

Prescription Cholesterol-lowering Medication Use in Adults Aged 40 and Over: United States, 2003–2012
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 177, December 2014
On This Page
- Key findings
- What were the trends in prescription cholesterol-lowering medication use in the United States?
- What were the most commonly used prescription cholesterol-lowering medications?
- Did prescription cholesterol-lowering medication use vary by demographic subgroups?
- What percentage of adults with a selected medical condition used a prescription cholesterol-lowering medication?
- Did use of a prescription cholesterol-lowering medication vary among adults aged 40–64 with and without health insurance coverage?
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (682 KB)
Qiuping Gu, M.D., Ph.D.; Ryne Paulose-Ram, Ph.D., M.A.; Vicki L. Burt, Sc.M., R.N.; and Brian K. Kit, M.D., M.P.H.
Key findings
Data from the National Health and Nutrition Examination Survey
- During 2003–2012, the percentage of adults aged 40 and over using a cholesterol-lowering medication in the past 30 days increased from 20% to 28%.
- The use of statins increased from 18% to 26%. By 2011–2012, 93% of adults using a cholesterol-lowering medication used a statin.
- Cholesterol-lowering medication use increased with age, from 17% of adults aged 40–59 to 48% of adults aged 75 and over.
- About 71% of adults with cardiovascular disease and 54% of adults with hypercholesterolemia used a cholesterol-lowering medication.
- Adults aged 40–64 with health insurance were more likely than those without health insurance to use a cholesterol-lowering medication.
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality in the United States. Nearly one in three Americans dies of heart disease or stroke (1). Elevated blood cholesterol is a major risk factor for CVD, and statin therapy has been strongly associated with a reduced risk of atherosclerotic CVD (2,3). The national cholesterol treatment guidelines outline the importance of using cholesterol-lowering medications for the prevention of coronary heart disease (4). Using National Health and Nutrition Examination Survey (NHANES) data, this report evaluates recent trends in prescription cholesterol-lowering medication use among U.S. adults aged 40 and over.
Keywords: prevalence, statins, trends, NHANES
What were the trends in prescription cholesterol-lowering medication use in the United States?
During 2011–2012, more than one-quarter (27.9%) of adults aged 40 and over reported using a prescription cholesterol-lowering medication in the past 30 days. This was an increase from 2003–2004, when one in five adults used a cholesterol-lowering medication (19.9%) (Figure 1).
Figure 1. Percentage of adults aged 40 and over who reported using a prescription cholesterol-lowering medication: United States, 2003–2012
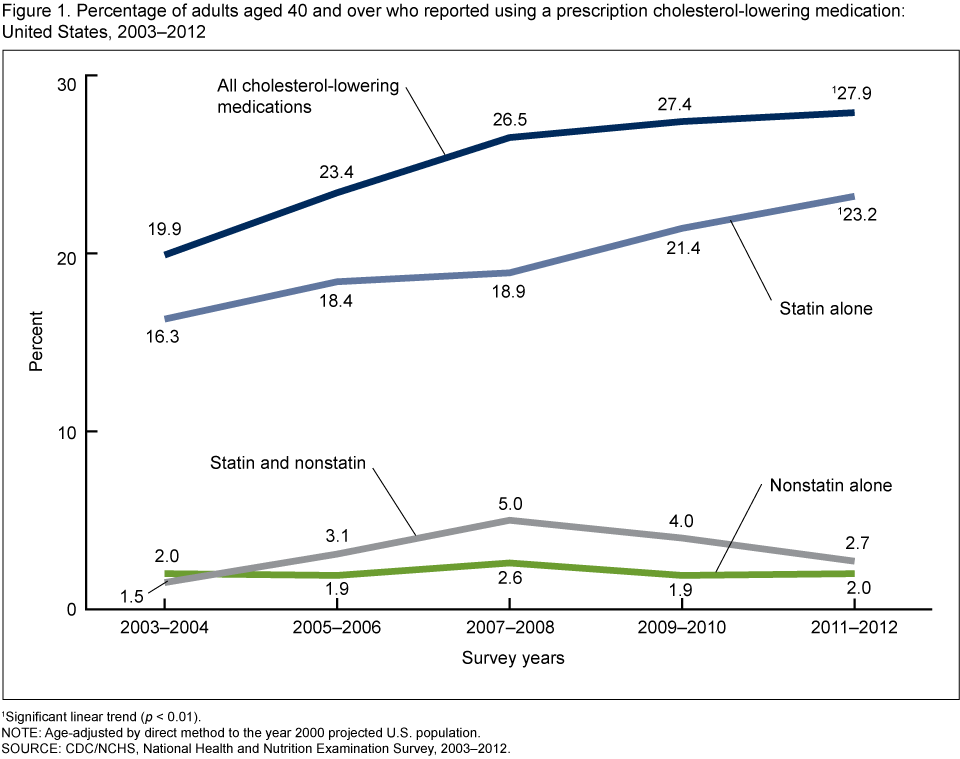
1Significant linear trend (p < 0.01).
NOTE: Age-adjusted by direct method to the year 2000 projected U.S. population.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2003–2012.
For 2011–2012, 83% of adults who used a cholesterol-lowering medication reported using a statin alone, 10% used both a statin and a nonstatin, and 7% used only a nonstatin. The percentage of adults who used a statin alone increased from 16.3% in 2003–2004 to 23.2% in 2011–2012.
What were the most commonly used prescription cholesterol-lowering medications?
Among adults who used a prescription cholesterol-lowering medication, simvastatin was the most commonly used cholesterol-lowering medication, with 42% reporting its use. This was followed by atorvastatin (20.2%), pravastatin (11.2%), rosuvastatin (8.2%), and lovastatin (7.4%) (Figure 2).
Figure 2. Percentage of adults aged 40 and over using each specific medication among those who reported using a cholesterol-lowering medication in the past 30 days: United States, 2011–2012
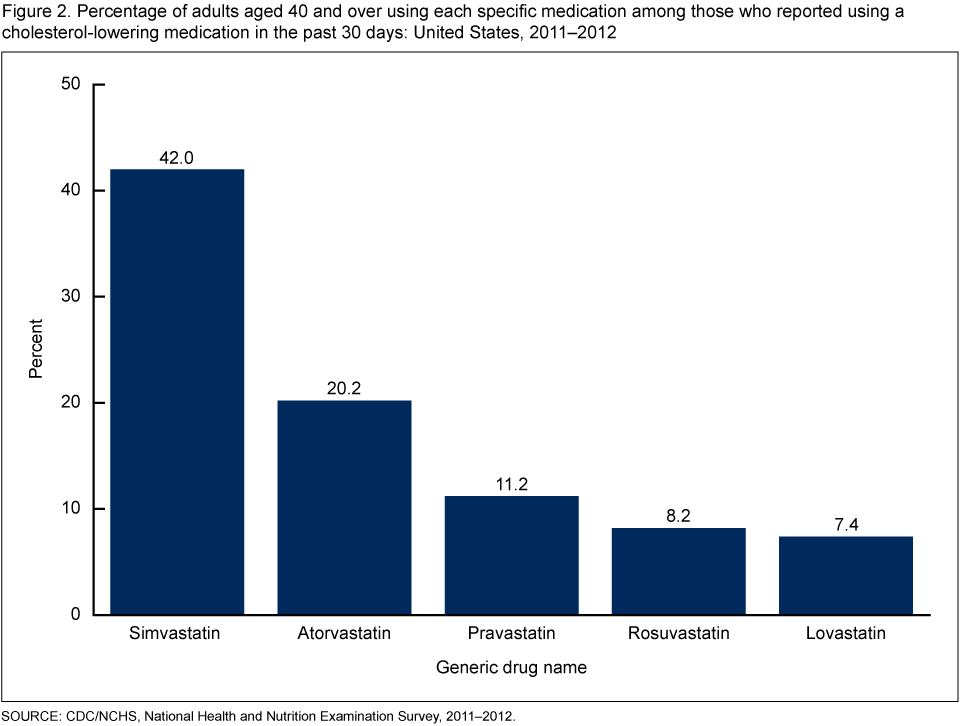
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012.
Did prescription cholesterol-lowering medication use vary by demographic subgroups?
Prescription cholesterol-lowering medication use increased with age, from 17.4% in adults aged 40–59 to 43.3% in adults aged 60–74 and 47.6% in adults aged 75 and over. There was no significant difference between men (30.1%) and women (26.2%) or any race and Hispanic origin groups (24.1%–28.9%) in the percentage that used a prescription cholesterol-lowering medication (Figure 3).
Figure 3. Percentage of adults aged 40 and over who used a prescription cholesterol-lowering medication in the past 30 days, by age, sex, and race and Hispanic origin: United States, 2011–2012
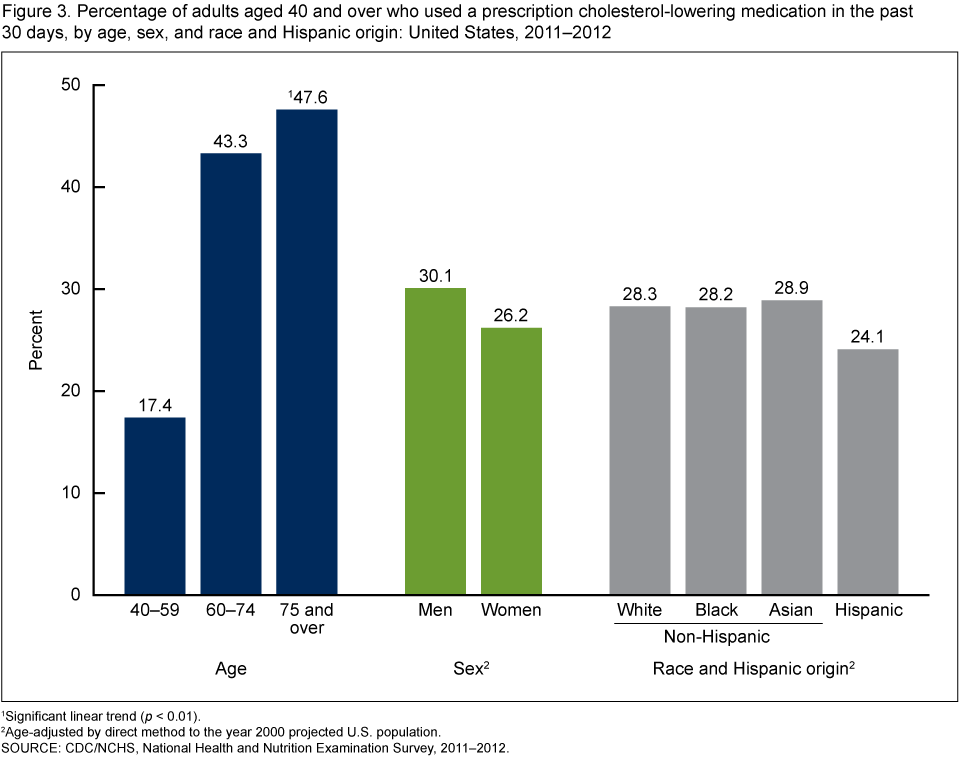
1Significant linear trend (p < 0.01).
2Age-adjusted by direct method to the year 2000 projected U.S. population.
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012.
What percentage of adults with a selected medical condition used a prescription cholesterol-
lowering medication?
Slightly more than 70% of adults with doctor-diagnosed CVD reported taking prescription cholesterol-lowering medication in the past 30 days. Nearly 63% of adults with diagnosed diabetes and nearly 54% of adults with diagnosed hypercholesterolemia reported using a prescription cholesterol-lowering medication (Figure 4).
Figure 4. Percentage of adults aged 40 and over who used a prescription cholesterol-lowering medication in the past 30 days, by selected medical conditions: United States, 2011–2012
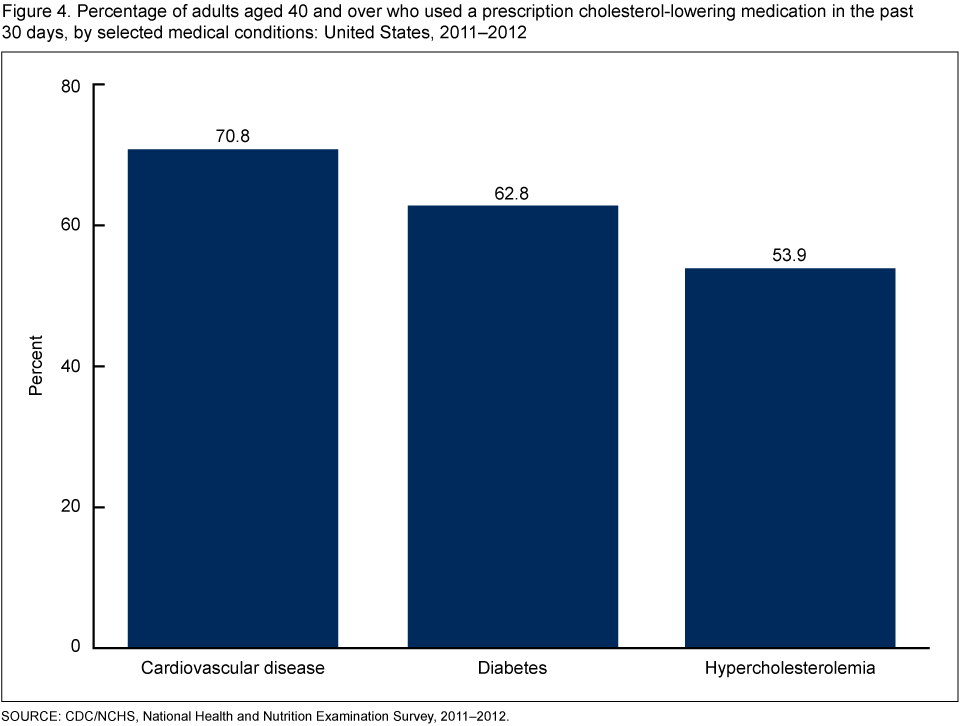
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012.
Did use of a prescription cholesterol-lowering medication vary among adults aged 40–64 with and without health insurance coverage?
Cholesterol-lowering medication use was three times greater among adults aged 40–64 with health insurance (23.9%) than among those without health insurance (8.1%).
Among adults aged 40–64 with a prescription drug benefit, 24.3% used a cholesterol-lowering medication compared with 9.3% of those who did not have a prescription drug benefit (Figure 5).
Figure 5. Percentage of adults aged 40–64 who used a prescription cholesterol-lowering medication in the past 30 days, by health insurance coverage: United States, 2011–2012
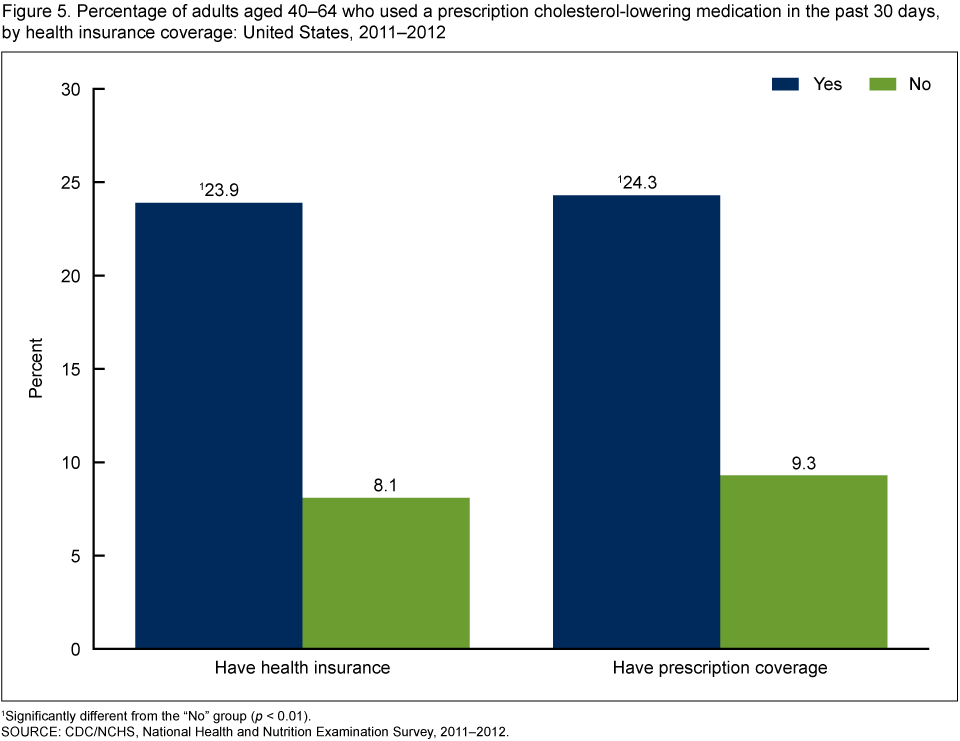
1Significantly different from the “No” group (p < 0.01).
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2011–2012.
Summary
During 2003–2012, there was a significant increase in the percentage of adults aged 40 and over who used a prescription cholesterol-lowering medication. In 2003–2004, one in five adults reported using a prescription cholesterol-lowering medication in the past 30 days. By 2011–2012, that number had risen to one in four adults. In 2011–2012, the majority of adults using a cholesterol-lowering medication reported using a statin alone (83%). Ten percent used both a statin and a nonstatin and another 7% used only a nonstatin. Simvastatin was the most commonly used medication, with 42% of all cholesterol-lowering medication users reporting its use, followed by atorvastatin (20.2%).
Use of a prescription cholesterol-lowering medication increased with age but was similar between men and women and race and Hispanic origin groups. Adults aged 40–64 who reported having health insurance or prescription medication coverage were more likely to take prescription cholesterol-lowering medications.
Hypercholesterolemia or high cholesterol is one of the most common preventable risk factors for atherosclerotic CVD. In 2011–2012, more than 30 million Americans aged 20 and over (13%) had measured high total cholesterol (5). There is extensive and consistent evidence supporting the use of cholesterol-lowering medication, especially statins, in addition to lifestyle changes, to treat lipid disorders and reduce atherosclerotic CVD events. The 2013 cholesterol treatment guidelines updated recommendations for statin therapy on the basis of low-density lipid cholesterol levels and atherosclerotic CVD risks (6). Approximately 71% of adults with diagnosed CVD, 63% of those with diagnosed diabetes, and 54% of those with diagnosed hypercholesterolemia reported taking prescription cholesterol-lowering medications.
Definitions
Prescription medication use: Survey participants were asked if they had taken a prescription medication in the past 30 days. Those who answered “yes” were asked to show the interviewer the medication containers of all prescription medications. For each drug reported, the interviewer recorded the product’s complete name from the container (7).
Cholesterol-lowering medication: Prescription medications were classified based on the three-level nested therapeutic classification scheme of Cerner Multum’s Lexicon (8). Cholesterol-lowering medications were identified using the secondary level of drug category codes, specifically code 19. Another prescription drug, omega-3-polyunsaturated fatty acid (brand name Lovaza or Omacor), was also considered a cholesterol-lowering medication.
Statins and nonstatins: The third level of drug category codes were used to identify statins (code 173); nonstatins (codes 174, 241, 252, and 316); and combinations of the two (code 317). Omega-3-polyunsaturated fatty acid was included in the nonstatin subclass. Persons who reported taking both a statin and a nonstatin either in a single pill combination or two separate pills were considered statin and nonstatin users.
Health insurance coverage: Based on the question, “Are you covered by health insurance or some other kind of health care plan?”
Prescription drug benefit: Based on the question, “Do any of these plans cover any part of the cost of prescriptions?”
Diagnosed cardiovascular disease: Based on an affirmative response to any one of four questions about doctor-diagnosed heart attack, angina, coronary heart disease, and stroke.
Diagnosed diabetes: Based on an affirmative response to the question, “Have you ever been told by a doctor or other health professional that you have diabetes?”
Diagnosed hypercholesterolemia: Based on an affirmative response to the question, “Have you ever been told by a doctor or other health professional that your blood cholesterol level was high?”
Data source and methods
NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (9). It is conducted by the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics. Data from NHANES 2003–2004 through 2011–2012 were used for trend analysis, and the most recent cycle of 2011–2012 data were further used for examining the patterns of cholesterol-lowering medication use.
The NHANES sample is selected through a complex, multistage probability design. In 2011–2012, non-Hispanic Asian, non-Hispanic black, and Hispanic persons; persons with low income (below 130% of the federal poverty level); and those aged 60 and over were oversampled to obtain reliable estimates of health and nutritional measures for these population subgroups. Sample weights, accounting for the differential probabilities of selection, nonresponse, and noncoverage, were used for analyses. Variance estimates accounted for the complex survey design using Taylor series linearization. Estimates for the total adult population aged 40 and over, for men and women, and for race and Hispanic origin subpopulations were age-adjusted by the direct method to the 2000 U.S. census population, using age groups 40–59, 60–74, and 75 and over (10). Differences between groups were evaluated using a t statistic at the p less than 0.01 significance level (adjusted for multiple comparisons). All differences reported are statistically significant unless otherwise noted. To test for linear trends, the null hypothesis of nonlinear trend was examined using orthogonal polynomials. Statistical analyses were conducted using SAS version 9.3 (SAS Institute, Inc., Cary, N.C.) and SUDAAN version 11.0 (RTI International, Research Triangle Park, N.C.).
About the authors
Qiuping Gu, Ryne Paulose-Ram, Vicki L. Burt, and Brian K. Kit are with CDC’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys.
References
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 129(3):e28–e292. 2014.
- Taylor F, Huffman MD, Macedo AF, Moore TH, Burke M, Davey Smith G, et al. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev 1:CD004816. 2013.
- Cholesterol Treatment Trialists’ (CTT) Collaborators, Mihaylova B, Emberson J, Blackwell L, Keech A, Simes J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: Meta-analysis of individual data from 27 randomised trials. Lancet 380(9841):581–90. 2012.
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 106(25):3143–421. 2002.
- Carroll MD, Kit BK, Lacher DA, Yoon SS. Total and high-density lipoprotein cholesterol in adults: National Health and Nutrition Examination Survey, 2011–2012. NCHS data brief, no 132. Hyattsville, MD: National Center for Health Statistics. 2013.
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 129(25 Suppl 2):S1–45. 2014.
- National Center for Health Statistics. National Health and Nutrition Examination Survey. Dietary supplements and prescription medication questions [PDF - 129KB].
- National Center for Health Statistics. National Health and Nutrition Examination Survey. 1988–2012 data documentation, codebook, and frequencies: Prescription medications–drug information.
- National Center for Health Statistics. National Health and Nutrition Examination Survey.
- Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People 2010 Statistical Notes, no 20. Hyattsville, MD: National Center for Health Statistics. 2001.
Suggested citation
Gu Q, Paulose-Ram R, Burt VL, Kit BK. Prescription cholesterol-lowering medication use in adults aged 40 and over: United States, 2003–2012. NCHS data brief, no 177. Hyattsville, MD: National Center for Health Statistics. 2014.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examinination Surveys
Kathryn S. Porter, M.D., M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: December 23, 2014
- Content source: