


Hispanic Laborer Dies after Falling through a Second Story Floor Opening in a Single Family Home under Construction - North Carolina
 ShareCompartir
ShareCompartir
NIOSH In-house FACE Report 2007-01
May 31 , 2007
Summary
On September 5, 2006, a 30-year-old construction laborer (the victim) was fatally injured when he fell through a floor opening to a concrete floor approximately 10 feet, 10 inches below. The victim had spent the majority of his work shift cutting plywood sheathing and handing it up to coworkers who were sheathing the roof. He was working from the second floor of a two-story, single-family home under construction where he and other workers had completed most, but not all, of the subfloor (plywood sheathing secured over floor joists) on previous workdays. They had left a floor area open in an attic space where a walk-in closet was to be constructed later. At the end of the shift, the victim’s lead worker asked two workers to complete the second story subfloor in the attic space. One of these workers joined the roofers to lay roofer’s felt. The other co-worker joined the victim and together, they cut two sheets of plywood sheathing and placed them over the joists in the open area in the attic space. They were not wearing fall protection. The co-worker reported that he was looking down at the sheets of unsecured plywood sheathing trying to make the pieces fit into an opening that was not square and when he looked up the victim was gone. The victim had apparently stepped onto a piece of the unsecured plywood sheathing that covered part of the floor opening, and when the plywood sheathing pivoted on the floor joist, he fell through the opening.
 |
|
Photo 1: This photograph illustrates the two-story home that workers were framing when the incident occurred |
The victim’s co-worker immediately phoned their employer who was working off-site. The victim’s employer then called the general contractor’s field manager, who was working on-site, and the field manager called 911. Emergency medical services (EMS) arrived within minutes and immediately transported the victim to an area hospital. The victim was pronounced dead in the emergency room.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
- ensure that all employees are provided with and use appropriate fall protection when exposed to fall hazards
- ensure through employee training and job-site inspection that correct construction procedures, such as use of appropriate fasteners, are followed during all phases of construction
- develop, implement, and enforce a comprehensive, written fall protection program that, at a minimum, complies with applicable OSHA fall prevention standards
- assign a competent person to inspect the worksite before work begins to identify fall hazards and to determine the appropriate fall prevention systems for workers
- ensure that all employees are provided with training in the recognition and avoidance of fall hazards and the fall protection system they are to use in the workplace where fall hazards exist, in a language and at a literacy level that all workers can comprehend.
Additionally,
- Nail manufacturers should consider color coating the body and head of nails used in pneumatic nail guns so that a specific color corresponds to a specific nail size.
Introduction
On September 5, 2006, a 30-year-old construction laborer (the victim) was fatally injured when he fell through a floor opening in a single family home under construction to a concrete floor approximately 10 feet, 10 inches below. On September 28, 2006, the North Carolina Department of Labor / Occupational Safety and Health Division (NCDOL/OSH) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), of the incident. On November 27, 2006, a DSR safety and occupational health specialist met with the NCDOL/OSH compliance officer assigned to the incident and traveled together with him to the incident site. Investigators met with the general contractor’s safety officer and with the victim’s employer and his supervisor. The house at the incident site had been completed before the DSR investigation. The house where the incident took place and a house nearby, with a floor plan and stage of construction similar to the house where the incident occurred, were examined to gain an understanding of the events that led up to the fatal fall. The police report was reviewed. The police report contained the official cause of death provided by the emergency room physician who pronounced the victim dead.
Employer
The victim’s Hispanic employer, a framing contractor, employed 7 Hispanic employees at the incident site (the number of employees varied as contracts were obtained) and had been in business for 7 years. He spoke Spanish and very limited English.
Victim
The victim was employed as a construction laborer and had worked for the company for 8 months. He had come to the U.S. from Mexico approximately 2 years before the incident and spoke only Spanish.
Employer Safety Program and Training
The victim’s employer had a general written safety and health program. The company had employed a Hispanic bilingual supervisor who was also responsible for safety. He had been employed by the company for approximately 8 months after gaining work experience in general industry. He communicated with the Hispanic framing crew in Spanish and with the general contractor’s employees in English. He trained the victim on-the-job. This training consisted of a site walkthrough and some formal training on general fall protection. There was no documentation of safety training for the employees, including the victim.
General contractor
The general contractor employed four field managers, one quality control manager, and one customer service manager, all of whom worked at the site and reported to the safety officer. The safety officer was located off-site and was responsible for several construction sites. All construction work was contracted. The general contractor provided his employees with safety and heath training and required each subcontractor to have a safety program as part of their written contract. However, due to issues of liability, the general contractor did not require contractors to provide a copy of their safety program or evaluate its components. The general contractor’s quality control manager was responsible for inspecting the quality of homes during their construction.
Incident Site
The incident took place in a two story, 2,700 square-foot, single-family home that was being constructed on a .10 acre lot in a large residential complex. Over a period of two years, 124 homes were to be built in the complex.
This was the employer’s first workplace fatality.
Investigation
On the day of the incident, the victim began work about 7:30 a.m. He was one of a crew of seven workers who were framing a new home (Photo 1). He was working on the second floor of the home for most of the day, cutting ½ inch plywood sheathing and handing it up to other workers who were sheathing the roof. A co-worker went to lunch with the victim and when they returned, the victim continued to cut plywood sheathing for the workers on the roof throughout the afternoon while the co-worker cleaned up the interior of the home.
A few minutes after 5:00 p.m., the general contractor’s quality control manager stopped by the site and went to the second floor to check the framers’ progress on the roof. At about the same time, the victim’s lead worker told the co-worker, who had gone to lunch with the victim, and another worker to go up to the second floor and finish sheathing the second floor. An opening approximately 64½ inches wide by about 12 feet long for a walk-in closet to be completed later had been left open when workers installed the subfloor on a previous workday. One of these workers went on the roof instead to lay roofing felt. According to witness statements, workers sheathing the roof were provided with personal fall arrest systems (PFAS) but workers assigned to sheathing the second floor were never told to use fall protection or provided with fall protection equipment.
The co-worker went to the second floor and joined the victim, already working on the second floor cutting plywood sheathing for the workers on the roof. They looked at the floor opening and worked together to cut pieces of plywood (uncut sheets were 48 inches wide by 96 inches long by ¾ inch thick) to make them fit. The openings were not square and required some adjustments to make the plywood sheets fit properly. The floor joists had been set 24-inches on center, creating a gap of approximately 22½ inches between joists. After two sheets of plywood sheathing had been cut and the pieces placed over the joists but not yet nailed in place, the co-worker knelt down to hold the end of one sheet of plywood, while the victim walked on the unsecured plywood sheathing to adjust it. Their intention was to adjust the dimensions of both pieces and to make them fit properly and then nail them in place. The co-worker reported that he did not see the victim fall as he was looking down at the sheet of plywood but he heard a noise that sounded like a thunder clap, and when he looked over to where the victim had been standing, he was gone. The victim had fallen through the opening to the cement floor 10 feet, 10 inches below. After the victim fell, the opening in the second floor was approximately 46½ inches wide, as one of the joists had failed and fell to the cement floor along with a sheet of plywood.
The victim’s co-worker immediately phoned his employer who was working off-site. The victim’s employer called the general contractor’s field manager, who was working on-site and the field manager called 911. The city’s highway fire and rescue were the first emergency personnel to respond (5:22 p.m.) and the Captain noted that the victim had suffered severe head injuries. Emergency medical services (EMS) arrived a few minutes later and transported the victim by ambulance to an area hospital emergency room where an emergency room physician pronounced the victim dead at 6:04 p.m.
The NCDOL/OSH compliance officer assigned to the case inspected the site the day following the incident and took photographs. He reported that it appeared that when the victim, who was not protected against falling, fell through the joist openings, his body struck one of the joists causing it to fall with him. He also reported that the ledger used to support the joist and the joist nailing appeared to be substandard; the ledger (Photo 2) had separated from the floor framing (girder) to which it was nailed, eliminating the support to the joist that failed. The NCDOL/OSH compliance officer inspected the ledger and the joists and noted that they were fastened with 8d versus 16d nails. 8d nails are 2 ½ inches long versus 3 ½ inches long for the 16d nails. The joist appeared to be adequately nailed at one end but at the other end, the nails just barely exited the joist and provided little support (Photo 3). The NCDOL/OSH compliance officer reported that although the nonstandard joist and ledger nailing could have contributed to the incident, the primary cause of the incident was walking onto unsecured plywood used to deck floor openings in the walk-in closet without wearing any fall protection.

During the FACE investigation, the DSR investigator, NCDOL/OSH compliance officer, general contractor’s safety officer, victim’s employer and the victim’s supervisor, viewed photographs of the incident that had been taken after the victim’s fall. The floor joists under the walk-in closet in the attic space were placed 24-inches on center and had been notched at one end and placed over a 2-inch by 1½ inch ledger that had been nailed in place using 8d nails. These 8d nails are used on the roof sheathing where the plywood is ¼ inch to ½ inch thick. According to the general contractor’s safety officer, the victim’s employer and his supervisor, workers had run out of 16d nails at the site on the day of the incident and used the 8d nails instead because they were available. The general contractor’s safety officer reported that the 8d nails were too short for floor decking but were on-site for roof sheathing. The DSR investigator noted that the 8d nails, in addition to being too short for the job, were nailed at an angle and not evenly placed, making them even less likely to hold. Both sizes of nails fit the pneumatic nail guns used at the site.
Following the incident, the victim’s employer made a change in work procedures and now requires his employees to stand on ladders or scaffolds placed on the first floor to install plywood sheathing over second story floor joists to create the subfloor. As a quality control measure, the general contractor chose to require metal joist hangers (Photo 4) instead of wooden ledgers for use by framing contractors as they can be secured with either 8d or 16d nails without compromising structural integrity. Both contractors suggested that it would help workers, including quality control managers, if manufacturers used a color coating on nails that corresponded to nail size.
 |
|
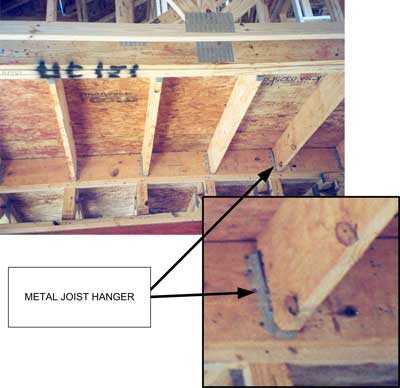
Photo 4: This photo illustrates the use of metal joist hangers (see arrow) and was taken by the DSR investigator on another house under construction at the site. |
Back to Top
Cause of Death
The emergency room physician who pronounced the victim dead reported that the cause of death was severe head trauma.
Recommendations/Discussion
Recommendation #1: Employers should ensure that all employees are provided with and use appropriate fall protection when exposed to fall hazards.
Discussion: Employers have a responsibility to identify potential fall hazards and to provide their workers with fall protection as needed. The attic floor opening presented a fall hazard. Use of appropriate fall protection, such as covering the floor opening with a properly sized cover and securing it properly until subflooring could be completed, and use of a guardrail system, safety net system, or personal fall arrest system (PFAS) while completing the floor would have protected workers against falling. Duty to provide fall protection is found in 29 CFR 1926.501 (b) (1-15)1 and requirements for fall protection systems, criteria, and practices are found in 29 CFR 1926.502.2
According to the NCDOL/OSH compliance officer, the workers were sheathing a floor and were not protected from falling through the floor joists which were set at 24" on center, creating a gap of approximately 22½" between joists. NCDOL/OSH Operational Procedure Notice 109A, Subject: Interim Fall Protection Requirements for Residential Construction,3 signed August 4, 2005, and STD 3-0.1A, Subject: Plain Language Revision of OSHA Instruction STD 3.1, Interim Fall Protection Compliance Guidelines for Residential Construction,4 June 18, 1999, are two documents that contain guidelines for employers to implement procedures that will allow workers to safely accomplish the floor sheathing activity. Appendix A to Operational Procedure Notice 109A, Subject: Interim Fall Protection Requirements for Residential Construction, provides further guidance at paragraph D.2: Working atop unsheathed floor joists. In summary, if an employee is standing or walking on floor joists, the assumption is made that they will fall to the same level on which they are standing and not incur a serious injury. In this case, the employee was not walking on the floor joist but standing on an unsecured piece of floor decking on top of the joists. The height of the top of the floor joists to the concrete floor was approximately 10 foot, 10 inches. Since the height was greater than six feet, the OPN suggests that the first row of sheathing be installed from ladders, carpenter bracket scaffolds, etc. The method used by these employees, since the roof was sheathed and the second floor minus the attic area was sheathed, was to begin the process from the nearly completed second floor. This is acceptable since the closest and most direct access to the area to be sheathed was from the same level. Two pieces of plywood were cut and the two workers proceeded to lay the plywood sheathing over the floor joists in the attic area. According to the NCDOL/OSH compliance officer, at this point in the floor sheathing, the workers departed from safe work practices and stepped on unsecured plywood. Direction in OPN 109A suggests that once the first row of sheathing is down and properly secured, workers climb atop the sheathing and continue with the second row. The two workers walked onto the unsecured plywood with the intention of adjusting them on the joists and then nailing them to the joists. The victim’s coworker was in the corner adjusting one piece of plywood while the victim walked onto the other piece of plywood. Neither worker was wearing any type of personal fall arrest system (PFAS). Following the suggestion in the North Carolina Operational Procedure Notice (OPN) 109A, anchorage points should have been placed in appropriate locations for employees to use PFASs (i.e. harnesses with retractable rope grabs) while completing the sheathing operation.
Recommendation #2: Employers should ensure through employee training and job-site inspection that correct construction procedures, such as use of appropriate fasteners, are followed during all phases of construction.
Discussion: In the area where the incident occurred, the open area to be filled with plywood was reportedly out of square and required some extra work to make the pieces of plywood fit. In addition, a floor joist and a section of ledger were nailed in some places with nails that were too short and sometimes nailed at an angle that made the length of nail entering the girder very short. When the nails pulled out of the girder, the joist and ledger gave way. The joist failed and fell to the floor. Employers should conduct inspections to ascertain levels of employee expertise and then provide basic skills training to ensure that work is performed correctly, substandard work is corrected, and that safety is not compromised.
Additionally, employers should also ensure that sufficient supplies, such as correct size nails, are available to workers and that workers are instructed to stop work and wait for the correct size nails for the job if they run out. Nail guns are made to adjust to several nail sizes but employers should consider labeling the nail guns at the worksite with the correct size nail for the job, for example use one gun and label it 16d for floor joists. Label and use a second gun 8d and use it to secure the ½ inch sheathing on the roof. This may help remind workers of the importance of using the correct nail for the job.
Following the incident, the general contractor chose to require the use of metal joist hangers (Photo 4) instead of wooden ledgers for hanging floor joists. The general contractor determined that although joist hangers are more expensive, they are more efficient and require less skill to install, and can be nailed in place using either 8d or 16d nails.
Recommendation #3: Employers should develop, implement, and enforce a comprehensive, written fall protection program that, at a minimum, complies with applicable OSHA fall prevention standards.
Discussion: Although the employer had developed a general safety program, it had not been implemented at the time of the incident. A comprehensive written fall prevention program is part of an employer safety program and should be written in compliance with 29 CFR 1926.500 Subpart M.5 The fall prevention program should be implemented and enforced before workers are assigned to tasks where there is a potential for fall hazards.
Recommendation #4: Employers should ensure that all employees are provided with and use appropriate fall protection when exposed to fall hazards.
Discussion: According to OSHA, a competent person is one who can (1) identify existing and predictable hazards in the surrounding or working conditions that are unsanitary, hazardous or dangerous to workers , and (2) is authorized to take prompt corrective measures to eliminate them [29CFR 1926.32].6 In this incident the competent person would have been responsible for ensuring that appropriate fall protection was available and correctly used to protect workers from falling through the floor opening in the attic space. Additionally, the competent person, by virtue of specialized training in fall hazards, would be expected to recognize the hazards associated with workers using unsecured floor decking as a walking/working surface, stop the practice, and educate workers about this unsafe and unacceptable practice.
Recommendation #5: Employers should ensure that all employees are provided with training in the recognition and avoidance of fall hazards and the fall protection system they are to use in the workplace where fall hazards exist, in a language and at a literacy level that all workers can comprehend.
Discussion:In this instance, the victim and his co-workers had completed most, but not all, of the second floor sheathing before the day of the incident. However, the floor in the attic area had been left open and workers were directed by their lead worker to finish decking the floor just before the end of the work shift on the day of the incident. The quality control manager who worked for the general contractor had been on the second floor several minutes before the incident to check on the progress of the work, but it appears that none of these employees recognized the fall hazard. All employers should provide training to workers who may be exposed to a fall hazard. The training should enable each worker to recognize fall hazards and the procedures to follow for minimizing these hazards. OSHA standard 29 CFR 1926.5037 requires that worker training in fall protection be provided by a competent person that is qualified in many areas of fall protection. The areas of expertise in fall protection that pertain to this incident, for example would include, at minimum, the following elements:
- Identification and description of fall hazards in the work area.
- Correct procedures for erecting, maintaining, using, disassembling, and inspecting fall prevention systems to be used (such as covers, guardrail system, PFAS, etc.).
- The use and operation of the fall protection system to be used.
- The role of employees in fall protection plans.
- The applicable OSHA standards contained in subpart M, including, for example, requirements for standard guardrails, covers, screens, or PFAS to prevent falls.
In addition, training should be provided using a language and literacy level that all workers can comprehend so that all workers have an opportunity to learn how to protect themselves from hazardous situations.
Additional useful information for safety training for workers who work around fall hazards can be found in the NIOSH publications entitled Worker Deaths by Falls8 and in NIOSH Alert: Preventing Falls of Workers through Skylights and Roof and Floor Openings.9 The Worker Deaths by Falls publication can be found at the NIOSH web site at https://www.cdc.gov/niosh/docs/2000-116. The NIOSH Alert can be found at https://www.cdc.gov/niosh/docs/2004-156 . The Alert is available in both English and Spanish and contains a tear-out sheet (PDF format) that summarizes safety precautions that workers should take to protect themselves from falls through skylights and roof and floor openings. Posting this tear-out sheet at the worksite may serve as an additional means of communicating safe work procedures to workers. Employers can call the NIOSH publications office at 1-800-356-4674 to obtain a paper copy of each NIOSH publication.
Recommendation #6: Nail manufacturers should consider color coating the body and head of nails used in pneumatic nail guns so that a specific color corresponds to a specific nail size.
Discussion: Color coating the body and heads of nails used in pneumatic nail guns would provide an additional message to workers regarding nail choice. For example, orange could be used for 8d nails only to be used for sheathing roofs and black could be used for 16d nails only to be used for sheathing floors and fastening joists and ledgers. Color coating the head as well as the body of the nail would also help employees working in quality control as they would be able to see the color of the nail head after jobs had been completed and determine, by comparing the nail head color with the nail size required for the job, if the correct nail size had been used.
References
- Code of Federal Regulations [2006]. 29 CFR 1926.501. Duty to have fall protection. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2006]. 29 CFR 1926.502. Fall protection systems criteria and practices. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- NCDOL/OSHA [2005]. Operational Procedure Notice 109A Subject: Interim Fall Protection Requirements for Residential Construction. Raleigh, NC: North Carolina Department of Labor/Occupational Safety and Health.
- OSHA [1999]. STD 3-0.1A Plain Language Revision of OSHA Instruction STD 3.1, Interim Fall Protection Compliance Guidelines for Residential Construction. Washington, DC: Occupational Safety and Heath Administration.
- Code of Federal Regulations [2006]. 29 CFR 1926.500. Subpart M Fall Protection. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2006]. 29 CFR 1926.32 (f). Competent person. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations [2006]. 29 CFR 1926.503. Training requirements. Washington, DC: U.S. Government Printing Office, Office of the Federal Register.
- NIOSH [2000]. Worker Deaths by Falls. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health , DHHS (NIOSH) Publication No. 2000-116.
- NIOSH [2004]. Alert: Preventing Falls of Workers through Skylights and Roof and Floor Openings. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health , DHHS (NIOSH) Publication No. 2004-156.
Investigator Information
This investigation was conducted by Doloris N. Higgins, Safety and Occupational Health Specialist, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research, National Institute for Occupational Safety and Health. The NIOSH FACE Program and the safety and occupational health specialist would like to acknowledge the NCDOL/OSH Compliance Officer for assistance in this investigation.
Back to Top
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research