

Use of Emergency Contraception Among Women Aged 15–44: United States, 2006–2010
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- The percentage of sexually experienced women who have ever used emergency contraception has increased over time.
- Ever-use of emergency contraception varied by age, marital status, Hispanic origin and race, and education.
- Nearly one-half of women who had ever used emergency contraception reported fear of method failure as a reason for use, but variation occurred by age, Hispanic origin and race, and education.
- Nearly one-half of women who had ever used emergency contraception gave having unprotected sex as a reason for use, but variation occurred across Hispanic origin and race, and education.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 112, February 2013
PDF Version (679 KB)
Kimberly Daniels, Ph.D.; Jo Jones, Ph.D.; and Joyce Abma, Ph.D.
Key findings
Data from the 2006–2010 National Survey of Family Growth
- In 2006–2010, among sexually experienced women aged 15–44, roughly one in nine (11% or 5.8 million) women had ever used emergency contraception, up from 4.2% in 2002.
- Most women who had ever used emergency contraception had done so once (59%) or twice (24%).
- Young adult women aged 20–24 were most likely to have ever used emergency contraception; about one in four had done so (23%).
- Almost 1 in 5 never-married women (19%), 1 in 7 cohabiting women (14%), and 1 in 20 currently or formerly married women (5.7%) had ever used emergency contraception.
- About one in two women reported using emergency contraception because of fear of method failure (45%), and about one in two reported use because they had unprotected sex (49%).
Emergency contraception can be used by women after sexual intercourse in an effort to prevent an unintended pregnancy. Roughly one-half of all pregnancies in the United States are unintended (1,2). The FDA first approved emergency contraceptive pills in 1998, but there is evidence of limited use of hormonal contraceptives for emergency contraception since the 1960s (3,4). Now, there are at least four brands of emergency contraceptive pills; most are available over the counter for women aged 17 and over (5). Although insertion of a copper intrauterine device can be used for emergency contraception (1,4), this report focuses only on emergency contraceptive pills. This report describes trends and variation in the use of emergency contraception and reasons for use among sexually experienced women aged 15–44 using the 2006–2010 National Survey of Family Growth.
Keywords: unintended pregnancy, method failure, unprotected sex, National Survey of Family Growth
The percentage of sexually experienced women who have ever used emergency contraception has increased over time.
Figure 1. Percentage of sexually experienced women aged 15–44 who have ever used emergency contraception: United States, 1995, 2002, and 2006–2010, and frequency of use among women who have ever used emergency contraception, 2006–2010
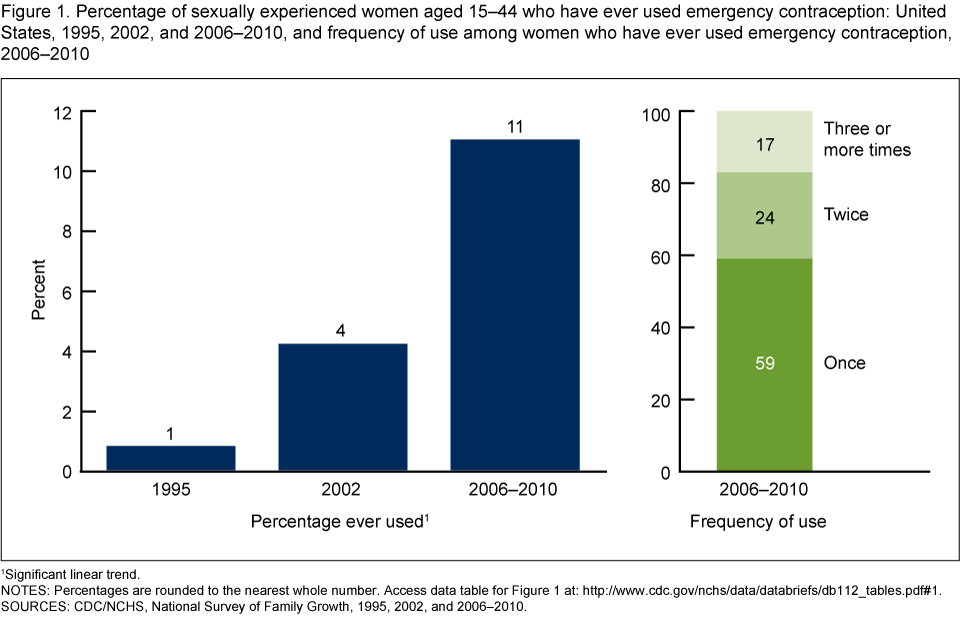
1 Significant linear trend.
NOTES: Percentages are rounded to the nearest whole number. Access data table for Figure 1 [PDF – 146 KB].
SOURCES: CDC/NCHS, National Survey of Family Growth, 1995, 2002, and 2006–2010.
In 2006–2010, 11% (or 5.8 million) of sexually experienced women aged 15–44 had ever used emergency contraception, compared with 4.2% of women in 2002 and less than 1% in 1995 (Figure 1). In 2006–2010, of women who had ever used emergency contraception, 59% had used it once, 24% had used it twice, and 17% had used it three or more times.
Ever-use of emergency contraception varied by age, marital status, Hispanic origin and race, and education.
Figure 2. Percentage of sexually experienced women aged 15–44 who have ever used emergency contraception, by selected characteristics: United States, 2006–2010

1 Significantly different from age group 20–24.
2 Significantly different from age group 30–44.
3 Significantly different from never-married women.
4 Significantly different from currently or formerly married women.
5 Significantly different from non-Hispanic black women.
6 Significant linear trend.
NOTES: Percentages are rounded to the nearest whole number. Analyses of education are limited to women aged 22–44 at the time of interview. GED is General Educational Development high school equivalency diploma. Access data table for Figure 2 [PDF – 146 KB].
SOURCE: CDC/NCHS, National Survey of Family Growth, 2006–2010.
- Nearly one in four (23%) sexually experienced women aged 20–24 had ever used emergency contraception, compared with 16% of women aged 25–29 and 14% of women aged 15–19 (Figure 2). Older women had used emergency contraception less than younger women, with 5.0% of women aged 30–44 having ever used it.
- A larger proportion of never-married women had ever used emergency contraception (19%) compared with women who were cohabiting (14%) or currently or formerly married (5.7%).
- Non-Hispanic white and Hispanic women were more likely to have ever used emergency contraception (11%) compared with non-Hispanic black women (7.9%).
- Ever-use of emergency contraception increased with educational attainment—12% of women with a bachelor’s degree or higher and 11% of women with some college education had ever used it. This compares with 7.1% of women who had a high school diploma or GED and 5.5% of women with less than a high school education.
Nearly one-half of women who had ever used emergency contraception reported fear of method failure as a reason for use, but variation occurred by age, Hispanic origin and race, and education.
Figure 3. Use of emergency contraception due to fear of method failure among women aged 15–44 who had ever used emergency contraception, by selected characteristics: United States, 2006–2010

1 Significantly different from age group 15–19.
2 Significantly different from non-Hispanic white women.
3 Significant linear trend.
NOTES: Percentages are rounded to the nearest whole number. Reasons for use are not mutually exclusive, women could provide more than one response; see “Data source and methods” section for details. Analyses of education are limited to women aged 22–44 years at time of interview. GED is General Educational Development high school equivalency diploma. Access data table for Figure 3 [PDF – 146 KB].
SOURCE: CDC/NCHS, National Survey of Family Growth, 2006–2010.
- A larger percentage of older women, those aged 30–44 (52%), reported using emergency contraception because they feared that the contraceptive method they used would not work, compared with 34% of women aged 15–19 (Figure 3). The difference between women aged 15–19 and 25–29 was not statistically significant.
- A larger percentage of non-Hispanic white women (53%) reported emergency contraceptive use due to fear of method failure compared with non-Hispanic black (27%) and Hispanic women (33%).
- The percentage of women reporting use of emergency contraception because of fear of method failure increased with more education—from 26% of women with less than a high school education to 58% of women with a bachelor’s degree or higher.
Nearly one-half of women who had ever used emergency contraception gave having unprotected sex as a reason for use, but variation occurred across Hispanic origin and race, and education.
Figure 4. Use of emergency contraception due to unprotected sex among women aged 15–44 who had ever used emergency contraception, by selected characteristics: United States, 2006–2010

1 Significantly different from non-Hispanic white women.
2 Significant linear trend.
NOTES: Percentages are rounded to the nearest whole number. Reasons for use are not mutually exclusive, women could provide more than one response; see “Data source and methods” section for details. Analyses of education are limited to women aged 22–44 years at the time of interview. GED is General Educational Development high school equivalency diploma. Access data table for Figure 4 [PDF – 146 KB].
SOURCE: CDC/NCHS, National Survey of Family Growth, 2006–2010.
- The percentage of women in each age group reporting that they used emergency contraception because they had unprotected sex was similar, around 50% (Figure 4).
- Hispanic women (59%) and non-Hispanic black women (60%) more often reported using emergency contraception because they had unprotected sex compared with non-Hispanic white women (43%).
- The percentage of women reporting use of emergency contraception because of unprotected sex decreased with more education—from 62% of those with less than a high school education to 43% of women with a bachelor’s degree or higher.
Summary
In 2006–2010, one in nine sexually experienced women aged 15–44 had used emergency contraception at least once. The ever-use of emergency contraception was most common among women aged 20–24, those who never married, Hispanic or non-Hispanic white women, and those who attended college. Most women who had used emergency contraception had done so once or twice.
Among women who had ever used emergency contraception, nearly equal percentages of women, around 50%, reported having used it because of fear of method failure and because of unprotected sex. Non-Hispanic black and Hispanic women and those with less education were more likely to have used emergency contraception because of unprotected sex, compared with women of other characteristics. Older women, non-Hispanic white women, and women with more education more often used emergency contraception because of fear of method failure, compared with women of other characteristics.
When looking at age differences, it should be kept in mind that not all women had access to emergency contraception during the earlier portion of their reproductive years. It was expected that older women would have used emergency contraception less frequently than younger women for reasons of both supply and demand: Emergency contraception was not FDA approved in their early reproductive years, and the use of sterilization as a contraceptive method increases with age, consequently decreasing the potential demand for emergency contraception (6). Additionally, differences across marital status and other groups presented here could be confounded by age; for instance, married women are on average older than never-married women.
Definitions
Education: Educational attainment at the time of interview, indicating the highest grade or degree finished. Analyses by education were limited to women aged 22–44 at the time of interview because large percentages of women aged 15–21 are still attending school. Using the full age range of 15–44 would misclassify many young women still attending school as having low educational attainment.
Emergency contraception: Methods that women can use after sexual intercourse in instances where a method of contraception was not used during intercourse, or if a woman thought the method that she and her partner used might fail to protect them from an unintended pregnancy. Emergency contraception includes emergency contraceptive pills and the insertion of a copper intrauterine device (IUD) by a medical provider (1,4,7); however, this report describes use only as was reported in response to the survey question described below. The 2006–2010 National Survey of Family Growth (NSFG) did not specifically ask about IUD use for emergency contraception.
Ever-use of emergency contraception: Similar questions were asked in each survey to measure ever-use of emergency contraception among women who had ever had sex; however, examples of brand names were added as more became available. In 1995, women were asked, “Have you ever used ‘morning after’ pills?” The 2002 survey question asked, “Have you ever used ‘morning after’ pills or emergency contraception?” The 2006–2010 NSFG asked, “Have you ever used emergency contraception, also known as ‘Plan B’ or ‘Preven’ or ‘Morning after’ pills?”
Frequency of use of emergency contraception: Women who reported ever using emergency contraception were asked, “How many different times have you used emergency contraception?”
Reasons for using emergency contraception: Women who had ever used emergency contraception were asked, “Did you use emergency contraception because you were worried your birth control method would not work, you didn’t use birth control that time, or for some other reason?” For convenience in writing, the phrases “fear of method failure” and “unprotected sex” were used. Women could give multiple responses to this question because they may have had more than one reason or used emergency contraception multiple times for different reasons. If a woman chose both “worried the method would not work” and “did not use birth control,” she was counted in both categories. Most emergency contraception users reported only one reason. Too few women reported “some other reason” to analyze.
Sexually experienced: Women who had ever had vaginal, heterosexual intercourse. Of the sample of women aged 15–44 in the 2006–2010 NSFG, 87% had ever had sexual intercourse.
Data source and methods
This report is based primarily on data from the 2006–2010 NSFG. NSFG provides population-level information about lifetime and recent use of emergency contraception among U.S. women of reproductive age. Additional questions in the data set related to the use of emergency contraception are not presented here.
Statistics for this report were produced using SAS software version 9.2. The sampling errors were produced with SUDAAN software version 10.0.1. Percentages were compared using two-tailed t tests at the 5% level. No adjustments were made for multiple comparisons. A weighted least-squares regression method was used to test the significance of the time trend and differences across education. Lack of comment regarding the difference between any two statistics does not mean that the difference was tested and found not to be significant. In the description of the results, when the percentage being cited is below 10%, the text cites the percentage to one decimal point. To make reading easier and to remind the reader that the results are based on samples and subject to sampling error, percentages of 10% and above are shown rounded to the nearest whole number.
This report presents descriptive statistics on ever-use, frequency of use, and reasons for use of emergency contraception by women’s characteristics at the time of interview, not cause-and-effect relationships. A link to a data table that includes percentages and standard errors is listed in the footnotes of each figure. Although not shown in the figures, the supplemental data tables provide information on variation in ever-use and reasons for use of emergency contraception by region and metropolitan residence.
About the authors
Kimberly Daniels, Jo Jones, and Joyce Abma are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Vital Statistics, Reproductive Statistics Branch.
References
- Trussell J, Raymond EG. Emergency contraception: A last chance to prevent unintended pregnancy [PDF – 400 KB]. 2012.
- Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception 84(5):478–85. 2011.
- Ellertson C. History and efficacy of emergency contraception: Beyond Coca-Cola. Int Fam Plan Perspect 22(2):52–6. 1996.
- Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar MS. Contraceptive technology. 20th ed rev. New York: Ardent Media. 2011.
- Food and Drug Administration. Plan B: Questions and answers. 2006.
- Jones J, Mosher WD, Daniels K. Current contraceptive use in the United States, 2006–2010, and changes in patterns of use since 1995. National health statistics reports; no. 60. Hyattsville, MD: National Center for Health Statistics. 2012.
- Cleland K, Zhu H, Goldstuck N, Cheng L, Trussell J. The efficacy of intrauterine devices for emergency contraception: A systematic review of 35 years of experience. Hum Reprod 27(7):1994–2000. 2012.
Suggested citation
Daniels K, Jones J, Abma J. Use of emergency contraception among women aged 15-44: United States, 2006-2010. NCHS data brief, no 112. Hyattsville, MD: National Center for Health Statistics. 2013.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Vital Statistics
Charles J. Rothwell, M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: February 14, 2013
- Content source: