Non-small-cell lung carcinoma
Non-small-cell lung carcinoma (NSCLC) is any type of epithelial lung cancer other than small-cell lung carcinoma (SCLC). NSCLC accounts for about 85% of all lung cancers.[1][2][3] As a class, NSCLCs are relatively insensitive to chemotherapy, compared to small-cell carcinoma. When possible, they are primarily treated by surgical resection with curative intent, although chemotherapy has been used increasingly both preoperatively (neoadjuvant chemotherapy) and postoperatively (adjuvant chemotherapy).
| Nonsmall-cell lung carcinoma | |
|---|---|
 | |
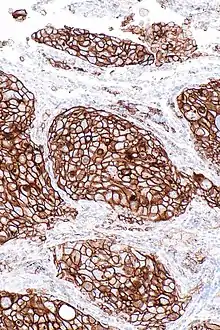
| Micrograph of a squamous carcinoma, a type of nonsmall-cell lung carcinoma, FNA specimen, Pap stain. | |
| Specialty | Oncology |
Types

The most common types of NSCLC are squamous-cell carcinoma, large-cell carcinoma, and adenocarcinoma, but several other types occur less frequently. A few of the less common types are pleomorphic, carcinoid tumor, salivary gland carcinoma, and unclassified carcinoma.[5] All types can occur in unusual histologic variants and as mixed cell-type combinations.[6] Nonsquamous-cell carcinoma almost occupies the half of NSCLC. In the tissue classification, the central type contains about one-ninth.
Sometimes, the phrase "not otherwise specified" (NOS) is used generically, usually when a more specific diagnosis cannot be made. This is most often the case when a pathologist examines a small number of malignant cells or tissue in a cytology or biopsy specimen.[6]
Lung cancer in people who have never smoked is almost universally NSCLC, with a sizeable majority being adenocarcinoma.[7]
On relatively rare occasions, malignant lung tumors are found to contain components of both SCLC and NSCLC. In these cases, the tumors are classified as combined small-cell lung carcinoma (c-SCLC),[8] and are (usually) treated as "pure" SCLC.[9]
Lung adenocarcinoma
Adenocarcinoma of the lung is currently the most common type of lung cancer in "never smokers" (lifelong nonsmokers).[10] Adenocarcinomas account for about 40% of lung cancers. Historically, adenocarcinoma was more often seen peripherally in the lungs than SCLC and squamous-cell lung cancer, both of which tended to be more often centrally located.[11][12] Recent studies, though, suggest that the "ratio of centrally to peripherally occurring" lesions may be converging toward unity for both adenocarcinoma and squamous-cell carcinoma.
Squamous-cell lung carcinoma

Squamous-cell carcinoma (SCC) of the lung is more common in men than in women. It is closely correlated with a history of tobacco smoking, more so than most other types of lung cancer. According to the Nurses' Health Study, the relative risk of SCC is around 5.5, both among those with a previous duration of smoking of 1 to 20 years, and those with 20 to 30 years, compared to "never smokers" (lifelong nonsmokers).[13] The relative risk increases to about 16 with a previous smoking duration of 30 to 40 years, and roughly 22 with more than 40 years.[13]
Large-cell lung carcinoma
Large-cell lung carcinoma (LCLC) is a heterogeneous group of undifferentiated malignant neoplasms originating from transformed epithelial cells in the lung. LCLCs have typically comprised around 10% of all NSCLC in the past, although newer diagnostic techniques seem to be reducing the incidence of diagnosis of "classic" LCLC in favor of more poorly differentiated SCCs and adenocarcinomas.[14] LCLC is, in effect, a "diagnosis of exclusion", in that the tumor cells lack light microscopic characteristics that would classify the neoplasm as a small-cell carcinoma, squamous-cell carcinoma, adenocarcinoma, or other more specific histologic type of lung cancer. LCLC is differentiated from SCLC primarily by the larger size of the anaplastic cells, a higher cytoplasmic-to-nuclear size ratio, and a lack of "salt-and-pepper" chromatin.
Symptoms
Many of the symptoms of NSCLC can be signs of other diseases, but having chronic or overlapping symptoms may be a signal of the presence of the disease. Some symptoms are indicators of less advanced cases, while some may signal that the cancer has spread. Some of the symptoms of less advanced cancer include chronic cough, coughing up blood, hoarseness, shortness of breath, wheezing, chest pain, weight loss, and loss of appetite.[15] A few more symptoms associated with the early progression of the disease are feeling weak, being very tired, having trouble swallowing, swelling in the face or neck, and continuous or recurring infections such as bronchitis or pneumonia.[5][15][16] Signs of more advanced cases include bone pain, nervous-system changes (headache, weakness, dizziness, balance problems, seizures), jaundice, lumps near the surface of the body, numbness of extremities due to Pancoast syndrome, and nausea, vomiting, and constipation brought on by hypercalcemia.[15][16] Some more of the symptoms that indicate further progression of the cancer include shortness of breath, superior vena cava syndrome, trouble swallowing, large amounts of mucus, weakness, fatigue, and hoarseness.[16]
Cause
Smoking is by far the leading risk factor for lung cancer.[17] Cigarette smoke contains more than 6,000 components, many of which lead to DNA damage[18] (see table of tobacco-related DNA damages in Tobacco smoking).
Other causes include radon, exposure to secondhand smoke, exposure to substances such as asbestos, chromium, nickel, beryllium, soot, or tar, family history of lung cancer, and air pollution.[5][17]
Genetics can also play a role as a family history of lung cancer can contribute to an increased risk of developing the disease.[19] Furthermore, research has revealed specific chromosome regions associated with increased risks of developing lung cancer.[20] [21]
In general, DNA damage appears to be the primary underlying cause of cancer.[22] Though most DNA damages are repairable,[18] leftover unrepaired DNA damages from cigarette smoke are the likely cause of NSCLC.
DNA replication past an unrepaired damage can give rise to a mutation because of inaccurate translesion synthesis. In addition, during repair of DNA double-strand breaks, or repair of other DNA damages, incompletely cleared sites of repair can lead to epigenetic gene silencing.[23][24]
DNA repair deficiency in NSCLC
Deficiencies in DNA repair underlie many forms of cancer.[25] If DNA repair is deficient, the frequency of unrepaired DNA damages increases, and these tend to cause inaccurate translesion synthesis leading to mutation. Furthermore, increased damages can elevate incomplete repair, leading to epigenetic alterations.
As indicated as in the article Carcinogenesis, mutations in DNA repair genes occasionally occur in cancer, but deficiencies of DNA repair due to epigenetic alterations that reduce or silence DNA repair-gene expression occur much more frequently in cancer.
Epigenetic gene silencing of DNA repair genes occurs frequently in NSCLC. At least nine DNA repair genes that normally function in relatively accurate DNA repair pathways are often repressed by promoter hypermethylation in NSCLC. One DNA repair gene, FEN1, that functions in an inaccurate DNA repair pathway, is expressed at an increased level due to hypo-, rather than hyper-, methylation of its promoter region (deficiency of promoter methylation) in NSCLC.
| Gene | Frequency of hyper- (or hypo-) methylation | DNA repair pathway | Ref. |
|---|---|---|---|
| NEIL1 | 42% | base excision repair | [26] |
| WRN | 38% | homologous recombinational repair, nonhomologous end joining, base excision repair | [27] |
| MGMT | 13% - 64% | direct reversal | [26][28][29] |
| ATM | 47% | homologous recombinational repair | [30] |
| MLH1 | 48% - 73% | mismatch repair | [30][31] |
| MSH2 | 42% - 63% | mismatch repair | [30][31] |
| BRCA2 | 42% | homologous recombinational repair | [32] |
| BRCA1 | 30% | homologous recombinational repair | [32] |
| XRCC5 (Ku80) | 20% | nonhomologous end joining | [32] |
| FEN1 | 100% hypomethylated (increased expression) | microhomology-mediated end joining | [33] |
The frequent deficiencies in accurate DNA repair, and the increase in inaccurate repair, likely cause the high level of mutation in lung cancer cells of more than 100,000 mutations per genome (see Whole genome sequencing).
Staging
Staging is a formal procedure to determine how developed the cancer is, which determines treatment options.
The American Joint Committee on Cancer and the International Union Against Cancer recommend TNM staging, using a uniform scheme for NSCLC, SCLC, and bronchopulmonary carcinoid tumors.[34] With TNM staging, the cancer is classified based on the size of the tumor and spread to lymph nodes and other organs. As the tumor grows in size and the areas affected become larger, the staging of the cancer becomes more advanced as well.
Several components of NSCLC staging then influence physicians' treatment strategies.[35] The lung tumor itself is typically assessed both radiographically for overall size and by a pathologist under the microscope to identify specific genetic markers or to see if invasion into important structures within the chest (e.g., bronchus or pleural cavity) has occurred. Next, the patient's nearby lymph nodes within the chest cavity, known as the mediastinum, are checked for disease involvement. Finally, the patient is evaluated for more distant sites of metastatic disease, most typically with brain imaging and or scans of the bones.[36]
Five-year survival rates
The survival rates for stages I through IV decrease significantly due to the advancement of the disease. For stage I, the five-year survival rate is 47%, stage II is 30%, stage III is 10%, and stage IV is 1%.[37]
Treatment
More than one kind of treatment is often used, depending on the stage of the cancer, the individual's overall health, age, response to chemotherapy, and other factors such as the likely side effects of the treatment. After full staging, the NSCLC patient can typically be classified in one of three different categories: patients with early, nonmetastatic disease (stages I and II, and select type III tumors), patients with locally advanced disease confined to the thoracic cavity (e.g., large tumors, tumors involving critical chest structures, or patients with positive mediastinal lymph nodes), or patients with distant metastasis outside of the thoracic cavity.
Early/nonmetastatic NSCLC
NSCLCs are usually not very sensitive to chemotherapy[38] and/or radiation, so surgery (lung resection to remove the tumor) remains the treatment of choice if patients are diagnosed at an early stage.[39]
If the persons have a small, but inoperable tumor, they may undergo highly targeted, high-intensity radiation therapy. New methods of giving radiation treatment allow doctors to be more accurate in treating lung cancers. This means less radiation affects nearby healthy tissues. New methods include Cyberknife and stereotactic body radiation therapy. Certain people who are deemed to be higher risk may also receive adjuvant (ancillary) chemotherapy after initial surgery or radiation therapy. A number of possible chemotherapy agents can be selected, but most involve the platinum-based chemotherapy drug called cisplatin.
Other treatments include percutaneous ablation and chemoembolization.[40] The most widely used ablation techniques for lung cancer are radiofrequency ablation (RFA), cryoablation, and microwave ablation.[41] Ablation may be an option for patients whose tumors are near the outer edge of the lungs. Nodules less than 1 cm from the trachea, main bronchi, oesophagus, and central vessels should be excluded from RFA given high risk of complications and frequent incomplete ablation. Additionally, lesions greater than 5 cm should be excluded and lesions 3 to 5 cm should be considered with caution given high risk of recurrence.[42] As a minimally invasive procedure, it can be a safer alternative for patients who are poor candidates for surgery due to comorbidities or limited lung function. A study comparing thermal ablation to sublobar resection as treatment for early stage NSCLC in older people found no difference in overall survival of the patients.[43] It is possible that RFA followed by radiation therapy has a survival benefit due to synergism of the two mechanisms of cell destruction.[44]
Advanced/metastatic NSCLC
The treatment approach for people who have advanced NSCLC is first aimed at relieving pain and distress (palliative), but a wide variety of chemotherapy options exists.[45][46] These agents include both traditional chemotherapies, such as cisplatin, which indiscriminately target all rapidly dividing cells, and newer targeted agents, which are more tailored to specific genetic aberrations found within a person's tumor.[46] When choosing an appropriate chemotherapy approach, the toxicity profile (side effects of the drug) should be taken into account and balanced with the person's comorbidities (other conditions or side effects that the person is experiencing).[46] Carboplatin is a chemotherapy agent that has a similar effect on a person's survival when compared to cisplatin, and has a different toxicity profile from cisplatin.[46] Carboplatin may be associated with a higher risk of thrombocytopenia. Cisplatin may cause more nausea or vomiting when compared to carboplatin treatment.[46]
At present, two genetic markers are routinely profiled in NSCLC tumors to guide further treatment decision-making - mutations within epidermal growth factor (EGFR) and anaplastic lymphoma kinase.[47] Also, a number of additional genetic markers are known to be mutated within NSCLC and may impact treatment in the future, including BRAF, HER2/neu, and KRAS. For advanced NSCLC, a combined chemotherapy treatment approach that includes cetuximab, an antibody that targets the EGFR signalling pathway, is more effective at improving a person's overall survival when compared to standard chemotherapy alone.[48]
Thermal ablations, i.e. RFA, cryoablation, and microwave ablation, are appropriate for palliative treatment of tumor-related symptoms or recurrences within treatment fields. People with severe pulmonary fibrosis and severe emphysema with a life expectancy less than a year should be considered poor candidates for this treatment.[41]
EGFR mutations
Roughly 10–35% of people who have NSCLC will have drug-sensitizing mutations of the EGFR.[47] The distribution of these mutations has been found to be race-dependent, with one study estimating that 10% of Caucasians, but 50% of Asians, will be found to have such tumor markers.[49] A number of different EGFR mutations have been discovered, but certain aberrations result in hyperactive forms of the protein. People with these mutations are more likely to have adenocarcinoma histology and be nonsmokers or light smokers. These people have been shown to be sensitized to certain medications that block the EGFR protein known as tyrosine kinase inhibitors specifically, erlotinib, gefitinib, afatinib, or osimertinib.[50] Reliable identification of mutations in lung cancer needs careful consideration due to the variable sensitivity of diagnostic techniques.[51]
ALK gene rearrangements
Up to 7% of NSCLC patients have EML4-ALK translocations or mutations in the ROS1 gene; these patients may benefit from ALK inhibitors, which are now approved for this subset of patients.[52] Crizotinib, which gained FDA approval in August 2011, is an inhibitor of several kinases, specifically ALK, ROS1, and MET. Crizotinib has been shown in clinical studies to have response rates around 60% if patients are shown to have ALK-positive disease.[39] Several studies have also shown that ALK mutations and EGFR activating mutations are typically mutually exclusive. Thus, patients who fail crizotinib are not recommended to be switched to an EGFR-targeted drug such as erlotinib.[39]
Other treatment options
NSCLC patients with advanced disease who are not found to have either EGFR or ALK mutations may receive bevacizumab, which is a monoclonal antibody medication targeted against the vascular endothelial growth factor (VEGF). This is based on an Eastern Cooperative Oncology Group study that found that adding bevacizumab to carboplatin and paclitaxel chemotherapy for certain patients with recurrent or advanced NSCLC (stage IIIB or IV) may increase both overall survival and progression-free survival.[53]


NSCLC cells expressing programmed death-ligand 1 (PD-L1) could interact with programmed death receptor 1 (PD-1) expressed on the surface of T cells, and result in decreased tumor cell kill by the immune system. Atezolizumab is an anti PD-L1 monoclonal antibody. Nivolumab and Pembrolizumab are anti PD-1 monoclonal antibodies. Ipilimumab is a monoclonal antibody that targets Cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) on the surface of T cells. Bevacizumab is a monoclonal antibody that targets Vascular Endothelial Growth Factor (VEGF) in the circulation and functions as an angiogenesis inhibitor. Multiple phase 3 clinical trials utilizing immunotherapy in the first line for treatment of NSCLC were published, including Pembrolizumab in KEYNOTE-024, KEYNOTE-042, KEYNOTE-189 and KEYNOTE-407; Nivolumab and Ipilimumab in CHECKMATE-227 and CHECKMATE 9LA; and Atezolizumab in IMpower110, IMpower130 and IMpower150.[54]
In 2015, the US Food and Drug Administration (FDA) approved the anti-PD-1 agent nivolumab for advanced or metastatic SCC.
In 2015, FDA also approved the anti-EGFR drug necitumumab for metastatic SCC.
2 October 2015, the FDA approved pembrolizumab for the treatment of metastatic NSCLC in patients whose tumors express PD-L1 and who have failed treatment with other chemotherapeutic agents.
October 2016, pembrolizumab became the first immunotherapy to be used first line in the treatment of NSCLC if the cancer overexpresses PDL1 and the cancer has no mutations in EGFR or in ALK; if chemotherapy has already been administered, then pembrolizumab can be used as a second-line treatment, but if the cancer has EGFR or ALK mutations, agents targeting those mutations should be used first. Assessment of PDL1 must be conducted with a validated and approved companion diagnostic.

The prognosis of patients with non-small-cell lung cancer improved significantly with the introduction of immunotherapy.[54] People with tumor PDL-1 expressed over half or more of the tumor cells achieved a median overall survival of 30 months with pembrolizumab.[55][56]
Mobocertinib (Exkivity) was approved for medical use in the United States in September 2021, and it is indicated for adults with locally advanced or metastatic non-small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 20 insertion mutations, as detected by an FDA-approved test, whose disease has progressed on or after platinum-based chemotherapy.[57][58]
References
- Khajuria, Ocean; Sharma, Neha (1 December 2021). "Epigenetic targeting for lung cancer treatment via CRISPR/Cas9 technology". Advances in Cancer Biology - Metastasis. 3: 100012. doi:10.1016/j.adcanc.2021.100012. ISSN 2667-3940.
- Non-Small Cell Lung Cancer at eMedicine
- "What Is Non-Small Cell Lung Cancer?". www.cancer.org.
- Smokers defined as current or former smoker of more than 1 year of duration. See image page in Commons for percentages in numbers. Reference: Table 2 in: Kenfield SA, Wei EK, Stampfer MJ, Rosner BA, Colditz GA (June 2008). "Comparison of aspects of smoking among the four histological types of lung cancer". Tobacco Control. 17 (3): 198–204. doi:10.1136/tc.2007.022582. PMC 3044470. PMID 18390646.
- "Non-Small Cell Lung Cancer Treatment". National Cancer Institute. 1 January 1980. Retrieved 4 December 2017.
- "Non-small cell lung cancer treatment – National Cancer Institute". 1 January 1980. Retrieved 19 October 2008.
- Hanna N (2007). "Lung Cancer in the Never Smoker Population". Hematology-Oncology. Medscape.
- Travis WD, Brambilla E, Muller-Hermelink HK, et al., eds. (2004). Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart (PDF). World Health Organization Classification of Tumours. Lyon: IARC Press. ISBN 978-92-832-2418-1. Archived from the original (PDF) on 23 August 2009. Retrieved 27 March 2010.
- Simon GR, Turrisi A (September 2007). "Management of small cell lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition)". Chest. 132 (3 Suppl): 324S–339S. doi:10.1378/chest.07-1385. PMID 17873178. Archived from the original on 12 January 2013.
- Subramanian J, Govindan R (February 2007). "Lung cancer in never smokers: a review". Journal of Clinical Oncology. 25 (5): 561–70. doi:10.1200/JCO.2006.06.8015. PMID 17290066.
- Mitchell RS, Kumar V, Abbas AK, Fausto N (2007). "morphology of adenocarcinoma". Robbins Basic Pathology (8th ed.). Philadelphia: Saunders. ISBN 978-1-4160-2973-1.
- Travis WD, Travis LB, Devesa SS (January 1995). "Lung cancer". Cancer. 75 (1 Suppl): 191–202. doi:10.1002/1097-0142(19950101)75:1+<191::AID-CNCR2820751307>3.0.CO;2-Y. PMID 8000996. S2CID 221577784.
- Kenfield SA, Wei EK, Stampfer MJ, Rosner BA, Colditz GA (June 2008). "Comparison of aspects of smoking among the four histological types of lung cancer". Tobacco Control. 17 (3): 198–204. doi:10.1136/tc.2007.022582. PMC 3044470. PMID 18390646.
- Popper HH (2011). "Large cell carcinoma of the lung – a vanishing entity?". Memo - Magazine of European Medical Oncology. 4: 4–9. doi:10.1007/s12254-011-0245-8. S2CID 71238993.
- "Non-Small Cell Lung Cancer Signs and Symptoms". www.cancer.org. Retrieved 4 December 2017.
- "Non-small cell lung cancer". University of Maryland Medical Center. Retrieved 4 December 2017.
- "Non-Small Cell Lung Cancer Risk Factors". www.cancer.org.
- Liu X, Conner H, Kobayashi T, Kim H, Wen F, Abe S, et al. (August 2005). "Cigarette smoke extract induces DNA damage but not apoptosis in human bronchial epithelial cells". American Journal of Respiratory Cell and Molecular Biology. 33 (2): 121–9. doi:10.1165/rcmb.2003-0341OC. PMID 15845867.
- Khajuria, Ocean; Sharma, Neha (1 December 2021). "Epigenetic targeting for lung cancer treatment via CRISPR/Cas9 technology". Advances in Cancer Biology - Metastasis. 3: 100012. doi:10.1016/j.adcanc.2021.100012. ISSN 2667-3940.
- Khajuria, Ocean; Sharma, Neha (1 December 2021). "Epigenetic targeting for lung cancer treatment via CRISPR/Cas9 technology". Advances in Cancer Biology - Metastasis. 3: 100012. doi:10.1016/j.adcanc.2021.100012. ISSN 2667-3940.
- Herbst, Roy S.; Heymach, John V.; Lippman, Scott M. (25 September 2008). "Lung Cancer". New England Journal of Medicine. 359 (13): 1367–1380. doi:10.1056/NEJMra0802714. ISSN 0028-4793. PMID 18815398.
- Kastan MB (April 2008). "DNA damage responses: mechanisms and roles in human disease: 2007 G.H.A. Clowes Memorial Award Lecture". Molecular Cancer Research. 6 (4): 517–24. doi:10.1158/1541-7786.MCR-08-0020. PMID 18403632.
- O'Hagan HM, Mohammad HP, Baylin SB (August 2008). Lee JT (ed.). "Double strand breaks can initiate gene silencing and SIRT1-dependent onset of DNA methylation in an exogenous promoter CpG island". PLOS Genetics. 4 (8): e1000155. doi:10.1371/journal.pgen.1000155. PMC 2491723. PMID 18704159.
- Cuozzo C, Porcellini A, Angrisano T, Morano A, Lee B, Di Pardo A, et al. (July 2007). "DNA damage, homology-directed repair, and DNA methylation". PLOS Genetics. 3 (7): e110. doi:10.1371/journal.pgen.0030110. PMC 1913100. PMID 17616978.
- Harper JW, Elledge SJ (December 2007). "The DNA damage response: ten years after". Molecular Cell. 28 (5): 739–45. doi:10.1016/j.molcel.2007.11.015. PMID 18082599.
- Do H, Wong NC, Murone C, John T, Solomon B, Mitchell PL, Dobrovic A (February 2014). "A critical re-assessment of DNA repair gene promoter methylation in non-small cell lung carcinoma". Scientific Reports. 4: 4186. Bibcode:2014NatSR...4E4186D. doi:10.1038/srep04186. PMC 3935198. PMID 24569633.
- Agrelo R, Cheng WH, Setien F, Ropero S, Espada J, Fraga MF, et al. (June 2006). "Epigenetic inactivation of the premature aging Werner syndrome gene in human cancer". Proceedings of the National Academy of Sciences of the United States of America. 103 (23): 8822–7. Bibcode:2006PNAS..103.8822A. doi:10.1073/pnas.0600645103. PMC 1466544. PMID 16723399.
- Wolf P, Hu YC, Doffek K, Sidransky D, Ahrendt SA (November 2001). "O(6)-Methylguanine-DNA methyltransferase promoter hypermethylation shifts the p53 mutational spectrum in non-small cell lung cancer". Cancer Research. 61 (22): 8113–7. PMID 11719438.
- Ekim M, Caner V, Büyükpınarbaşılı N, Tepeli E, Elmas L, Bağcı G (May 2011). "Determination of O6-methylguanine DNA methyltransferase promoter methylation in non-small cell lung cancer". Genetic Testing and Molecular Biomarkers. 15 (5): 357–60. doi:10.1089/gtmb.2010.0211. PMID 21288129.
- Safar AM, Spencer H, Su X, Coffey M, Cooney CA, Ratnasinghe LD, et al. (June 2005). "Methylation profiling of archived non-small cell lung cancer: a promising prognostic system". Clinical Cancer Research. 11 (12): 4400–5. doi:10.1158/1078-0432.CCR-04-2378. PMID 15958624.
- Gomes A, Reis-Silva M, Alarcão A, Couceiro P, Sousa V, Carvalho L (2014). "Promoter hypermethylation of DNA repair genes MLH1 and MSH2 in adenocarcinomas and squamous cell carcinomas of the lung". Revista Portuguesa de Pneumologia. 20 (1): 20–30. doi:10.1016/j.rppneu.2013.07.003. PMID 24360395.
- Lee MN, Tseng RC, Hsu HS, Chen JY, Tzao C, Ho WL, Wang YC (February 2007). "Epigenetic inactivation of the chromosomal stability control genes BRCA1, BRCA2, and XRCC5 in non-small cell lung cancer". Clinical Cancer Research. 13 (3): 832–8. doi:10.1158/1078-0432.CCR-05-2694. PMID 17289874.
- Nikolova T, Christmann M, Kaina B (July 2009). "FEN1 is overexpressed in testis, lung and brain tumors". Anticancer Research. 29 (7): 2453–9. PMID 19596913.
- "Cancer Staging Posters: Lung" (PDF). AJCC Cancer Staging (7th ed.). 2009. Archived from the original (PDF) on 28 September 2011.
- "National Cancer Institute Non-Small Cell Lung Cancer Treatment (PDQ)". 1 January 1980. Retrieved 12 May 2015.
- Chawla M, Kumar R, Agarwala S, Bakhshi S, Gupta DK, Malhotra A (October 2010). "Role of positron emission tomography-computed tomography in staging and early chemotherapy response evaluation in children with neuroblastoma". Indian Journal of Nuclear Medicine. 25 (4): 147–55. doi:10.4103/0972-3919.78249 (inactive 31 July 2022). PMC 3109821. PMID 21713223.
{{cite journal}}: CS1 maint: DOI inactive as of July 2022 (link) - "Non-Small Cell Lung Cancer Survival Rates, by Stage". www.cancer.org. Retrieved 4 December 2017.
- Cotran RS, Kumar V, Fausto N, Robbins SL, Abbas AK (2005). Robbins and Cotran pathologic basis of disease. St. Louis MO: Elsevier Saunders. p. 759. ISBN 978-0-7216-0187-8.
- "NCCN Clinical Practice Guidelines for NSCLC" (PDF). Retrieved 12 May 2015.
- "Chemoembolisation". Cancer Research UK. 30 August 2017. Archived from the original on 9 October 2007.
- Dupuy DE, Shulman M (September 2010). "Current status of thermal ablation treatments for lung malignancies". Seminars in Interventional Radiology. 27 (3): 268–75. doi:10.1055/s-0030-1261785. PMC 3324195. PMID 22550366.
- Bargellini I, Bozzi E, Cioni R, Parentini B, Bartolozzi C (October 2011). "Radiofrequency ablation of lung tumours". Insights into Imaging. 2 (5): 567–576. doi:10.1007/s13244-011-0110-7. PMC 3259330. PMID 22347976.
- Kwan SW, Mortell KE, Talenfeld AD, Brunner MC (January 2014). "Thermal ablation matches sublobar resection outcomes in older patients with early-stage non-small cell lung cancer". Journal of Vascular and Interventional Radiology. 25 (1): 1–9.e1. doi:10.1016/j.jvir.2013.10.018. PMID 24365502.
- Grieco CA, Simon CJ, Mayo-Smith WW, DiPetrillo TA, Ready NE, Dupuy DE (July 2006). "Percutaneous image-guided thermal ablation and radiation therapy: outcomes of combined treatment for 41 patients with inoperable stage I/II non-small-cell lung cancer". Journal of Vascular and Interventional Radiology. 17 (7): 1117–24. doi:10.1097/01.RVI.0000228373.58498.6E. PMID 16868164.
- "Lung Cancer online". lungcanceronline.org. Archived from the original on 17 June 2008. Retrieved 13 December 2008.
- Vasconcellos, Vitor F.; Marta, Guilherme N.; da Silva, Edina Mk; Gois, Aecio Ft; de Castria, Tiago B.; Riera, Rachel (13 January 2020). "Cisplatin versus carboplatin in combination with third-generation drugs for advanced non-small cell lung cancer". The Cochrane Database of Systematic Reviews. 1: CD009256. doi:10.1002/14651858.CD009256.pub3. ISSN 1469-493X. PMC 6956680. PMID 31930743.
- "Molecular Profiling of Lung Cancer". Retrieved 12 May 2015.
- Yang ZY, Liu L, Mao C, Wu XY, Huang YF, Hu XF, Tang JL (November 2014). "Chemotherapy with cetuximab versus chemotherapy alone for chemotherapy-naive advanced non-small cell lung cancer". The Cochrane Database of Systematic Reviews (11): CD009948. doi:10.1002/14651858.CD009948.pub2. PMID 25400254.
- Hirsch FR, Bunn PA (May 2009). "EGFR testing in lung cancer is ready for prime time". The Lancet. Oncology. 10 (5): 432–3. doi:10.1016/s1470-2045(09)70110-x. PMID 19410185.
- Kris MG (October 2005). "How today's developments in the treatment of non-small cell lung cancer will change tomorrow's standards of care". The Oncologist. 10 Suppl 2 (Suppl 2): 23–9. doi:10.1634/theoncologist.10-90002-23. PMID 16272456. Archived from the original on 22 August 2009.
- Sherwood J, Dearden S, Ratcliffe M, Walker J (September 2015). "Mutation status concordance between primary lesions and metastatic sites of advanced non-small-cell lung cancer and the impact of mutation testing methodologies: a literature review". Journal of Experimental & Clinical Cancer Research. 34 (1): 92. doi:10.1186/s13046-015-0207-9. PMC 4559261. PMID 26338018.
- Farmer (2010). "Non-Small-Cell Lung Cancer Standards of Care Challenged by a Cornucopia of New Drugs".
- Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, et al. (December 2006). "Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer". The New England Journal of Medicine. 355 (24): 2542–50. doi:10.1056/nejmoa061884. PMID 17167137.
- Nasser, Nicola J.; Gorenberg, Miguel; Agbarya, Abed (2020). "First line Immunotherapy for Non-Small Cell Lung Cancer". Pharmaceuticals. 13 (11): 373. doi:10.3390/ph13110373. PMC 7695295. PMID 33171686.
 Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License.
Text was copied from this source, which is available under a Creative Commons Attribution 4.0 International License. - Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. (November 2016). "Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer". The New England Journal of Medicine. 375 (19): 1823–1833. doi:10.1056/NEJMoa1606774. PMID 27718847.
- Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, et al. (March 2019). "Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With PD-L1 Tumor Proportion Score of 50% or Greater". Journal of Clinical Oncology. 37 (7): 537–546. doi:10.1200/JCO.18.00149. PMID 30620668. S2CID 58640902.
- "FDA grants accelerated approval to mobocertinib for metastatic non-sma". U.S. Food and Drug Administration (FDA). 16 September 2021. Retrieved 16 September 2021.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - "Takeda's Exkivity (mobocertinib) Approved by U.S. FDA as the First Oral Therapy Specifically Designed for Patients with EGFR Exon20 Insertion+ NSCLC" (Press release). Takeda. 15 September 2021. Retrieved 16 September 2021 – via Business Wire.
{kind=link}
External links
- MedlinePlus Encyclopedia: Lung cancer — non-small cell