

Diagnostic History and Treatment of School-aged Children with Autism Spectrum Disorder and Special Health Care Needs
 ShareCompartir
ShareCompartir
On This Page
- Key findings
- One-half of school-aged CSHCN with ASD were aged 5 years and over when they were first identified as having ASD.
- CSHCN are identified as having ASD by a range of health care providers.
- Just over one-half of school-aged CSHCN with ASD use three or more health care services to meet their developmental needs.
- More than one-half of school-aged CSHCN with ASD use one or more psychotropic medications to meet their developmental needs.
- Summary
- Definitions
- Data sources and methods
- About the authors
- References
- Suggested citation
NCHS Data Brief No. 97, May 2012
PDF Version (624 KB)
Beverly A. Pringle, Ph.D.; Lisa J. Colpe, Ph.D., M.P.H.; Stephen J. Blumberg, Ph.D.; Rosa M. Avila, M.S.P.H.; and Michael D. Kogan, Ph.D.
Key findings
Data from the 2011 Survey of Pathways to Diagnosis and Services
- The median age when school-aged children with special health care needs (CSHCN) and autism spectrum disorder (ASD) were first identified as having ASD was 5 years.
- School-aged CSHCN identified as having ASD at a younger age (under age 5 years) were identified most often by generalists and psychologists, while those identified later (aged 5 years and over) were identified primarily by psychologists and psychiatrists.
- Nine out of 10 school-aged CSHCN with ASD use one or more services to meet their developmental needs. Social skills training and speech or language therapy are the most common, each used by almost three-fifths of these children.
- More than one-half of school-aged CSHCN with ASD use psychotropic medication.
Autism Spectrum Disorder (ASD) is a set of complex neurodevelopment disorders characterized by mild to severe problems in social interaction and communication along with restricted repetitive behavior patterns (1). ASD symptoms begin before age 3 years and last into adulthood, although symptoms may improve over time. There is no one best treatment for ASD, but the American Academy of Pediatrics recommends early behavioral intervention once a child is diagnosed (2). Nearly all children (94%) with ASD have special health care needs, defined as requiring health or related services beyond those required by children generally (3,4). This report provides information on diagnosis and treatment of school-aged (6–17 years) children with special health care needs (CSHCN) and ASD.
Keywords: developmental disorders, health care services, medications, Pathways to Diagnosis and Services Study
One-half of school-aged CSHCN with ASD were aged 5 years and over when they were first identified as having ASD.
- Fewer than one-fifth of school-aged CSHCN with ASD were identified as having ASD within the first 2 years of life.
- Two-fifths of school-aged CSHCN with ASD were aged 6 years and over when first identified as having ASD.
Figure 1. Percent distribution of child’s age when parent or guardian was first told that child had autism spectrum disorder among children aged 6–17 years with special health care needs and autism spectrum disorder: United States, 2011.
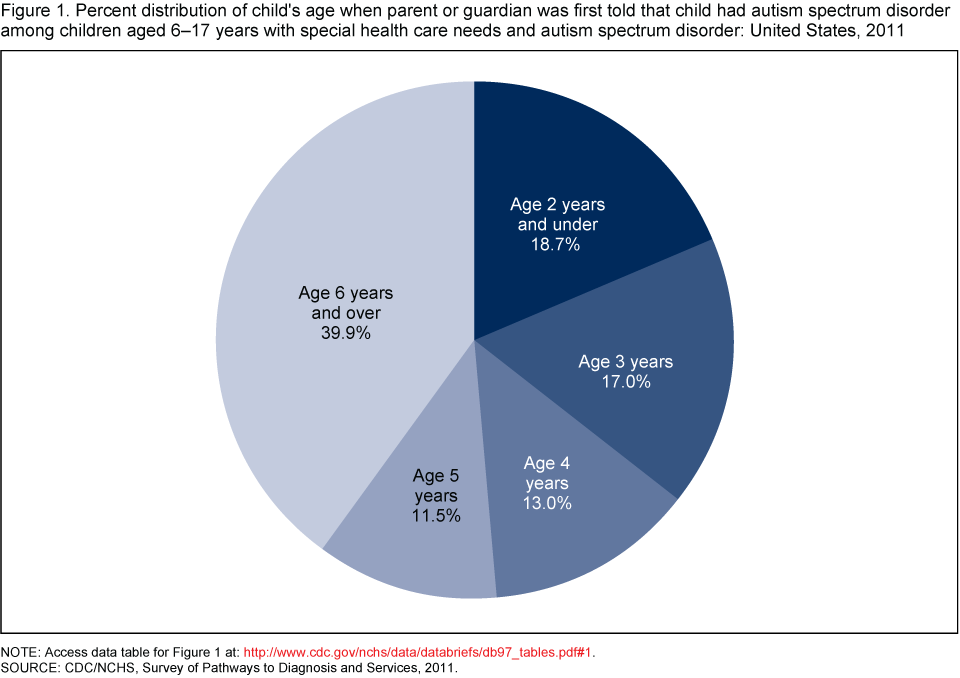
NOTE: Access data table for Figure 1 [PDF – 164 KB]
SOURCE: CDC/NCHS, Survey of Pathways to Diagnosis and Services, 2011.
CSHCN are identified as having ASD by a range of health care providers.
- School-aged CSHCN identified as having ASD before age 5 years were most often identified by generalists (such as pediatricians, family physicians, and nurse practitioners) and psychologists.
- Relative to those school-aged CSHCN identified at age 5 years and over, those identified as having ASD before age 5 years were more likely to be identified by generalists, specialist pediatricians, neurologists, and multidisciplinary teams.
- School-aged CSHCN identified as having ASD at age 5 years and over were identified primarily by psychologists and psychiatrists.
Figure 2. Percent distribution of type of doctor or health care provider who first told parent or guardian that child had autism spectrum disorder, by child’s age when parent or guardian was first told, among children aged 6–17 years with special health care needs and autism spectrum disorder: United States, 2011

1Indicates a statistically significant difference (p < .05) between age groups.
NOTES: Access data table for Figure 2 [PDF – 164 KB]. CSHCN is children with special health care needs. ASD is autism spectrum disorder.
SOURCE: CDC/NCHS, Survey of Pathways to Diagnosis and Services, 2011.
Just over one-half of school-aged CSHCN with ASD use three or more health care services to meet their developmental needs.
- Across both age groups, approximately 9 out of 10 CSHCN with ASD use one or more of the eight services included in the Pathways survey.
- Younger CSHCN with ASD are more likely than older CSHCN with ASD to use any of these eight services and to use three or more of these services.
- The most commonly used services are social skills training and speech or language therapy for both age groups.
- About 40% of school-aged CSHCN with ASD use behavioral intervention or modification services to meet developmental needs.
- Younger CSHCN with ASD are more likely than older CSHCN with ASD to use occupational therapy and speech or language therapy to meet their developmental needs.
Figure 3. Percentage of children aged 6–17 years with special health care needs and autism spectrum disorder who currently use selected health care services, by age: United States, 2011

1Indicates a statistically significant difference (p < .05) between age groups.
NOTE: Access data table for Figure 3 [PDF – 164 KB].
SOURCE: CDC/NCHS, Survey of Pathways to Diagnosis and Services, 2011.
More than one-half of school-aged CSHCN with ASD use one or more psychotropic medications to meet their developmental needs.
- More than one-half of school-aged CSHCN with ASD use at least one psychotropic medication to meet their developmental needs.
- Almost one-third of school-aged CSHCN with ASD use stimulant medications, one-quarter use anti-anxiety or mood-stabilizing medications, and one-fifth use antidepressants.
Figure 4. Percentage of children aged 6–17 years with special health care needs and autism spectrum disorder who currently use selected medication types: United States, 2011

NOTE: Access data table for Figure 4 [PDF – 164 KB].
SOURCE: CDC/NCHS, Survey of Pathways to Diagnosis and Services, 2011.
Summary
This report describes school-aged CSHCN with ASD, looking at when they were reported to be first identified as having ASD, who made the identification, and the services and medications they currently receive to meet their developmental needs. Early identification is an important first step toward making sure that children with ASD and their families are able to access and benefit from early intervention, which has been associated with positive developmental outcomes (5–7). Among school-aged CSHCN with ASD, a majority were aged 5 years and over when they were first identified as having ASD, while only one in five was identified as having ASD within the first 3 years of life. A wide range of health care providers—including general and specialist physicians, mental health specialists, and others—were the first professionals to identify CSHCN as having ASD. A majority of CSHCN recognized as having ASD at age 5 years and over were identified by psychologists and psychiatrists, whereas no one type of health care provider identified more than 20% of CSHCN recognized as having ASD before age 5 years.
Most families use a combination of services to address the developmental needs of their CSHCN with ASD. Social skills training and speech or language therapy are the most commonly used, followed by occupational therapy. Twelve percent of CSHCN with ASD do not use any of the eight services included in the survey, whereas fewer than one-half use behavioral intervention or modification services, the most well-established and efficacious intervention for ASD (2,8,9). Younger CSHCN with ASD are more likely than older CSHCN with ASD to use any services and multiple services, in part because they are more likely to use occupational therapy and speech or language therapy to meet their developmental needs. More than one-half of school-aged CSHCN with ASD use at least one psychotropic medication, with stimulants being the most common. Medication use spans a variety of medication classes, perhaps reflecting treatment of co-occurring symptoms or absence of clear practice guidelines for psychotropic medication use in children with ASD (10).
Definitions
Children with special health care needs (CSHCN): The National Survey of CSHCN (NS-CSHCN) used the CSHCN Screener (11) to identify CSHCN. This screener uses the health consequences that children experience as criteria for identifying special health care needs, rather than just specific diagnoses or health conditions.
Autism Spectrum Disorder (ASD): CSHCN were first identified as ever having or currently having ASD based on two questions on the NS-CSHCN: 1) “Has a doctor or other health care provider ever told you that [the child] had autism, Asperger’s disorder, pervasive developmental disorder, or other autism spectrum disorder?” and 2) “Does [the child] currently have autism or an autism spectrum disorder?” When recontacted to participate in the Pathways survey, parents or guardians were asked to confirm if their child ever had autism or ASD. If yes, they were then asked, “To the best of your knowledge, does [the selected child] currently have autism or an autism spectrum disorder.” This analysis is based on those CSHCN who were identified in the Pathways survey as currently having ASD.
Health care professional: Respondents were asked, “What type of doctor or other health care provider first told you that [the selected child] had autism or autism spectrum disorder?” Physician types were categorized as follows: 1) Pediatricians, family practice doctors, or other providers in general practice, which includes pediatric or family practice nurse practitioners, or physician’s assistants; 2) developmental pediatricians or other specialist pediatricians; 3) psychologists, including school psychologists or councilors; 4) psychiatrists (medical doctors); 5) neurologists; 6) a team of professionals or multidisciplinary team; and 7) specialist doctors (other than developmental pediatricians, psychiatrists, or neurologists) and other health care providers (i.e., school nurses; physical, occupational, speech, or other therapists; etc.).
Health care services: The Pathways survey asked about the following eight health care services: behavioral intervention or modification services; sensory integration therapy; cognitive based therapy; school-based occupational therapy or other occupational therapy; school-based physical therapy or other physical therapy; school-based social skills training or other social skills training; school-based speech or language therapy or other speech or language therapy; and alternative health care or treatment. For each selected service, parents or guardians were asked whether or not their child ever used the service to meet [his/her] developmental needs, and if so, whether the child currently uses the service on a regular basis.
Medication use: To determine what medication the child currently uses, the parent or guardian was asked to report “whether or not the child ever used this type of medication to meet [his/her] developmental needs,” and if so, whether the child currently uses the medication. Each type of medication was asked about separately. Specific medication names were not solicited, but if the parent knew the name of the drug but not the type, the interviewer could refer to a list of drug names matched to type of medication.
Data sources and methods
The Survey of Pathways to Diagnosis and Services is a nationally representative survey about children with special health care needs (CSHCN) aged 6–17 years ever diagnosed with autism spectrum disorder (ASD), intellectual disability, or developmental delay. The survey and this report are part of the Pathways to Diagnosis and Services Study, which was sponsored and co-led by the National Institute of Mental Health, using funds available from the American Recovery and Reinvestment Act of 2009.
Parents or guardians who previously participated in the 2009–2010 NS-CSHCN (sponsored by the Maternal and Child Health Bureau) and who reported that their child had ever been diagnosed with at least one of the three selected developmental conditions were recontacted via landline or cell telephone to participate in the Pathways survey. To be eligible, the CSHCN had to be aged 6–17 years at the time of the Pathways interview and still living in the same household as the recontacted parent or guardian. Of the parents or guardians with eligible CSHCN, 71% were successfully recontacted and 87% agreed to participate. A total of 4,032 interviews were completed from February–May 2011, an average of 9 months after the initial interview. This report presents selected measures of diagnostic history and health care experience for the 1,420 CSHCN who were reported to have an ASD at the time of the Pathways interview. (See “Definitions ” for question wording.) All estimates shown in this report are weighted to produce national estimates representative of the noninstitutionalized population of U.S. CSHCN with ASD as estimated from the 2009–2010 NS-CSHCN. The NS-CSHCN response and realization rates were about 25%; unpublished analyses suggest no significant nonresponse bias in estimates of the prevalence or characteristics of CSHCN with ASD. For more information about the Pathways survey, including questionnaire content, please visit Survey of Pathways to Diagnosis and Services website.
About the authors
Beverly Pringle and Lisa Colpe are with the National Institutes of Health’s National Institute of Mental Health, Division of Services and Intervention Research. Stephen Blumberg and Rosa Avila are with the Centers for Disease Control and Prevention’s National Center for Health Statistics, Division of Health Interview Statistics. Michael Kogan is with the Health Resources and Services Administration’s Maternal and Child Health Bureau, Office of Epidemiology and Research.
References
- Rutter M. Incidence of autism spectrum disorders: Changes over time and their meaning. Acta Paediatr 94:2–15. 2005.
- Myers SM, Johnson CP. Management of children with autism spectrum disorders. Pediatr 120(5):1162–82. 2007.
- McPherson M, Arango P, Fox H, Lauver C, et al. A new definition of children with special health care needs. Pediatr 102(1):137–40. 1998.
- Child and Adolescent Health Measurement Initiative. Query of 2007 National Survey of Children’s Health Data from the Data Resource Center for Child and Adolescent Health [Accessed 3/22/12].
- Dawson G. Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Dev Psychopathol 20:775–803. 2008.
- Guralnick MJ. Effectiveness of early intervention for vulnerable children: A developmental perspective. Am J Ment Retard 102:19–45. 1997.
- CDC. Learn the signs. Act early. Atlanta, GA: U.S. Department of Health and Human Services, CDC.
- Vismara LA, Rogers SJ. Behavioral treatments in autism spectrum disorders: What do we know? Clin Psychol Rev 6:447–68. 2010.
- Reichow B, Wolery M. Comprehensive synthesis of early intensive behavioral interventions for young children with autism based on the UCLA young autism project model. J Autism Dev Disord 39(1):23–41. 2009.
- Frazier TW, Shattuck PT, Narendorf SC, Cooper BP, Wagner M, Spitznagel EL. Prevalence and correlates of psychotropic medication use in adolescents with an autism spectrum disorder with and without caregiver-reported attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 21(6):571–9. 2011.
- Bethell CD, Read D, Stein RE, Blumberg SJ, Wells N, Newacheck PW. Identifying children with special health care needs: Development and evaluation of a short screening instrument. Ambulatory Pediatr 2(1):38–48. 2002.
Suggested citation
Pringle BA, Colpe LJ, Blumberg SJ, Avila RM, Kogan MD. Diagnostic history and treatment of school-aged children with autism spectrum disorder and special health care needs. NCHS data brief, no 97. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Edward J. Sondik, Ph.D., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Jane F. Gentlemen, Ph.D., Director
- Page last reviewed: November 6, 2015
- Page last updated: May 24, 2012
- Content source: