; Viereck, Søren; Møller, Thea Palsgaard; Ersbøl (2017). "The Effects of Public Access Defibrillation on Survival After Out-of-Hospital Cardiac Arrest: A Systematic Review of Observational Studies". Circulation. 136 (10): 954–965. doi:10.1161/CIRCULATIONAHA.117.029067. PMID 28687709. S2CID 21249432.
- Laws on Cardiac Arrest and Defibrillators, 2013 update. National Conference of State Legislatures. Retrieved on 2013-03-18.
- "Archived copy". Archived from the original on 2002-10-16. Retrieved 2007-07-22.
{{cite web}}: CS1 maint: archived copy as title (link) - Laws on Cardiac Arrest and Defibrillators
- Health System Improvement Act, 2007 Retrieved on 26 June 2007
- "Legal and Ethical Issues Related to Resuscitation - Section 10: Guideline 10.5" (PDF). Australian Resuscitation Council. 2015. Retrieved 16 October 2020.
- "Work Health and Safety Act 2011 No 10". legislation.nsw.gov.au. Retrieved 16 October 2020.
- "The Shocking Truth About Defibrillators". IEEE Spectrum, March 2012. Retrieved 2012-07-28. 2012-02-27.
- "FDA takes steps to improve reliability of automated external defibrillators". FDA News Release, January 2015. Retrieved 2017-07-15.
- "Effective Date of Requirement for Premarket Approval for Automated External Defibrillator Systems; Republication". Federal Register, February 3, 2015. Retrieved 2017-07-15. 2015-02-03.
- White, David (21 July 2017). "Life-savers out of date". Henley Standard.
- "Claude Beck, defibrillation and CPR". Case Western Reserve University. Archived from the original on 2007-10-24. Retrieved 2007-06-15.
- Shurlock, B (18 December 2007). "Pioneers in cardiology: Frank Pantridge, CBE, MC, MD, FRCP, FACC". Circulation. 116 (25): f145–48. doi:10.1161/CIRCULATIONAHA.107.187677. PMID 18086933.
- Evans, Alun (April 2, 2005). "Frank Pantridge". BMJ. 330 (7494): 793. doi:10.1136/bmj.330.7494.793. PMC 555899.
- "EMS Innovators". EMS Museum. Retrieved 2021-07-13.
- Telec W, Baszko A, Dąbrowski M, Dąbrowska A, Sip M, Puslecki M, Kłosiewicz T, Potyrała P, Jurczyk W, Maciejewski A, Zalewski R, Witt M, Ladny JR, Szarpak L (2018). "Automated external defibrillator use in public places: a study of acquisition time". Kardiol Pol. 76 (1): 181–185. doi:10.5603/KP.a2017.0199. PMID 29168550.
{{cite journal}}: CS1 maint: multiple names: authors list (link) - AED master
External links
- Sudden Cardiac Arrest Foundation
- American Heart Association: Learn & Live
- American Red Cross: Learn About Automated External Defibrillators
- FDA Heart Health Online: Automated External Defibrillator (AED)
- Resuscitation Council (UK)
- Sudden Cardiac Arrest Foundation (AU)
- The National EMS Museum
- Public Access Defibrillators
Emergency medicine | |
|---|---|
| Emergency medicine |
|
| Equipment |
|
| Drugs | |
| Organisations |
|
| Courses / Life support |
|
| Scoring systems |
|
| |