

Recent Trends in Cesarean Delivery in the United States
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- In 2007, the cesarean rate was the highest ever reported in the United States.
- Cesarean rates rose for women in all age groups in the last decade.
- Cesarean rates rose for women in all racial and ethnic groups from 1996 to 2007.
- Cesarean rates increased for infants of all gestational ages in the last decade.
- Cesarean rates varied widely by state.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 35, March 2010
PDF Version (856 KB)
Fay Menacker, Dr. P.H., and Brady E. Hamilton, Ph.D.
Key findings
Data from the Natality Data File, National Vital Statistics System
- The cesarean rate rose by 53% from 1996 to 2007, reaching 32%, the highest rate ever reported in the United States.
- From 1996 to 2007, the cesarean rate increased for mothers in all age and racial and Hispanic origin groups. The pace of the increase accelerated from 2000 to 2007.
- Cesarean rates also increased for infants at all gestational ages; from 1996 to 2006 preterm infants had the highest rates.
- Cesarean rates increased for births to mothers in all U.S. states, and by more than 70% in six states from 1996 to 2007.
In 2007, nearly one-third (32%) of all births were cesarean deliveries (1). Although there are often clear clinical indications for a cesarean delivery, the short- and long-term benefits and risks for both mother and infant have been the subject of intense debate for over 25 years (2). Cesarean delivery involves major abdominal surgery, and is associated with higher rates of surgical complications and maternal rehospitalization, as well as with complications requiring neonatal intensive care unit admission (3–5). In addition to health and safety risks for mothers and newborns, hospital charges for a cesarean delivery are almost double those for a vaginal delivery, imposing significant costs (6).
This report shows trends in cesarean delivery since 1991, focusing on the period from 1996 to 2007 when cesarean rates began to rise following a decline in the early 1990s. Data for 2007 are preliminary and 2006 data are presented when preliminary 2007 data are not available (1,7).
Keywords: cesarean delivery, race and Hispanic origin, gestational age, state specific rates
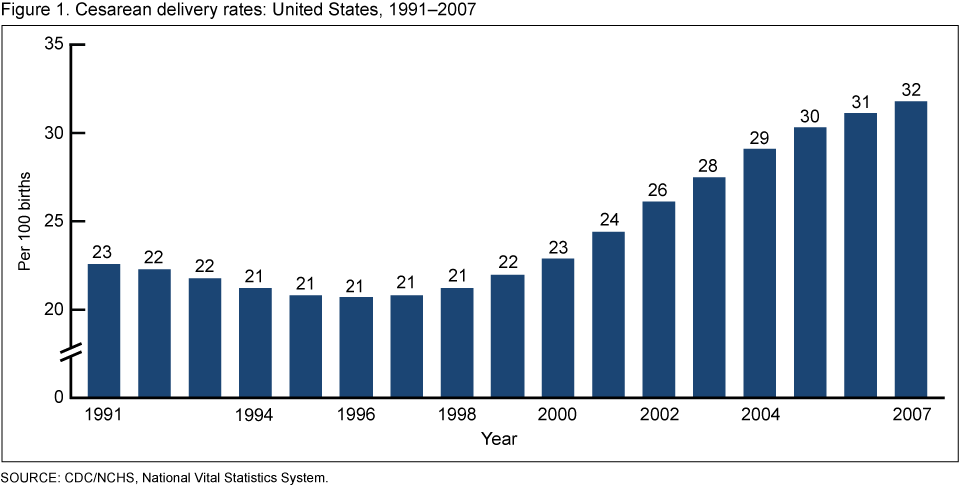
In 2007, the cesarean rate was the highest ever reported in the United States.
There were 1.4 million cesarean births in 2007, representing approximately one-third of all births in the United States.
Following a decline in the early 1990s, the cesarean rate increased by 53% from 1996 to 2007, from 21% to an all-time high of 32% (Figure 1).
The number of cesarean births increased by 71% from 1996 (797,119) to 2007 (1,367,049).
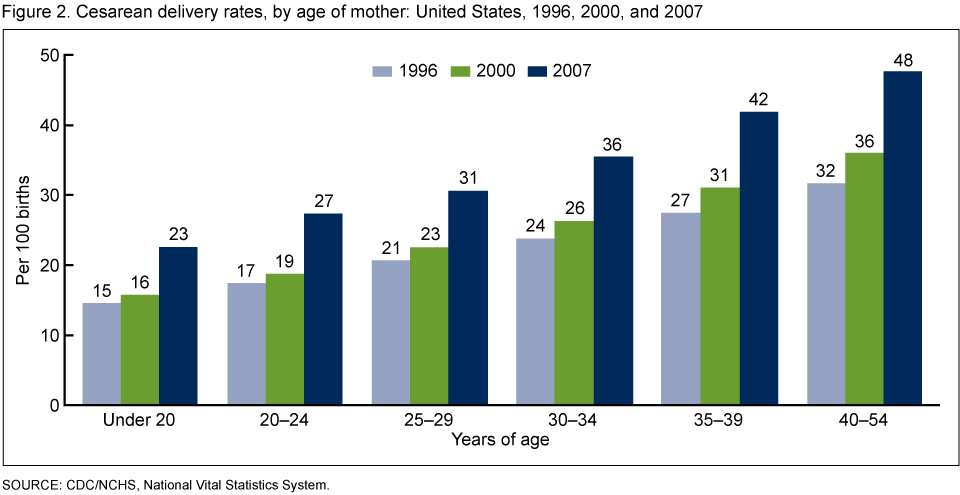
Cesarean rates rose for women in all age groups in the last decade.
Cesarean rates rose for women in all age groups from 1996 to 2007 (Figure 2). Rates for all age groups increased modestly from 1996 to 2000, then rose more than 33% from 2000 to 2007. Women under age 25 experienced the greatest increases in cesarean deliveries from 2000 to 2007 (57%).
Rates of cesarean delivery typically rise with increasing maternal age. As in 1996 and 2000, the rate for mothers aged 40–54 years in 2007 was more than twice the rate for mothers under age 20 (48% and 23%, respectively).
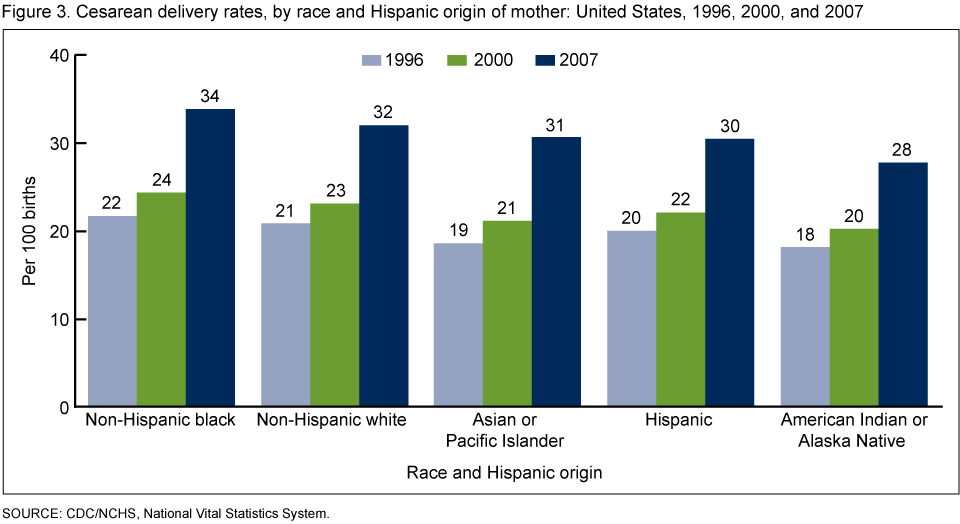
Cesarean rates rose for women in all racial and ethnic groups from 1996 to 2007.
All racial and ethnic groups experienced large increases in cesarean rates from 1996 to 2007 (Figure 3). The rate increased moderately for all groups from 1996 to 2000 (by about 12%), then accelerated with each group experiencing increases of around 40% from 2000 to 2007.
In 2007, cesarean delivery rates were slightly higher for non-Hispanic black women compared with non-Hispanic white women (34% and 32%, respectively). American Indian or Alaska Native women had the lowest cesarean delivery rate (28%).
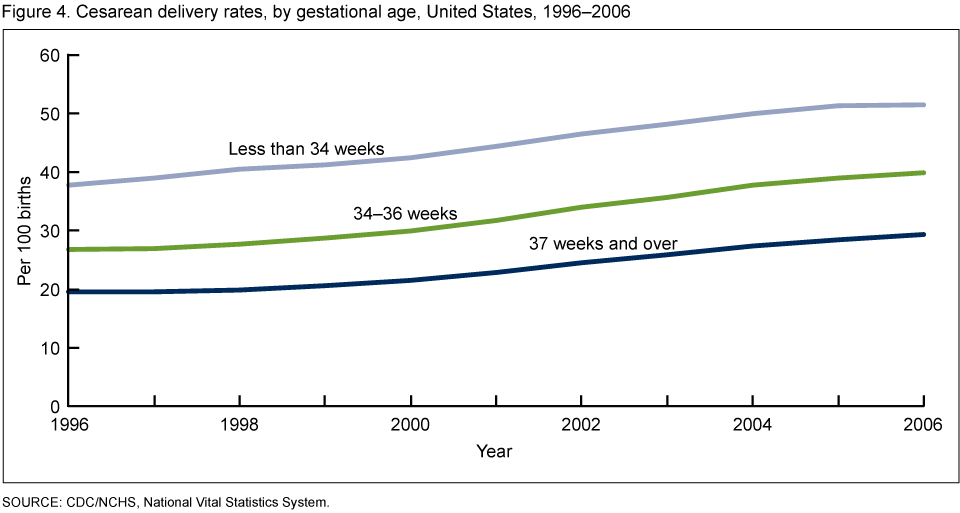
Cesarean rates increased for infants of all gestational ages in the last decade.
Cesarean rates increased for births at all gestational ages from 1996 to 2006 (Figure 4). During the decade, the cesarean rate for early preterm infants (less than 34 completed weeks of gestation) increased by 36%. Rates for infants born late preterm (34 to 36 completed weeks of gestation) and term and over (37 or more completed weeks of gestation) rose by almost 50%.
From 1996 to 2007, cesarean rates were higher for both early and late preterm infants than for term births.
Cesarean rates varied widely by state.
Rates varied considerably by state. In 2007, cesarean rates ranged from less than 25% in Alaska, Idaho, New Mexico, and Utah, to over 35% in Florida, Louisiana, Mississippi, New Jersey, and West Virginia.
Cesarean rates rose significantly in each state from 1996 to 2007 (see Table). The magnitude of the increases varied. Six states (Colorado, Connecticut, Florida, Nevada, Rhode Island, and Washington) had increases of over 70%. In 34 states, cesarean delivery rates increased by 50% or more.
Table. Cesarean delivery rates, by state: United States, 1996 and 2007 and percent change, 1996–2007
| 1996 | 2007 | Percent change 1996-2007 |
|
|---|---|---|---|
| United States | 20.7 | 31.8 | 54 |
| Alabama | 23.3 | 33.8 | 45 |
| Alaska | 16.7 | 22.6 | 35 |
| Arizona | 16.1 | 26.2 | 63 |
| Arkansas | 25.3 | 34.8 | 38 |
| California | 20.6 | 32.1 | 56 |
| Colorado | 15.1 | 25.8 | 71 |
| Connecticut | 19.8 | 34.6 | 75 |
| Delaware | 21.0 | 32.1 | 53 |
| District of Columbia | 21.3 | 32.6 | 53 |
| Florida | 21.6 | 37.2 | 72 |
| Georgia | 20.9 | 32.0 | 53 |
| Hawaii | 17.5 | 26.4 | 51 |
| Idaho | 16.0 | 24.0 | 50 |
| Illinois | 19.3 | 30.3 | 57 |
| Indiana | 20.3 | 29.4 | 45 |
| Iowa | 18.6 | 29.4 | 58 |
| Kansas | 19.2 | 29.8 | 55 |
| Kentucky | 21.3 | 34.6 | 62 |
| Louisiana | 26.4 | 35.9 | 36 |
| Maine | 20.8 | 30.0 | 44 |
| Maryland | 21.6 | 33.1 | 53 |
| Massachusetts | 19.8 | 33.5 | 69 |
| Michigan | 20.2 | 30.4 | 50 |
| Minnesota | 16.9 | 26.2 | 55 |
| Mississippi | 26.6 | 36.2 | 36 |
| Missouri | 20.4 | 30.3 | 49 |
| Montana | 19.1 | 29.4 | 54 |
| Nebraska | 19.8 | 30.9 | 56 |
| Nevada | 19.3 | 33.1 | 72 |
| New Hampshire | 20.3 | 30.8 | 52 |
| New Jersey | 24.0 | 38.3 | 60 |
| New Mexico | 17.2 | 23.3 | 35 |
| New York | 22.9 | 33.7 | 47 |
| North Carolina | 21.1 | 30.7 | 45 |
| North Dakota | 18.9 | 28.4 | 50 |
| Ohio | 19.0 | 29.8 | 57 |
| Oklahoma | 22.5 | 33.6 | 49 |
| Oregon | 16.9 | 28.2 | 67 |
| Pennsylvania | 19.4 | 30.1 | 55 |
| Rhode Island | 17.7 | 32.2 | 82 |
| South Carolina | 22.6 | 33.4 | 48 |
| South Dakota | 20.8 | 26.6 | 28 |
| Tennessee | 21.7 | 33.3 | 53 |
| Texas | 23.1 | 33.7 | 46 |
| Utah | 15.9 | 22.2 | 40 |
| Vermont | 16.5 | 26.8 | 62 |
| Virginia | 21.1 | 33.5 | 59 |
| Washington | 16.8 | 29.0 | 73 |
| West Virginia | 22.8 | 35.2 | 54 |
| Wisconsin | 15.6 | 25.0 | 60 |
| Wyoming | 18.3 | 26.9 | 47 |
NOTE: The cesarean rate is the percentage of all live births by cesarean delivery.
Summary
In 2007, approximately 1.4 million women had a cesarean birth, representing 32% of all births, the highest rate ever recorded in the United States and higher than rates in most other industrialized countries (8).
From 1996 to 2007, cesarean rates increased for all women, regardless of age, race and Hispanic origin, or state of residence. In 2006, cesarean delivery was the most frequently performed surgical procedure in U.S. hospitals (9). Cesarean rates also increased for infants of all gestational ages and may be partly related to the increased rate of multiple births (7), because infants in multiple births are much more likely than singletons to be cesarean births (10). However, cesarean delivery rates for singletons increased substantially more than cesarean rates for infants in multiple deliveries (data not shown).
In addition to clinical reasons, nonmedical factors suggested for the widespread and continuing rise of the cesarean rate may include maternal demographic characteristics (e.g., older maternal age), physician practice patterns, maternal choice, more conservative practice guidelines, and legal pressures (11–13).
Definitions
Cesarean delivery: Extraction of the infant, placenta, and membranes through an incision in the maternal abdominal and uterine walls.
Cesarean rate: Number of cesarean births per 100 live births.
Race and Hispanic origin: These items are reported separately on birth certificates. Persons of Hispanic origin may be of any race. Persons of non-Hispanic ancestry are further classified by race because there are substantial differences in fertility and maternal characteristics between Hispanic and non-Hispanic persons. Persons of American Indian or Alaska Native and Asian or Pacific Islander ancestry are not classified separately by Hispanic origin because the majority of these persons are non-Hispanic. Multiple race data reported since 2003 were bridged to single-race categories for trend analysis (7).
Preterm birth rate: The number of births delivered at less than 37 completed weeks of gestation per 100 total births.
Early preterm birth rate: The number of births delivered at less than 34 completed weeks of gestation per 100 total births.
Late preterm birth rate: The number of births delivered at 34 to 36 completed weeks of gestation per 100 total births.
Rate of term and later births: The number of births delivered at 37 completed weeks of gestation and over per 100 total births.
Data source and methods
This report contains data from the Natality Data File from the National Vital Statistics System (NVSS). The NVSS includes information for all live births reported in the United States. The Natality Data File is the primary data file for analyzing birth trends and patterns in the United States. Data may be accessed from NCHS at Vital Statistics Online and VitalStats
Terms such as “higher than” and “less than” indicate statistically significant differences.
Computations exclude records with missing data.
About the authors
Fay Menacker and Brady E. Hamilton are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Vital Statistics, Reproductive Statistics Branch.
References
- Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2007 [PDF – 650 KB]. National vital statistics reports; vol 57 no 12. Hyattsville, MD. National Center for Health Statistics, Released March 18, 2009.
- U.S. Department of Health and Human Services. Cesarean childbirth. Report of a consensus development conference sponsored by the National Institute of Child Health and Human Development in conjunction with the National Center for Health Care Technology. September 22–24, 1980. NIH Publication No.82–2067. 1981.
- Yang Q, Wen SW, Oppenheimer L, et al. Association of caesarean delivery for first birth with placenta previa and placental abruption in second pregnancy. BJOG 114(5): 609–13. 2007.
- Kuklina EV, Meikle SF, Jamieson DJ, et al. Severe obstetric morbidity in the United States: 1998–2005. Obstet Gynecol. 113(2 Part 1):293–9. 2009.
- Liston FA, Allen VM, O’Connel CM, Jangaard KA. Neonatal outcomes with cesarean delivery at term. Arch Dis Child Fetal Neonatal Ed. 93(3): F176–82. 2008.
- U.S. Agency for Healthcare Research and Quality. HCUPnet. Healthcare Cost and Utilization Project: Rockville, MD. AHRQ 2005 [DRGs 370–3].
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, et al. Births: Final data for 2006. National vital statistics reports; vol 57 no 7. Hyattsville, MD. National Center for Health Statistics. 2009.
- Organization for Economic Co-operation and Development. OECD health data 2009: statistics and indicators for 30 countries. Paris, France: Organization for Economic Cooperation and Development: 2009.
- Russo CA (Thompson Reuters), Wier L (Thompson Reuters), Steiner C. (AHRQ). Hospitalizations related to childbirth, 2006. HCUP, Statistical Brief #71. U.S. Agency for Healthcare Research and Quality, Rockville, MD. April 2009.
- CDC. QuickStats: Percentage of live births by cesarean delivery, by plurality—United States, 1996, 2000, and 2006. MMWR 58(19):542. 2009.
- Williams HO. The ethical debate of maternal choice and autonomy in cesarean delivery. Clin Perinatol 35:455–62. 2008.
- Murthy K, Grobman WA, Lee TA, Hall J L. Association between rising professional liability insurance premiums and primary cesarean delivery rates. Obstet Gynecol 110(6):1264–9. 2007.
- Guise J-M, McDonagh M, Hashima J, et al. Vaginal births after cesarean (VBAC). Evidence report/technology assessment No. 71 (Prepared by the Oregon Health & Science university Evidence-based Practice Center under Contract No. 209–977–0018). AHRQ Publication No. 03–Eoi8,: Agency for Healthcare Research and Quality. Rockville, MD. March 2003.
Suggested citation
Menacker F, Hamilton BE. Recent trends in cesarean delivery in the United States. NCHS data brief, no 35. Hyattsville, MD: National Center for Health Statistics. 2010.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Vital Statistics
Charles J. Rothwell, M.S., Director
- Page last reviewed: November 6, 2015
- Page last updated: March 23, 2010
- Content source: