


Career Fire Fighter Dies While Diving for a Civilian Drowning Victim - Rhode Island
 ShareCompartir
ShareCompartir
 Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
Death in the Line of Duty...A summary of a NIOSH fire fighter fatality investigation
F2008-32 Date Released: October 8, 2009
SUMMARY
On August 3, 2008, a 52-year-old male fire fighter (the victim) died while diving during a search for a civilian drowning victim. The victim was found unconscious on the surface of the lake after he had descended in SCUBA gear trying to locate the civilian drowning victim. The victim was off-duty and had responded to the scene in his personal watercraft with his personal dive gear. The local fire department had already rescued one civilian from the surface of the lake using a fire department boat and had marked the approximate location of the recovery with a buoy and anchor. A civilian boat was utilized to transport the surviving civilian to a local marina while the fire department boat remained on the scene performing a surface search for the second civilian. The victim arrived on the scene, and after a brief conversation with the fire fighters on the boat, began his dive in the area of the buoy. The fire fighters on the boat observed the fire fighter descend and then communicated to divers arriving by another fire department boat that there was a diver under the water in the area of the buoy. The arriving divers observed the buoy and another object floating in the water in the area of the buoy and recognized that object as a divers tank valve. After determining that the tank valve was the victims, the divers tried to communicate with the victim and discovered he was unconscious, facedown with his regulator out of his mouth. A Mayday was radioed for a diver in distress and divers entered the water and were able to place the victim in an inflatable boat that was delivering additional divers to the scene. Resuscitation efforts were initiated and continued during transport to shore. The victim was transported to a local hospital where he was pronounced dead. Key contributing factors identified in this investigation include: inadequate capacity of the fire department to lead and conduct a technical rescue SCUBA diving operation, insufficient training and experience of the victim to participate in a technical rescue diving operation, and the victims physical health and condition which increased risks for an adverse health outcome.
NIOSH investigators concluded that, to minimize the risk of similar occurrences, fire departments should:
- ensure that an effective incident management system is in place that supports technical rescue operations
- ensure that public safety divers are properly trained, equipped, and supported to perform public safety diving responsibilities
- ensure that a safety officer properly trained in the technical rescue field being performed is on scene and integrated into the command structure
- ensure that standard operating procedures regarding technical rescue capabilities are in place and enforced for all levels of water rescue specialty areas including SCUBA diving
- ensure a comprehensive risk-benefit program is in place prior to participating in specialty areas including technical rescue professional level operations
- ensure that programs are in place to provide for training and equipment (including vessels) expected for water rescue and the inspection, maintenance, testing, and replacement of water rescue equipment including SCUBA gear
- provide annual and periodic health, wellness, and fitness examinations with specific medical evaluations for fire fighters expected to perform technical rescues such as SCUBA diving
- adopt the International Association of Fire Chief’s Zero-Tolerance Policy for Alcohol and Drinking to prohibit the use of alcohol by members of any fire or emergency services agency/organization at any time when they may be called upon to act or respond as a member of those departments. Departments should develop written policies and have procedures in place to enforce this policy
Additionally, the following recommendations are preventative measures recommended by other fire service groups to reduce cardiovascular events among fire fighters. Fire departments should consider:
- phasing in a mandatory wellness/fitness program for fire fighters to reduce risk for cardiovascular disease and improve cardiovascular capacity
- performing a preplacement and an annual physical performance (physical ability) evaluation for all fire fighters to ensure they are physically capable of performing the essential job tasks of fire fighting
- ensuring that physicians are knowledgeable about the physical demands of fire fighting and the components of NFPA 1582 and the additional medical and physical requirements of performing technical rescuer SCUBA diving
INTRODUCTION
On August 3, 2008, a 52-year-old male fire fighter (the victim) died while SCUBAa diving during a search for a civilian drowning victim. On September 16, 2008, the chief of the involved department requested NIOSH to assist in an investigation of the incident. On October 69, 2008, two safety and occupational health specialists from the NIOSH Fire Fighter Fatality Investigation and Prevention Program (FFFIPP) traumatic injury component in Morgantown, WV, and an investigator from the FFFIPP cardiovascular disease component located in Cincinnati, Ohio, traveled to Rhode Island to investigate the incident. The NIOSH investigators met with the fire chief and fire fighters from the victims department, the police chief and detectives from the local police department, and divers from other local fire departments. Medical records were obtained from local medical providers, and contact was made with the medical examiners office that performed the examination of the victim. NIOSH investigators reviewed the departments SOPs related to water rescue and incident command; the victims fire fighting training records, SCUBA diving certificate, and water rescue training records (no other training data or SCUBA dive logs or dive computer information for the victim were available); witness statements; and the 911 dispatch tapes. Investigators visited the incident site and performed an inventory and took photographs of the victims dive gear at the police departments evidence room. The victims dive gear remained in the custody of the local police department after the incident and during the site visit. An evaluation of the victims dive gear was later performed by a private forensic casualty investigation firm that specializes in SCUBA diving casualty investigations.
a Self-contained underwater breathing apparatus (SCUBA) is an underwater breathing system where the inspired gas is delivered by a demand regulator and exhaled into the surrounding water (open circuit), and the gas supply is carried on the divers back (NOAA Diving Manual)1
FIRE DEPARTMENT
The department involved in this incident is a career fire department consisting of 32 members with 3 fire stations and serves a population of 17,000 residents in an area of 34 square miles. The department has a mutual aid agreement with neighboring departments for fire and rescue incidents. The department allows off-duty fire fighters to be placed back on duty during emergency incidents at the discretion of the chief.
The department is located near a busy harbor and has many bodies of water in their response area including shipping channels to the ocean, commercial waterways, canals and lakes. The department responds to approximately 12 marine/water rescue incidents per year. The department provides emergency water rescue services through fire department response with a 13-ft utility boat on a trailer housed with an engine company and has access to a larger boat through an agreement with the harbor master agency.
Training/Experience
The victim in this incident had approximately 25 years of experience as a professional fire fighter with this department. The victim held a certification as an emergency medical technician for the state of Rhode Island in addition to Hazardous Materials Operations Level and Fire Fighter Level 1 from the Rhode Island Fire Academy. In 1982 he was certified as an open-water diver through the National Association of Underwater Instructors. The victim did not have a dive computer on the day of the incident and diver logbook(s) were not provided to assess dive experience. The victim did not have documented training or certification in public safety diving.
The department had standard operating procedures regarding water rescue and boat usage and conducted frequent training on subjects such as ice rescue and small boat handling. Department SOPs were limited to surface water rescues. The incident commander and L-1 officer had experience in surface water rescue but lacked training on public safety diving oversight. The department did not have a formal or recognized technical rescue SCUBA diving team, and relied on mutual aid divers to perform technical rescue SCUBA diving resources through a formal mutual aid agreement.
SCUBA EQUIPMENT
The SCUBA equipment used by the victim in this incident was personally owned by the victim. After the incident, the equipment was taken to the local police department and stored under orders from the fire chief. NIOSH investigators examined the equipment and recommended that the equipment be evaluated by a qualified laboratory to determine working order.
The following equipment was present and examined and photographed by NIOSH investigators at the local police department evidence room:
- 1 open-circuit SCUBA demand regulator,b having a single intermediate pressure hose with first-stage pressure reduction at the yokec (cylinder attachment) and second-stage regulator at the mouthpiece. The first-stage regulator and yoke were found mounted on the tank valve upside down (see Photo 1) resulting in the primary second-stage and octopus regulators presenting over the left side of the victim instead of the normal profile of having the regulators on the right side of the diver.
- 1 octopus rigd
- 1 depth and pressure gauge pack (depth gauge did not have a maximum-depth indicator)
- 1 buoyancy compensator device (air bladders empty)
- 1 80-cubic feet, 3000-psi aluminum dive cylinder (empty). The cylinder had a mark indicating that the last hydrostatic test on this cylinder was performed on June 2006.
- 1 SCUBA mask (Lens was broken after the victim had been recovered.)
b A demand regulator is an apparatus in which the gas supply is activated by the negative pressure associated with inhalation.
c A yoke is a device for attaching the regulators to the cylinder(s) in order to make a leak-proof seal.
d An octopus rig is a single-hose regulator with an extra low-pressure port where an additional second-stage regulator has been provided for emergency buddy-breathing air supply or in case of primary second-stage regulator failure.
The victims weight belt was not recovered from the lake after being jettisoned by rescue divers. Investigators could not determine how much weight the victim was wearing. The victim did not have any thermal protection and did not have fins when he entered the water. The victim attempted to perform the dive without fins and likely would have had difficulty being able to move any distance, maintain buoyancy, or navigate underwater without having donned fins in open water such as this lake. The victims air supply was reported as 700 psi at the point when the rescue divers removed him from the water. His total downtime was reported to be a few minutes, and the low volume of remaining air would call into question the thoroughness of an equipment precheck. The victims first-stage regulator was found to be attached to the cylinder valve upside down (see Photos 1, 2) causing the profile of the primary second stage regulator and the octopus to be on the left side of the victim instead of the right. The open circuit SCUBA regulator that the victim was using had a standard 2nd stage mouthpiece and the regulator first stage should have been mounted so the second stage hose leads to the right and over the right shoulder of the diver. PADI Open Water Diver Manual2 states, the second-stage hose always goes over the right shoulder. This also resulted in the intermediate-pressure hose for the auto inflator profiling off of the victims right side, resulting in an across-the-chest attachment point to the auto-inflator low pressure hose on the buoyancy compensator (BC) vest (see Photo 1). The mouthpiece of the primary regulator would have been in an upside-down configuration and presenting in an unconventional and possibly confusing manner. The auto-inflator button on the BC vest would not have been in the correct position due to it being pulled to the divers right side. If the diver had experienced an unmanageable problem under the water and tried to locate the auto-inflator button to add air to his BC, the button might not have been located easily. The victim was found on the surface and some air was in his BC vest, but his weight belt had not been jettisoned which would have been one of a series of emergency procedures to ascend to the surface.
NIOSH investigators recommended that the department ship the victims SCUBA gear to a qualified independent test facility to examine and provide an evaluation report. The department sent the gear to a private forensic casualty investigation firm and an equipment evaluation was performed. The evaluation report noted the following:
- Equipment inspected was in fair to poor condition.
- Air gas sample showed an excess level of carbon dioxide gas. The gas sample test revealed 1991.99 ppm of carbon dioxide gas. Concentrations greater than 1000 ppm exceed the Compressed Gas Association (CGA) Grade E standard. Increased concentrations of carbon dioxide may have an adverse effect to SCUBA divers.
- The configuration of the air delivery system was rotated 180° from normal, resulting in the attached hoses presenting in an unconventional and possibly confusing manner.
- The SCUBA cylinder was within current hydrostatic test date, however the sticker evidencing a visual inspection expired the last day of May 2008.
- The air delivery system and its components showed a moderate level of corrosion. The first stage showed a moderate level of corrosion at the air filter.
- The primary second stage and alternate second stage both functioned as designed and were within manufacturers specifications, however, each second stage mouthpiece had a tear which could cause water intrusion into the path of airflow when used by a diver.
- The buoyancy compensator (BC) was in poor condition. The BC large bore inflation hose contained a tear which prevented the BC from holding air as designed and therefore failed the function test.
- The subject SCUBA equipment presents with several deficiencies rendering it unsafe for use, however, we cannot at this time directly attribute this SCUBA divers death to any of the aforementioned deficiencies.
WATER AND WEATHER CONDITIONS
The lake involved in this incident was approximately 476 acres with a maximum depth of 25 feet. The shoreline was composed of boulders and rocks with the bottom of the lake reported as layered silt and boulders. Surface water temperature was not reported but divers experienced a thermoclinee under under the surface. The water temperature at depth was not reported and visibility was reported to be between 0 to 3 feet at different depths.
Weather conditions on the day of the event were reported as
- air temperature of 71-76°F.
- winds from the northwest at 1 mph to 5 mph.3
- fire fighters reported during interviews that a strong thunderstorm was affecting the lake at the time of the initial rescue call and continued with heavy downpours during initial operations of fire department units arriving on scene.
e A thermocline is an abrupt change in temperature encountered at varying depths.
INVESTIGATION
At 1856 hours, on August 3, 2008, the local fire department was dispatched during a severe thunderstorm to a water rescue incident at a local lake for a reported drowning. The dispatched units were Engine 3, Rescue 1 (ambulance), Rescue 2 (ambulance), Squad 1, and Car 1 (chief of the department). Squad 1 responded with Marine 2 (a 13-ft utility boat used for water rescue stored at a station staffed with three personnel). The fire department responded to the emergency incident with their fire-rescue boat towed behind a support vehicle. The fire-rescue boat could not be observed in the mirrors of the support vehicle (due to the width of the tow vehicle), and the driver of the support vehicle had to open the rear doors to see the boat and trailer. The boat and trailer were not able to be backed down the boat ramp, and fire fighters had to move the boat and trailer by hand to launch the boat resulting in a delay in getting the boat launched. The fire-rescue boat was not equipped with water rescue gear such as throwable rescue devices and boarding ladders, but was equipped with personal flotation devices for the fire fighters.
Fire fighters from Squad 1 launched Marine 2 at a local ramp (see Photo 3), and then three fire fighters boarded Marine 2 and began trying to locate the victims on the lake. Marine 2 spotted a small aluminum boat with no one on board and a life jacket hanging on a fishing pole in the rear of the boat. The three fire fighters then saw a female in the water frantically waving. The crew rescued the female civilian and learned from her that there was another civilian, a male, who fell or jumped from the boat and was under the water. Marine 2 then transferred the female to another civilian boat and instructed them to take her to shore. One of the three fire fighters from Marine 2 was placed on another civilian boat to assist with search patterns, while Marine 2 obtained a small fender (air-filled bumper used for mooring protection between a boats hull and other boats or a dock) from the civilian boat and tied it to Marine 2s anchor to mark the spot where they had picked up the female civilian.
The trolling motor on the civilians aluminum boat had remained engaged, and the boat had motored away from the area on the lake where the female civilian was rescued. Marine 2, with two fire fighters, then started a series of surface search patterns to try and locate the male civilian.
Marine 2 was in radio communication with the chief of the department who had arrived on the scene and established command at the boat ramp. The chief requested mutual-aid assistance from three neighboring water rescue/dive teams and asked that they respond to the command post. The responding resources included five members of local fire department dive teams in addition to two more rescue boats. The chief requested all responding dive team members and resources to respond to the command post at the boat ramp to organize the dive team operation. All of the mutual-aid dive team members responded to the command post. Command advised Marine 2 that two divers were on their way out to their location on the lake and directed Marine 2 to meet the divers, show them the location, then return to the boat ramp and pick up three more divers. Command requested a helicopter from the U.S. Coast Guard to provide an aerial search of the lake.
The fire fighter (victim) was off duty but in the area and communicated via portable radio with the chief that he could be out there with my diving stuff if you want. Command advised him if he wished to that would be great. The victim then radioed command that he was on a jet ski and could be there in no time at all. Command advised the victim by radio to come to the command post at the boat ramp so we can keep track of everybody. The radio message from command was acknowledged by the victim over the radio. The victim later radioed command that he was heading out there right now and asked command for the location. Command radioed back to the victim asking his location. The victim radioed back that he was in the middle of the pond. Command then advised the victim to assist L-1 (officer) on Marine 2. That transmission was not acknowledged by the victim. Communicating with Marine 2, the victim tried to find the fire department boat among other boats on the lake.
The mutual-aid boat had been launched with two divers and had left the boat ramp en route to Marine 2s location. Command then radioed Marine 2 that two divers were en route and directed Marine 2 to return to the ramp after the mutual-aid boat with divers arrived at Marine 2s location. Command advised that he had four or five more divers that Marine 2 needed to transport back out to the scene. Command then advised Marine 2 that a second mutual-aid boat was on its way out from the ramp with additional divers. Marine 2 advised command that they had made contact with the first mutual-aid boat and that they were going to start diving with two divers, and that the victim had his dive gear and was with them. Marine 2 also reported that they were on their way back to pick up the second crew.
The victim arrived on his personal watercraft with his dive gear and contacted L-1 (the officer) on Marine 2. The Lieutenant and fire fighter on Marine 2 stated during interviews that the victim asked them where the civilian was and stated I can get him. L-1 reportedly advised the victim No, wait, the divers are on their way out. Talk with them to see what your plan is going to be. The victim reportedly responded No, Im going to stay right near the buoy. L-1 then reportedly told the victim Its been almost an hour, dont bother, wait for [mutual-aid divers]. The fire fighter on the boat reportedly also urged the victim not to go in but to wait on the other divers. The victim reportedly then stepped off his personal water craft with his SCUBA dive gear on (no fins) and submerged under the water.
The mutual-aid dive boat was approaching the scene and was met by L-1 in Marine 2. L-1 notified them of the diver (victim) in the water around the buoy. The dive leader asked who the diver in the water was, and after a short conversation with L-1, the dive team started to get ready to put their divers in the water while Marine 2 returned to the command post to pick up more divers. The mutual-aid dive boat motored slowly toward the buoy and noticed what they originally thought was another buoy floating in the water. They then realized it was a SCUBA tank valve and thought that the diver was on the surface looking down into the water. As they approached the diver, they struck the water with oars and made noise to try and gain his attention. The victim did not respond and the mutual-aid boat placed two divers in the water to rescue the victim. The victim was found face down in the water, unconscious with his second-stage regulator out of his mouth. A Mayday was transmitted for a diver in distress and additional divers were dispatched to assist along with Marine 2, which was turning around to return to the scene.
After jettisoning the victims weight belt, the rescue divers initially tried unsuccessfully to get the victim into the rigid hull of the mutual-aid boat. An arriving inflatable-hull boat was called over to remove the victim and his gear from the water. The victim was placed in the inflatable boat and resuscitation efforts started while the boat transported the victim to shore. The victim was transported by a rescue unit (standing by, on the scene) to a local hospital where he was pronounced dead.
The male civilians body was located on the lake bottom the following day by Rhode Island State Police using a side-scan sonar unit. State police divers then performed a SCUBA-dive operation and recovered the body from the lake.
CONTRIBUTING FACTORS
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following items as key contributing factors in this incident that ultimately led to the fatality:
- Inadequate capacity of the fire department to lead and conduct a technical rescue scuba diving operation
- Insufficient training and experience of the victim to participate in a technical rescue diving operation
- The victims physical health and condition which increased risks for an adverse health outcome.
CAUSE OF DEATH
The cause of death was reported by the medical examiner as probable cardiac arrhythmia in a person with hypertensive cardiovascular disease in the setting of acute ethanol intoxication.
MEDICAL FINDINGS
The death certificate and the autopsy, completed by a medical examiner, listed as the cause of death probable cardiac arrhythmia in a person with hypertensive cardiovascular disease in the setting of acute ethanol intoxication. Acute blood ethanol level was reported as 0.25%. Rhode Island state law defines legal intoxication at 0.08%. Pertinent findings from the autopsy include cardiomegaly (enlarged heart), left ventricular hypertrophy, minimal coronary artery disease, no coronary artery blood clot, and no pulmonary embolus.
The victim was 66 inches tall and weighed 179 pounds, giving him a body mass index (BMI) of 28.9. (A BMI of 25.029.9 kg/m2 is considered overweight.4) In 1992, the victim was diagnosed with hypertension (high blood pressure) and was prescribed a blood pressure-lowering medication. In 2003 an additional antihypertensive medication was prescribed. In 2006, the victim was medically cleared by his primary care provider for a commercial drivers license to drive trucks. He did not report heart-related symptoms (chest pain, chest pressure, angina, shortness of breath on exertion, etc.) to his physician, his family, or the fire department.
Cardiovascular Disease. The autopsy showed the fire fighter had minimal cardiovascular disease, therefore it is very unlikely the victim suffered a heart attack. More likely, as noted by the medical examiner, the victim experienced primary cardiac arrhythmia.
On autopsy, the victim was found to have left ventricular hypertrophy (LVH) and an enlarged heart (cardiomegaly). These findings were not identified prior to his death. Hypertrophy of the hearts left ventricle is a relatively common finding among individuals with long-standing high blood pressure, a heart valve problem, or chronic cardiac ischemia (reduced blood supply to the heart muscle).5 The victims 16-year history of high blood pressure was probably responsible for his LVH. Both LVH and cardiomegaly increase the risk for sudden cardiac death.6
RECOMMENDATIONS/DISCUSSIONS
Recommendation #1: Fire departments should ensure that an effective incident management system is in place that supports technical rescue operations.
Discussion: In the initial stages of a technical rescue, it is not uncommon for the incident commander to be playing catch-up implementing span of control and unity of command measures while expanding the command structure until enough management resources arrive on scene. An effective incident management system has two components: (1) the roles and responsibilities to be assumed by responders and (2) standard operating procedures to be used in the management and direction of emergency incidents and other functions.7 The incident management system should be tailored to the departments resources and the likely types of response needed in the jurisdiction. Personnel should be thoroughly trained in and understand the incident management system and how they are to operate within the incident action plan. In his book, Fire Department Safety Officer 2nd ed.,8 Chief Dodson defines freelancing as a failure to work within the framework of an incident action plan. Fire fighters have been killed and seriously injured while engaged in a freelance operation, that is, an operation or task being performed unknown to the incident commander or other working crews. Responders should understand that the check-in process allows incident command to maintain accountability and to ensure the safety of all responders.
In this incident, the chief of the department established command early in the incident at the boat ramp. The rescue boat and subsequent dive operation were not in view of or able to be easily controlled by the incident commander. A division-level officer on the dive site (or rescue boat) could have provided the incident commander with a more manageable span of control and unity of command functions. The fire department involved in this incident had standard operating procedures (SOPs) for water rescue but no SOPs for public safety SCUBA diving operations or guidelines on coordination with mutual-aid dive teams. The victim responded to the scene and was placed on duty as is the practice with this department concerning off-duty response and participation on emergency incidents. Although the victim checked in with command via a portable radio, and was told by command to respond to the command post, command reportedly did not know that the victim had entered the water until after being told by L-1 on Marine 2. If the victim had responded to the command post as instructed, the command staff could have had an opportunity to evaluate his fitness for duty. Departments should have clear SOPs for personnel accountability and members should understand how the check-in process is an important component of accountability.
Recommendation #2: Fire departments should ensure that public safety divers are properly trained, equipped, and supported to perform public safety diving responsibilities.
Discussion: Public safety agencies that perform technical rescue water operations, including SCUBA diving, need to ensure that personnel receive the proper training, equipment, and continued support consistent with national consensus standards and agencies that provide recognized advanced levels of certification to safely perform this level of emergency service capability. Although recreational SCUBA diving certification programs provide a level of training that is fine for the recreational SCUBA diving community, these programs are not commonly designed for the extreme hazards regularly encountered with public safety water rescue and diving. According to NFPA 1006 Standard for Technical Rescuer Professional Qualifications, 2008 edition, annex A,9 The committee is of the opinion that Advanced Open Water certification provided by most nationally recognized certifying agencies (agencies associated with the Recreational SCUBA Training Council) build an acceptable foundation for the basic SCUBA skills required for dive technical rescuer. These courses do not, however, offer all of the skills required to meet these standards, and further training and experience in special hazards expected to be encountered in the AHJs, territory should be sought. In his book Dive Rescue Specialist, Operational Training for Public Safety Divers,10 author Steve Orusa notes, Inadequate SCUBA skills may be the leading cause of public safety diver accidents. In many cases, a problem developed that the diver was unable to solve due to a basic skill level. In most cases, divers had received either insufficient or nonexistent SCUBA skills refresher training after initial certification. Public safety divers should have training and experience in a variety of environments likely to be encountered in rescue operations such as, ice, current, hazardous materials, dry suit, and lifting operations.
Public safety SCUBA diving is a technical skill that greatly exceeds recreational SCUBA certification levels. Annual confirmation of these skills should be performed to ensure continued competency. The level of knowledge, skills, ability, equipment and support required for a public safety SCUBA diver are outlined in NFPA 10069, and NFPA 1670 Standard on Operations and Training for Technical Search and Rescue Incidents, 2009 edition.11 Public safety diving requires emergency response teams with specific knowledge, skills, ability, equipment and continued support beyond basic fire fighter or emergency responder requirements to resolve unique or complex rescue situations. The dive team needs to stay current on training and annual skills evaluation. An example of an evaluation form to assess skills of public safety divers is provided in Appendix 1. Technical rescue SCUBA dive teams need to stay current on new equipment available such as in mask communications and protective gear such as dry suits and redundant air supply options. Continued support for the team is an important component of the leadership of technical rescue teams. Once a team is properly trained and equipped, the organization must continue to provide support to maintain the technical rescue teams operational readiness through continued training and review of program goals and needs. Inadequately trained divers should not be allowed to participate in technical rescue SCUBA diving incidents beyond their level of training.
In this incident, the victim held a recreational open water SCUBA diving certificate. This level of training is for recreational SCUBA diving and the training is limited to the level of training received at the time of the certification, which in this case, was more than 25 years ago. The attempted underwater rescue of the civilian was likely beyond the victims documented training and ability. Despite the certified training, the victim was not properly equipped to safely perform an underwater operation. The victims personally owned SCUBA equipment was evaluated and found to be in fair to poor condition and the breathing air would not have passed the CGA Grade E standards due to an excess of carbon dioxide gas.
Recommendation #3: Fire departments should ensure that a safety officer properly trained in the technical rescue field being performed is on scene and integrated into the command structure.
Discussion: Safety officers assigned to special operations incidents need to have the expertise in the specific technical rescuer field to effectively evaluate hazards and provide direction with respect to the safety of all personnel. A qualified fireground safety officer might not possess the expertise in water rescue or public safety diving and, therefore, might not recognize or understand capabilities of the team members, limitations and hazards to divers, problems with equipment, or performance issues of personnel. NFPA 1521 Standard for Fire Department Safety Officer, 2008 edition,12 notes, in cases where the designated ISO does not possess the technician-level training, appointing a technician level trained assistant or technical specialist with the necessary training will help satisfy the (safety) needs of the technician-level members.
Recommendation #4: Fire departments should ensure that SOPs regarding technical rescue capabilities are in place and enforced for all levels of water rescue specialty areas including SCUBA diving.
Discussion: Public safety diving operations are extremely complex and involve a tremendous amount of risk, but those risks can be eliminated, avoided, shared, or mitigated. A high proportion of dive operations can be categorized as high-risk/low-frequency events. Most agencies dont have enough water rescues or enough of the same type of water rescues to rely on call volume to prepare divers to perform safely and effectively. This makes preparation and training critical to safety and effectiveness. As in other special operations, risk management is a part of public safety diving operations.10 The safe and effective rescue or recovery of a water incident victim is dependent on a well coordinated relationship with other agencies sharing responsibility for providing service. Joint training exercises and scenario based training identifies the strengths and weaknesses in the response and provides areas to improve safety and effectiveness. Once identified, they can be cooperatively addressed by all agencies. Each team responding needs consistent standard operating procedures.
In this incident, the local fire department did have an SOP for water rescue (surface rescue), but did not have an SOP for technical rescue SCUBA diving. The department relied on mutual-aid departments to perform technical rescue SCUBA diving operations and lacked SOPs for the integration of the mutual-aid responders into the command system. Fire fighters interviewed from different departments reported problems with radio communications and coordination among the four departments on this incident. The victim was not a member of the mutual-aid SCUBA diving teams, and members of the dive team were not initially aware of the victims actions or how they were supposed to integrate the victims actions into their operation.
Recommendation #5: Fire departments should ensure a comprehensive risk-benefit program is in place prior to participating in specialty areas including technical rescue professional level operations.
Discussion: A program that measures the risk vs. benefit of a particular emergency operation is crucial to the safety of all emergency responders. A risk-benefit analysis must be performed on two levels: executive and on the scene. At the executive or strategic level, municipal and fire department leaders should identify their mission capabilities or plan for expanding their current capabilities through long-term funding, training, and continued support. Emergency incident risk-benefit analysis is performed on the scene, by the first arriving responders, and continued throughout the incident by the command structure.
Many communities rely on mutual aid or a combination of jurisdictional resources to provide response capabilities to complex rescue incidents such as high angle, hazardous materials response, trench or confined space, or other technical rescuer professional level operations such as public safety diving. A single community might not possess sufficient resources to effectively and safely provide a response level that would satisfy all the components of a safe, efficient, and effective emergency incident response. Fire department executives should perform a risk-benefit analysis and strategically plan for an emergency response that ensures the safety of all responders. For the more infrequent number of incidents requiring technical rescuer professional level operations such as SCUBA diving teams, preplanning and strategic level risk-benefit analysis can identify the level of response that can be safely performed and alternatives such as mutual aid or multi-jurisdictional, multi-agency capabilities that can be utilized.
In this incident the local fire department provided fire and rescue services to the local community as well as water rescue services through the use of two fire-rescue boats. The department responds to approximately 12 marine/water rescue incidents per year, ranging from boaters and swimmers in distress to ice rescues in the winter months. The department in this incident had mutual aid agreements with other local fire departments and provided this level of marine protection. The fire department did not have a formal SCUBA dive team and relied on mutual aid for this advanced level of technical rescue capability.
Emergency incident risk benefit analysis did occur on this scene and a quick response by the local fire department successfully rescued one civilian from the surface of the lake by fire fighters. Once the emergency incident shifted beyond the capabilities of the local fire department, the mutual aid SCUBA diving team should have performed a risk-benefit analysis by team members who are trained at that level of technical knowledge and the risk evaluation information provided to the incident commander. This level of incident risk-benefit analysis takes into account many factors, such as switching from a rescue to recovery mode, and the dive team plans for the incident accordingly.
Recommendation #6: Fire departments should ensure that programs are in place to provide for training and equipment (including vessels) expected for water rescue and the inspection, maintenance, testing, and replacement of water rescue equipment including SCUBA gear.
Discussion: Organizations that provide water search and rescue operations need to ensure that all members who respond to or may respond to water rescue incidents should be sufficiently trained to the level that they are expected to operate. Surface water search and rescue operations require training on a multi-tiered level. NFPA 1670 Standard on Operations and Training for Technical Search and Rescue Incidents11 describes the levels for water rescue training as awareness, operations, technician, and dive level responsibilities.
In this incident, the fire department provided members with practical training on small boat handling and ice rescue. The members did not receive formal training for surface water rescue incidents which would have provided a safe training foundation for members of the department who frequently provide water rescue services for the local jurisdiction. The department responds to approximately 12 emergency incidents per year involving water rescue and should provide the appropriate level of training for expected areas of emergency response. The fire department responded to the emergency incident with their fire-rescue boat (13-ft utility boat) towed behind a support vehicle. The fire-rescue boat could not be observed in the mirrors of the support vehicle (due to the width of the tow vehicle), and the driver of the support vehicle had to open the rear doors to see the boat and trailer. The boat and trailer were not able to be backed down the boat ramp, and fire fighters had to move the boat and trailer by hand to launch the boat resulting in a delay in getting the boat launched. The fire-rescue boat was not equipped with water rescue gear such as throwable rescue devices and boarding ladders, but was equipped with personal flotation devices for the fire fighters. The fire fighters had to borrow a fender from a civilian boat to improvise a buoy and anchor to mark the location of the civilian victim. If the boat were equipped with a global positioning system (GPS), the fire fighters could have marked the exact location where they picked up the female civilian and would have been able to return to that spot after dropping her off without impact by tide or wind. Minimum recommended equipment necessary for water rescue vessels are dependent on the mission capabilities and the forecasted needs for the locality, such as surface/swift water, surf rescue, ice rescue, and SCUBA diving operations.
Recommendation #7: Fire departments should provide annual and periodic health, wellness, and fitness examinations with specific medical evaluations for fire fighters expected to perform technical rescues such as SCUBA diving.
The purpose of periodic medical evaluations is to ensure that fire fighters have the ability to perform duties without presenting a significant risk to the safety and health of themselves or others. Guidance regarding the content and scheduling of periodic medical examinations for fire fighters can be found in NFPA 1582 Standard on Comprehensive Occupational Medical Program for Fire Departments.13 In addition to providing guidance on the frequency and content of the medical evaluation, NFPA 1582 provides guidance on medical requirements for persons performing fire fighting tasks. Applying NFPA 1582 involves legal and economic issues, so it should be carried out in a confidential, nondiscriminatory manner. Appendix D of NFPA 1582 provides guidance for fire department administrators regarding legal considerations in applying the standard. Technical rescue SCUBA diving candidates should be required to pass a more comprehensive medical evaluation that is administered by a physician familiar with diving medicine. A physician with a strong background in diving medicine and familiar with NFPA 1582 can help provide the technical rescue SCUBA dive team a more comprehensive evaluation of members and candidates.10 The Divers Alert Network14 is one resource technical rescue SCUBA diving teams can use to locate physicians familiar with diving medicine.
Recommendation #8: Fire departments should adopt the International Association of Fire Chiefs Zero-Tolerance Policy for Alcohol and Drinking15 to prohibit the use of alcohol by members of any fire or emergency services agency/organization at any time when they may be called upon to act or respond as a member of those departments. Departments should develop written policies and have procedures in place to enforce this policy.
Discussion: Fire departments should strictly prohibit any member of the fire department from responding to a call if they have been drinking. According to the International Fire Chiefs Association (IAFC) policy statement (#03.04) for Zero-Tolerance for Alcohol & Drinking in the Fire and Emergency Service, if someone has consumed alcohol within the previous eight (8) hours, or is still noticeably impaired by alcohol consumed previous to the eight (8) hours, they must voluntarily remove themselves from the activities and function of the fire or emergency services agency/organization, including all emergency operations and training. In addition, the IAFC policy states, No member of a fire & emergency services agency/organization shall participate in any aspect of the organization and operation of the fire or emergency agency/organization under the influence of alcohol, including but not limited to any fire and emergency operations, fire-police, training, etc.
The following three recommendations are preventive measures recommended by other fire service groups to reduce the risk of on-the-job heart attacks and sudden cardiac arrest among fire fighters. The final recommendation addresses a potential safety issue related to this particular event. These recommendations are listed in order of priority.
Recommendation #9: Fire departments should consider phasing in a mandatory wellness/fitness program for fire fighters to reduce risk factors for cardiovascular disease and improve cardiovascular capacity.
Physical inactivity is the most prevalent modifiable risk factor for coronary artery disease in the United States. Additionally, physical inactivity, or lack of exercise, is associated with other risk factors such as obesity and diabetes.16 NFPA 1500 Standard on Fire Department Occupational Safety and Health Program7 and NFPA 1583 Standard on Health-Related Fitness Programs for Fire Fighters17 recommend a wellness program that provides health promotion activities for preventing health problems and enhancing overall well-being.
In 1997, the International Association of Fire Fighters and the International Association of Fire Chiefs published a comprehensive Fire Service Joint Labor Management Wellness/Fitness Initiative18 to improve fire fighter quality of life and maintain physical and mental capabilities of fire fighters. Ten fire departments across the United States joined this effort to pool information about their physical fitness programs and to create a practical program for the fire service. They produced a manual and video detailing elements of such a program. Fire departments should review these materials to identify applicable elements. Other labor and management negotiated programs, developed for large city departments, can also be reviewed as potential models.
Recommendation #10: Fire departments should consider performing a preplacement and an annual physical performance (physical ability) evaluation for all fire fighters to ensure they are physically capable of performing the essential job tasks of fire fighting.
NFPA 15007 requires fire department members who engage in emergency operations to be annually evaluated and certified by the fire department as meeting the physical performance requirements identified in paragraph 8-2.1.
Recommendation #11: Fire departments should consider ensuring that physicians are knowledgeable about the physical demands of fire fighting and the components of NFPA 1582 and the additional medical and physical requirements of performing technical rescue SCUBA diving.
Frequently, private physicians are not familiar with a fire fighters job duties or with guidance documents such as NFPA 158213. To ensure physicians are aware of these guidelines, we recommend that fire departments provide contract and private physicians with a copy of NFPA 158213 and a SCUBA diving medical clearance form. Lastly, we recommend that all return-to-work clearances be reviewed by a fire department-contracted physician. Thus, the final decision regarding medical clearance for return to work lies with the fire department with input from many sources, including the fire fighters private physician.
REFERENCES
- Joiner JT [2001]. NOAA diving manual. 4th edition. Flagstaff, AZ: Best Publishing Company.
- PADI [1990]. PADI open water diver manual. Santa Ana, CA: Professional Association of Diving Instructors.
- Weather Underground [2009]. Weather history for Rhode Island, August 3, 2008 http://www.wunderground.com/weatherstation/WXDailyHistory.asp?ID=KRITIVER1&month=8&day=3&year=2008
- CDC (Centers for Disease Control and Prevention) [2008]. Adult BMI calculator: English [http://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/english_bmi_calculator/bmi_calculator.html]. Date accessed: September 28, 2009.
- Siegel RJ [1997]. Myocardial hypertrophy. In: Bloom S, ed. Diagnostic criteria for cardiovascular pathology acquired diseases. Philadelphia, PA: Lippencott-Raven, pp. 5557.
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP [1990]. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med 323(24):17061707.
- NFPA [2007]. NFPA 1500 Standard on fire department occupational safety and health program. Quincy, MA: National Fire Protection Association.
- Dodson D [2007]. Fire department incident safety officer. 2nd ed. New York: Delmar Publishers.
- NFPA [2008]. NFPA 1006 Standard for technical rescuer professional qualifications. Quincy, MA: National Fire Protection Association.
- Orusa S [2007]. Dive rescue specialist, operational training for public safety divers. 3rd ed. Fort Collins, CO: Dive Rescue International.
- NFPA [2009]. NFPA 1670 Standard on operations and training for technical search and rescue incidents. Quincy, MA: National Fire Protection Association.
- NFPA [2008]. NFPA 1521 Standard for fire department safety officer. Quincy, MA: National Fire Protection Association.
- NFPA [2007]. NFPA 1582 Standard on comprehensive occupational medical program for fire departments. Quincy, MA: National Fire Protection Association.
- DAN Services, Inc. [2009]. Divers Alert Network: divers helping divers [http://www.diversalertnetwork.org]. Date accessed: September 28, 2009.
- International Association of Fire Chiefs [2004]. Policy statement #03.04: Zero-tolerance for alcohol & drinking in the fire and emergency service [http://www.iafc.org/associations/4685/files/downloads/ABOUT/POLICY_STATES/IAFCpol_Alcohol_inFireEmergServ.pdf]. Date accessed: August 4, 2009.
- Plowman SA, Smith DL [1997]. Exercise physiology: for health, fitness and performance. Boston , MA: Allyn and Bacon.
- NFPA [2000]. NFPA 1583 Standard on health-related fitness programs for fire fighters. Quincy, MA: National Fire Protection Association.
- IAFF, IAFC [2000]. Fire service joint labor management wellness/fitness initiative. Washington, DC: International Association of Fire Fighters, International Association of Fire Chiefs.
INVESTIGATOR INFORMATION
This investigation was conducted by Stephen T. Miles and Jay Tarley, Safety and Occupational Health Specialists with the NIOSH Fire Fighter Fatality Investigation and Prevention Program (FFFIPP) traumatic injury component, located in Morgantown, WV, and Tommy Baldwin, Safety and Occupational Health Specialist with the FFFIPP Cardiovascular Disease Component, located in Cincinnati, Ohio. An expert technical review was conducted by Captain Steven Orusa of the City of Waukegan Fire Department, and Assistant Fire Chief, Beach Park Fire Department, Beach Park, Illinois. Chief Orusa is also the author of Dive Rescue Specialist, Operational Training for Public Safety Divers. An equipment evaluation was performed by Craig Jenni with Dive & Marine Consultants International, Inc., Boca Raton, FL. This report was authored by Stephen T. Miles.
APPENDIX
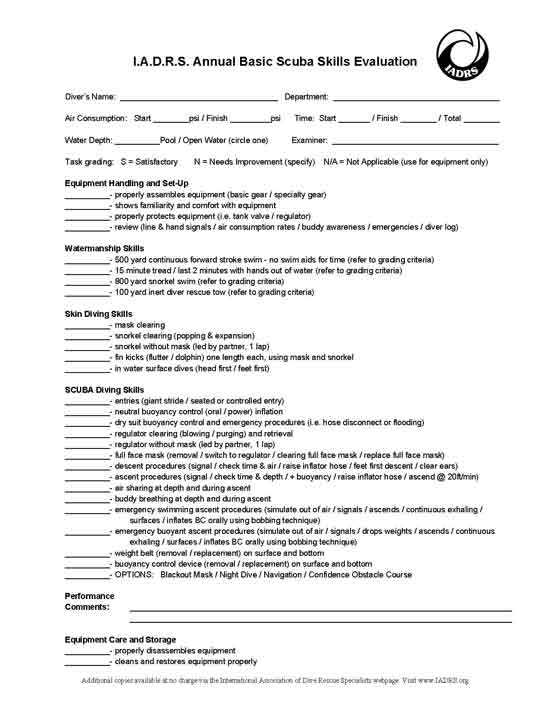
|
Appendix. Annual Basic SCUBA Skills Evaluation. |
PHOTOS AND DIAGRAMS



|
The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In fiscal year 1998, the Congress appropriated funds to NIOSH to conduct a fire fighter initiative. NIOSH initiated the Fire Fighter Fatality Investigation and Prevention Program to examine deaths of fire fighters in the line of duty so that fire departments, fire fighters, fire service organizations, safety experts and researchers could learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent future fire fighter deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under its program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agencys recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit
the program website at www.cdc.gov/niosh/fire or call toll free 1-800-CDC-INFO (1-800-232-4636).
|
This page was last updated on 10/07/09.
- Page last reviewed: November 18, 2015
- Page last updated: October 15, 2014
- Content source:
- National Institute for Occupational Safety and Health Division of Safety Research