


Amebiasis
 ShareCompartir
ShareCompartir
[Entamoeba histolytica]
Causal Agents
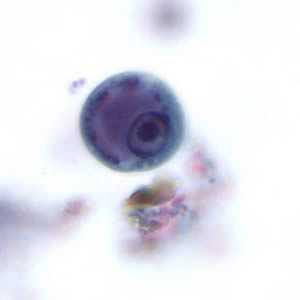
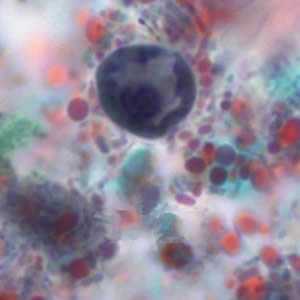
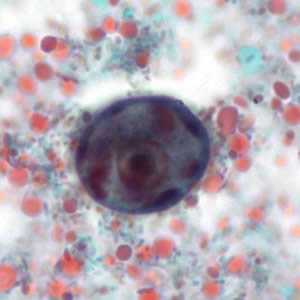
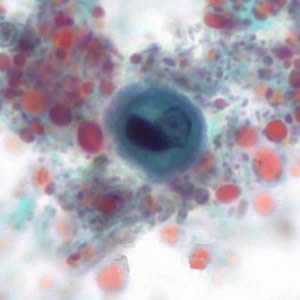
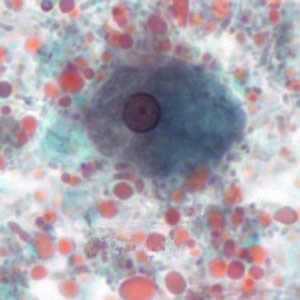
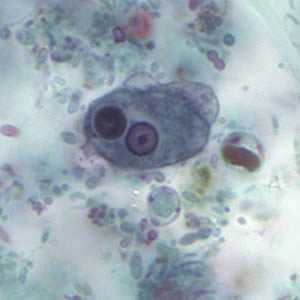
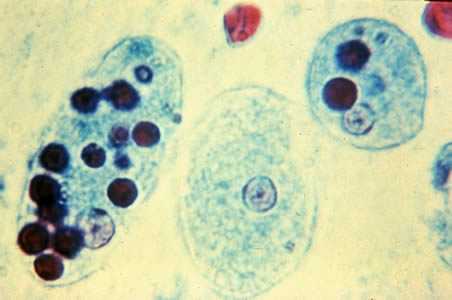
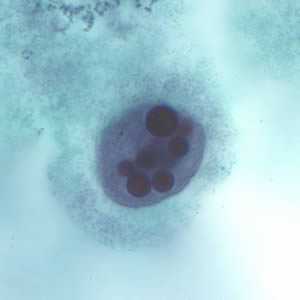
Several protozoan species in the genus Entamoeba colonize humans, but not all of them are associated with disease. Entamoeba histolytica is well recognized as a pathogenic ameba, associated with intestinal and extraintestinal infections. The other species are important because they may be confused with E. histolytica in diagnostic investigations.
Life Cycle

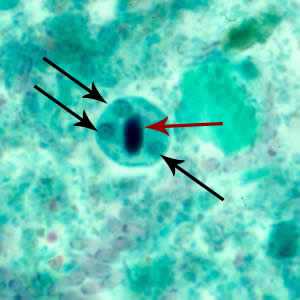
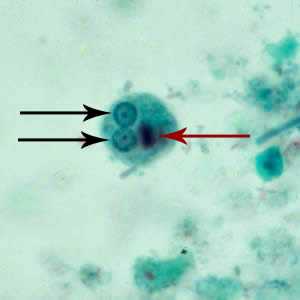
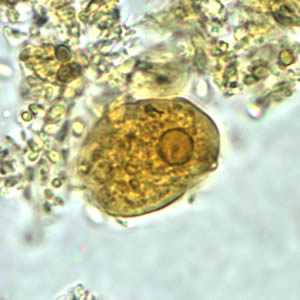
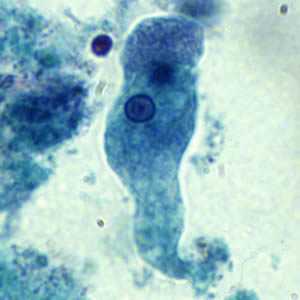
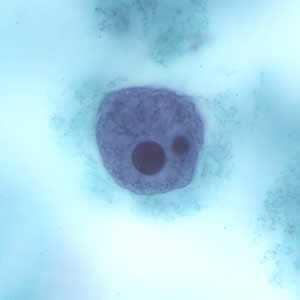
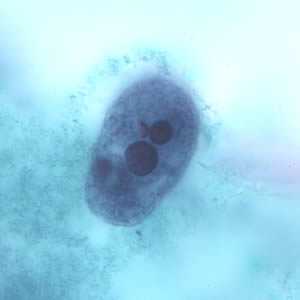
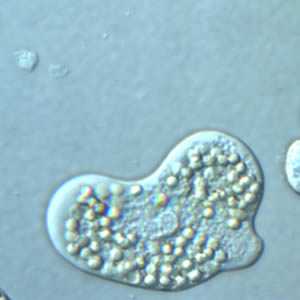
Cysts and trophozoites are passed in feces  . Cysts are typically found in formed stool, whereas trophozoites are typically found in diarrheal stool. Infection by Entamoeba histolytica occurs by ingestion of mature cysts
. Cysts are typically found in formed stool, whereas trophozoites are typically found in diarrheal stool. Infection by Entamoeba histolytica occurs by ingestion of mature cysts  in fecally contaminated food, water, or hands. Excystation
in fecally contaminated food, water, or hands. Excystation  occurs in the small intestine and trophozoites
occurs in the small intestine and trophozoites  are released, which migrate to the large intestine. The trophozoites multiply by binary fission and produce cysts
are released, which migrate to the large intestine. The trophozoites multiply by binary fission and produce cysts  , and both stages are passed in the feces . Because of the protection conferred by their walls, the cysts can survive days to weeks in the external environment and are responsible for transmission. Trophozoites passed in the stool are rapidly destroyed once outside the body, and if ingested would not survive exposure to the gastric environment. In many cases, the trophozoites remain confined to the intestinal lumen (
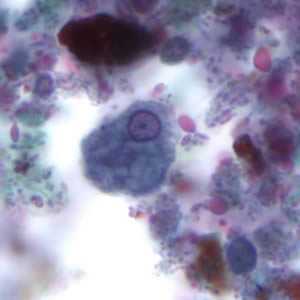
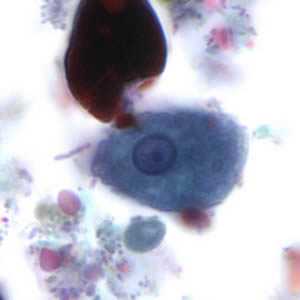
, and both stages are passed in the feces . Because of the protection conferred by their walls, the cysts can survive days to weeks in the external environment and are responsible for transmission. Trophozoites passed in the stool are rapidly destroyed once outside the body, and if ingested would not survive exposure to the gastric environment. In many cases, the trophozoites remain confined to the intestinal lumen ( : noninvasive infection) of individuals who are asymptomatic carriers, passing cysts in their stool. In some patients the trophozoites invade the intestinal mucosa (
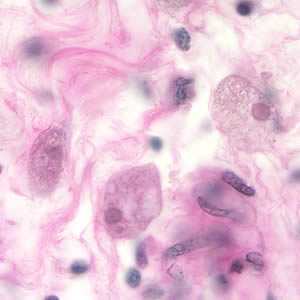
: noninvasive infection) of individuals who are asymptomatic carriers, passing cysts in their stool. In some patients the trophozoites invade the intestinal mucosa ( : intestinal disease), or, through the bloodstream, extraintestinal sites such as the liver, brain, and lungs (
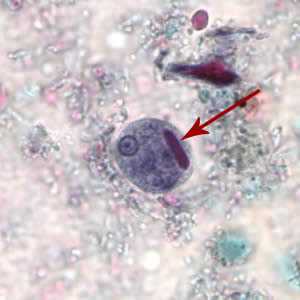
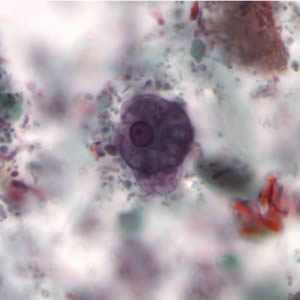
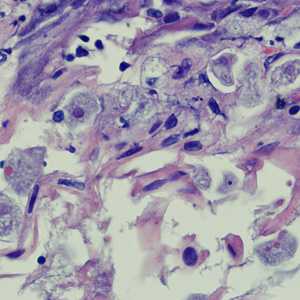
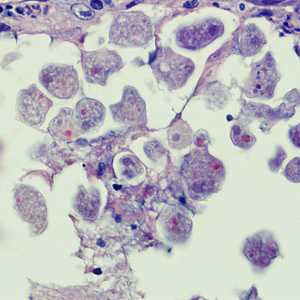
: intestinal disease), or, through the bloodstream, extraintestinal sites such as the liver, brain, and lungs ( : extraintestinal disease), with resultant pathologic manifestations. It has been established that the invasive and noninvasive forms represent two separate species, respectively E. histolytica and E. dispar. These two species are morphologically indistinguishable unless E. histolytica is observed with ingested red blood cells (erythrophagocystosis). Transmission can also occur through exposure to fecal matter during sexual contact (in which case not only cysts, but also trophozoites could prove infective).
: extraintestinal disease), with resultant pathologic manifestations. It has been established that the invasive and noninvasive forms represent two separate species, respectively E. histolytica and E. dispar. These two species are morphologically indistinguishable unless E. histolytica is observed with ingested red blood cells (erythrophagocystosis). Transmission can also occur through exposure to fecal matter during sexual contact (in which case not only cysts, but also trophozoites could prove infective).
Geographic Distribution
Worldwide, with higher incidence of amebiasis in developing countries. In industrialized countries, risk groups include male homosexuals, travelers and recent immigrants, and institutionalized populations.
Clinical Presentation
A wide spectrum, from asymptomatic infection ("luminal amebiasis"), to invasive intestinal amebiasis (dysentery, colitis, appendicitis, toxic megacolon, amebomas), to invasive extraintestinal amebiasis (liver abscess, peritonitis, pleuropulmonary abscess, cutaneous and genital amebic lesions).






 Laboratory Diagnosis of Amebiasis -- Entamoeba histolytica and Entamoeba dispar
Laboratory Diagnosis of Amebiasis -- Entamoeba histolytica and Entamoeba disparDPDx is an education resource designed for health professionals and laboratory scientists. For an overview including prevention and control visit www.cdc.gov/parasites/.
- Page last reviewed: May 3, 2016
- Page last updated: May 3, 2016
- Content source:
- Global Health – Division of Parasitic Diseases and Malaria
- Notice: Linking to a non-federal site does not constitute an endorsement by HHS, CDC or any of its employees of the sponsors or the information and products presented on the site.
- Maintained By: