

Health Insurance Affects Diagnosis and Control of Hypercholesterolemia and Hypertension Among Adults Aged 20-64: United States, 2005-2008
 ShareCompartir
ShareCompartir
NCHS Data Brief No. 57, January 2011
On this Page
- Key findings
- Adults with health insurance are more likely to be tested for high cholesterol than those without insurance.
- Hypercholesterolemia is more likely to be uncontrolled, and more likely to be undiagnosed, among uninsured adults with the condition than among those with health insurance.
- Hypertension is more likely to be uncontrolled, and more likely to be undiagnosed, among uninsured adults with the condition than among those with health insurance.
- More than one in six adults with either hypercholesterolemia or hypertension have no health insurance coverage.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
PDF Version (486 KB)
Susan E. Schober, Ph.D.; Diane M. Makuc, Dr.P.H.; Cindy Zhang, M.D., M.P.H.; Jocelyn Kennedy-Stephenson, M.S.; and Vicki Burt, Sc.M., R.N.
Key findings
Data from the National Health and Nutrition Examination Survey (NHANES), 2005-2008
- Nonelderly adults with health insurance were more likely to have had a test for high cholesterol in the past 5 years compared with those with no insurance.
- Hypercholesterolemia was undiagnosed among almost one-half of nonelderly adults with the condition who lacked health insurance-about twice the percentage for those who had insurance.
- Hypertension was undiagnosed among about 40% of nonelderly adults with that condition who lacked health insurance-about twice the percentage for those with insurance.
- Control of hypercholesterolemia and hypertension was also negatively affected by lack of health insurance, primarily due to the greater prevalence of undiagnosed conditions among those without insurance.
Lack of health insurance presents a barrier to obtaining routine preventive care and early diagnosis and management of chronic conditions. In 2005-2008, approximately 23% of adults aged 20-64 had no health insurance. Hypercholesterolemia (high total cholesterol or taking medication to lower cholesterol) and hypertension (high blood pressure or taking medication to lower blood pressure) are major risk factors for cardiovascular disease, particularly when untreated and uncontrolled (1,2) and are common among nonelderly adults. In 2005-2008, 23% of adults aged 20-64 had hypercholesterolemia and 23% had hypertension. The objective of this report is to quantify the association between health insurance coverage and the diagnosis and control of hypercholesterolemia and hypertension among persons with those conditions. The criteria used to define these conditions are provided in the “Definitions” section of the report.
Keywords: health care access, high total cholesterol, high blood pressure, National Health and Nutrition Examination Survey
Adults with health insurance are more likely to be tested for high cholesterol than those without insurance.

† Significantly different from those with private health insurance and those with public health insurance.
§ Significantly different from those with private health insurance.
NOTE: Access data table for Figure 1 [PDF - 63 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005-2008.
- In 2005-2008, nonelderly adults aged 20-64 with either private or public health insurance were almost twice as likely to have had their blood cholesterol checked in the past 5 years compared with those with no coverage (Figure 1).
- Among adults aged 40-64 with private or public health insurance, approximately 83% had received the recommended blood cholesterol screening in the past 5 years. In contrast, 52% of uninsured persons in this age group received the recommended screening. Younger adults were less likely to be screened than older adults.
Hypercholesterolemia is more likely to be uncontrolled, and more likely to be undiagnosed, among uninsured adults with the condition than among those with health insurance.

† Significantly different from those with private health insurance and those with public health insurance.
NOTE: Access data table for Figure 2 [PDF - 63 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005-2008.
- Among nonelderly adults with hypercholesterolemia, the condition was uncontrolled for approximately 80% of those with no health insurance, compared with about 60% of those with private or public health insurance (Figure 2).
- Control of hypercholesterolemia varied by insurance coverage status only among adults aged 40-64. Among adults 20-39, the percentage with uncontrolled hypercholesterolemia did not differ by health insurance coverage. In addition, those 20-39 were more likely than those in the older age group to have uncontrolled hypercholesterolemia, regardless of health insurance coverage.
- Differences in the control of hypercholesterolemia between insured and uninsured adults were primarily related to differences in the diagnosis of the condition. Among nonelderly adults who had hypercholesterolemia, the condition was undiagnosed among 48% of those who were uninsured, compared with 27% of those with private and 25% with public health insurance. In contrast, the condition was diagnosed but currently not adequately controlled among approximately one-third of all nonelderly adults with the condition, and there was no difference in the percentage among those with private, public, or no health insurance.
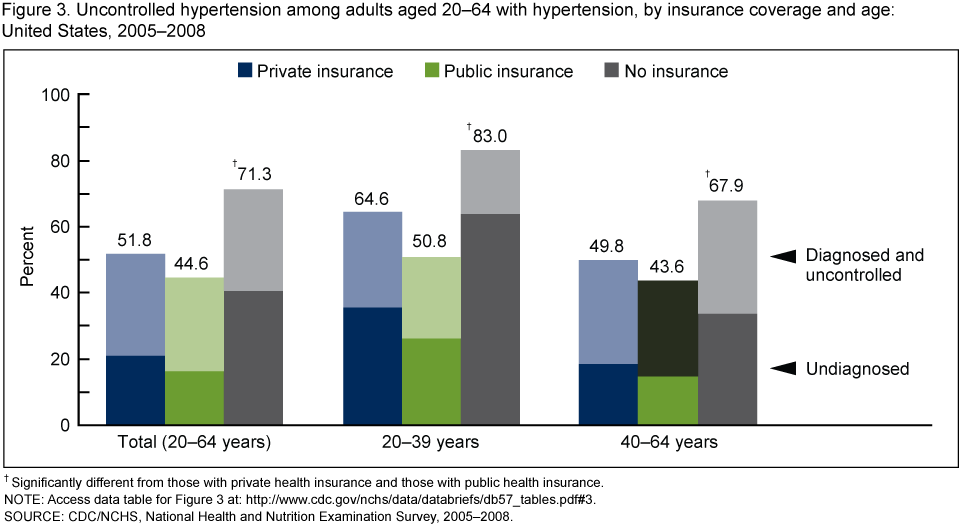
Hypertension is more likely to be uncontrolled, and more likely to be undiagnosed, among uninsured adults with the condition than among those with health insurance.
† Significantly different from those with private health insurance and those with public health insurance.
NOTE: Access data table for Figure 3 [PDF - 63 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005-2008.
- Among nonelderly adults with hypertension, the condition was uncontrolled among 71% of those with no health insurance, compared with 52% of those with private and 45% with public insurance (Figure 3).
- Control of hypertension was more likely among those with private or public insurance, compared with those with no insurance, for persons of both age groups (20-39 and 40-64 years), but 20-39 year olds were more likely to lack control than those aged 40-64.
- Similar to the results for hypercholesterolemia, differences in the control of hypertension between insured and uninsured adults were primarily related to differences in the diagnosis of the condition. Among nonelderly adults with hypertension, the condition was undiagnosed among 40% of the uninsured-a rate approximately twice that for those with either private or public insurance. However, hypertension was diagnosed but currently uncontrolled among approximately 30% of all nonelderly persons with the condition, and there was little difference between those with and without health insurance coverage.
More than one in six adults with either hypercholesterolemia or hypertension have no health insurance coverage.

† Significantly different from those aged 20-39.
NOTE: Access data table for Figure 4 [PDF - 63 KB].
SOURCE: CDC/NCHS, National Health and Nutrition Examination Survey, 2005-2008.
- In 2005-2008, 18% of adults aged 20-64 with hypercholesterolemia or hypertension, or both, had no health insurance, 68% had private health insurance, and 14% had public health insurance (Figure 4).
- Among those with either or both of these conditions, adults aged 20-39 were more likely to be uninsured (25%) than those 40-64 (15%).
- Nonelderly adults with either or both of these conditions were less likely to be uninsured (18%) than all nonelderly adults (23%) (data not shown).
Summary
In 2005-2008, 23% of adults aged 20-64 had hypercholesterolemia and 23% had hypertension. The prevalence was higher among adults 40-64 (33% for hypercholesterolemia and 36% for hypertension) than among those 20-39 (10% and 8%, respectively). Overall during this period, lack of health insurance coverage was associated with poorer rates of diagnosis and control of hypercholesterolemia and hypertension among nonelderly U.S. adults with these conditions. Uninsured persons with each of these conditions were about twice as likely to be undiagnosed as those who had private or public coverage. Among persons with hypercholesterolemia, the condition was uncontrolled among 81% of uninsured persons, compared with 61% of those with private coverage and 58% with public coverage. Similarly, among those with hypertension, 71% of the uninsured group had uncontrolled hypertension compared with 52% of the private and 45% of the public coverage groups. The association of insurance coverage with the diagnosis and control of hypercholesterolemia was found only among those aged 40-64 and not in the younger age group. In contrast, the association of insurance coverage with the diagnosis and control of hypertension was found for both the younger and older age groups.
Hypercholesterolemia and hypertension were uncontrolled in more than one-half of nonelderly adults with each condition, regardless of health insurance coverage, even though therapies are available that adequately control these conditions (1,2). Lack of control may be due to many factors, including that the conditions are not diagnosed or are inadequately treated, or because of poor compliance with prescribed therapy (whether lifestyle changes or medication). The higher percentages of adults with uncontrolled conditions among those without health insurance than among those with health insurance are explained in large part by higher percentages of undiagnosed conditions among uninsured adults.
Nonelderly adults without health insurance coverage were also less likely to have received recommended screening for high cholesterol. One objective of the Healthy People 2010 initiative was to increase to at least 80% the proportion of adults aged 18 and over who have been screened for high cholesterol in the last 5 years (3). This level of screening was attained among persons aged 40-64 who had either private or public insurance but was not met for uninsured adults in that age group or for younger adults regardless of insurance coverage. Another Healthy People 2010 objective was to increase to 95% the proportion of adults 18 and over who have had their blood pressure checked by a health professional in the last 2 years and can state whether their blood pressure is normal or high (3). In 2008, adults 18-64 with private or public insurance (94%-95%) were closer to attaining this target than those with no insurance (82%) (National Health Interview Survey, unpublished data). The definitions of hypertension and hypercholesterolemia used in this report are based on clinical measures and a history of currently taking medication for the respective conditions, consistent with current definitional guidelines (1,2). Expanding the definitions to include persons with nonpharmacological control of these conditions increases estimates of prevalence and control (4,5) but was not considered in this report.
Other studies (see, for example, references 6-8) have examined the association of health insurance coverage with diagnosis and control of hypertension and hypercholesterolemia based on NHANES data, but in most cases definitions or target age groups differ, so results are not directly comparable with those reported here. A previous study based on NHANES III (1988-1994) data found that nonelderly adults with hypertension and hypercholesterolemia (as defined in this brief) were much more likely to be undiagnosed if they were uninsured than insured, even after adjustment for sociodemographic characteristics. Three measures of access to care that are affected by health insurance coverage (having a regular site of care, a regular provider, and a recent health care contact) explained much of the difference in undiagnosed conditions by insurance status (9). This report provides continued evidence of the positive association of health insurance coverage with the diagnosis and control of hypertension and hypercholesterolemia.
Definitions
Hypercholesterolemia: Blood total cholesterol level of 240 mg/dL or greater or currently taking cholesterol-lowering medication (based on positive responses to the following questions: “Have you ever had your blood cholesterol checked?”; “Have you ever been told by a doctor or other health professional that your blood cholesterol level was high?”; “To lower your blood cholesterol, have you ever been told by a doctor or other health professional to take prescribed medication?”; and “Are you now following this advice to take prescribed medication?”).
Undiagnosed hypercholesterolemia: A finding of hypercholesterolemia and never told by a health care provider that cholesterol was high (based on a negative response to the question, “Have you ever been told by a doctor or health professional that your blood cholesterol is high?”).
Uncontrolled hypercholesterolemia: Blood total cholesterol level of 240 mg/dL or greater among those with hypercholesterolemia.
Screened for high cholesterol in the past 5 years: Based on an affirmative response to the question, “Have you ever had your blood cholesterol checked?” and response indicating less than 5 years ago to the question, “About how long has it been since you last had your blood cholesterol level checked?”
Hypertension: Systolic blood pressure of 140 mm Hg or greater, or diastolic blood pressure of 90 mm Hg or greater, or currently taking medication to lower blood pressure (based on positive responses to the following questions: “Have you ever been told by a doctor or other health professional that you had hypertension, also called high blood pressure?”; “Because of your [high blood pressure/hypertension], have you ever been told to take prescribed medicine?”; and “Are you now taking a prescribed medicine?”).
Undiagnosed hypertension: A finding of hypertension and never told by a health care provider that blood pressure was high (based on a negative response to the question, “Have you ever been told by a doctor or other health professional that you had hypertension, also called high blood pressure?”).
Uncontrolled hypertension: Systolic blood pressure of 140 mm Hg or greater, or diastolic blood pressure of 90 mm Hg or greater, among those with hypertension.
Health insurance coverage: At the time of interview. Private insurance excludes plans that pay for only one type of service, such as dental or vision care. Persons covered by both public and private plans are classified as having private coverage. Public coverage includes Medicaid, Children’s Health Insurance Program (CHIP), state-sponsored or other government-sponsored health plan, Medicare (disability), or military health care (TRICARE, VA, or CHAMP-VA). Uninsured persons do not have private or public coverage.
Data source and methods
The National Health and Nutrition Examination Surveys (NHANES) conducted from 2005 through 2008 were used for these analyses. NHANES is a cross-sectional survey designed to monitor the health and nutritional status of the civilian noninstitutionalized U.S. population (10). The survey consists of interviews conducted in participants’ homes, standardized physical examinations conducted in mobile examination centers, and laboratory tests utilizing blood and urine specimens provided by participants during the physical examination.
The NHANES sample is selected through a complex, multistage design that includes selection of primary sampling units (counties), household segments within the counties, and, finally, sample persons from selected households. In 2005-2008, non-Hispanic black and Mexican-American persons, persons with low-income, and those aged 60 years and over were oversampled in order to obtain reliable estimates of health and nutritional measures for these population subgroups. In 2007-2008, all Hispanic persons were oversampled in addition to the oversampling of the Mexican-American population. In 1999, NHANES became a continuous survey fielded on an ongoing basis. Each year of data collection is based on a representative sample covering all ages of the civilian noninstitutionalized population. Public-use data files are released in 2-year cycles.
Sample weights, which account for the differential probabilities of selection, nonresponse, and noncoverage, are incorporated into the estimation process. All variance estimates accounted for the complex survey design by using Taylor series linearization (11). Differences between groups were evaluated using a univariate t statistic. All significance tests were two-sided using p < 0.05 as the level of statistical significance. All differences reported are statistically significant unless otherwise indicated. Adjustments were not made for multiple comparisons.
Statistical analyses were conducted using the SAS System for Windows (release 9.1; SAS Institute, Inc., Cary, North Carolina) and SUDAAN (release 9.0; Research Triangle Institute, Research Triangle Park, North Carolina).
About the authors
Susan Schober and Vicki Burt are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health and Nutrition Examination Surveys. Diane Makuc is with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Office of Analysis and Epidemiology. Cindy Zhang is with Harris IT Services. Jocelyn Kennedy-Stephenson is with Northrop Grumman Corporation.
References
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 285:2486-97. 2001.
- Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 289(19):2560-71. 2003.
- U.S. Department of Health and Human Services. Healthy People 2010, 2nd ed, 2 vols. Washington, DC: U.S. Government Printing Office. 2000.
- Cutler JA, Sorlie PD, Wolz M, Thom T, Fields LE, Roccella EJ. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988-1994 and 1999-2004. Hypertension 52(5):818-27. 2008.
- Hyre AD, Muntner P, Menke A, Raggi P, He J. Trends in ATP-III-defined high blood cholesterol prevalence, awareness, treatment, and control among U.S. adults. Ann Epidemiol 17(7):548-55. 2007.
- Duru OK, Vargas RB, Kermah D, Pan D, Norris KC. Health insurance status and hypertension monitoring and control in the United States. Am J Hypertens 20(4):348-53. 2007.
- Ostchega Y, Hughes JP, Wright JD, McDowell MA, Louis T. Are demographic characteristics, health care access and utilization, and comorbid conditions associated with hypertension among US adults? Am J Hypertens 21(2):159-65. 2008.
- Wilper AP, Woolhandler S, Lasser KE, McCormick D, Bor DH, Himmelstein DU. Hypertension, diabetes, and elevated cholesterol among insured and uninsured U.S. adults. Health Aff 28(6):w1151-w1159. 2009.
- Ayanian JZ, Zaslavsky AM, Weissman JS, Schneider EC, Ginsburg JA. Undiagnosed hypertension and hypercholesterolemia among uninsured and insured adults in the Third National Health and Nutrition Examination Survey. Am J Public Health 93(12):2051-4. 2003.
- National Center for Health Statistics. National Health and Nutrition Examination Surveys, 2005-2008. Accessed May 2010.
- National Center for Health Statistics. National Health and Nutrition Examination Survey: Analytic guidelines. Accessed May 2010.
Suggested citation
Schober SE, Makuc DM, Zhang C, Kennedy-Stephenson J, Burt V. Health insurance affects diagnosis and control of hypercholesterolemia and hypertension among adults aged 20-64: United States, 2005-2008. NCHS data brief, no 57. Hyattsville, MD: National Center for Health Statistics. 2011.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health and Nutrition Examination Surveys
Clifford L. Johnson, M.S.P.H., Director
Office of Analysis and Epidemiology
Linda T. Bilheimer, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: January 26, 2011
- Content source: