Bronchiectasis
| Bronchiectasis | |
|---|---|
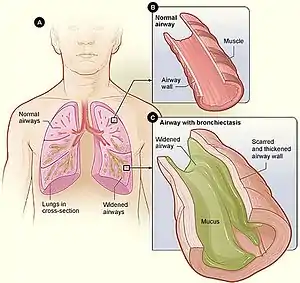 | |
| Figure A shows a cross-section of the lungs with normal airways and widened airways. Figure B shows a cross-section of a normal airway. Figure C shows a cross-section of an airway with bronchiectasis. | |
| Pronunciation |
|
| Specialty | Pulmonology |
| Symptoms | Productive cough, shortness of breath, chest pain[2][3] |
| Usual onset | Gradual[4] |
| Duration | Long term[5] |
| Causes | Infections, cystic fibrosis, other genetic conditions, unknown[3][6] |
| Diagnostic method | Based on symptoms, CT scan[7] |
| Treatment | Antibiotics, bronchodilators, lung transplant[3][8][9] |
| Frequency | 1–250 per 250,000 adults[10] |
Bronchiectasis is a disease in which there is permanent enlargement of parts of the airways of the lung.[5] Symptoms typically include a chronic cough with mucus production.[3] Other symptoms include shortness of breath, coughing up blood, and chest pain.[2] Wheezing and nail clubbing may also occur.[2] Those with the disease often get frequent lung infections.[8]
Bronchiectasis may result from a number of infectious and acquired causes, including pneumonia, tuberculosis, immune system problems, as well as the genetic disorder cystic fibrosis.[11][3][12] Cystic fibrosis eventually results in severe bronchiectasis in nearly all cases.[13] The cause in 10–50% of those without cystic fibrosis is unknown.[3] The mechanism of disease is breakdown of the airways due to an excessive inflammatory response.[3] Involved airways (bronchi) become enlarged and thus less able to clear secretions.[3] These secretions increase the amount of bacteria in the lungs, resulting in airway blockage and further breakdown of the airways.[3] It is classified as an obstructive lung disease, along with chronic obstructive pulmonary disease and asthma.[14] The diagnosis is suspected based on symptoms and confirmed using computed tomography.[7] Cultures of the mucus produced may be useful to determine treatment in those who have acute worsening and at least once a year.[7]
Periods of worsening may occur due to infection.[8] In these cases, antibiotics are recommended.[8] Common antibiotics used include amoxicillin, erythromycin, or doxycycline.[15] Antibiotics, such as erythromycin, may also be used to prevent worsening of disease.[3][16] Airway clearance techniques, a type of physical therapy, are also recommended.[17] Medications to dilate the airways and inhaled steroids may be used during sudden worsening, but there are no studies to determine effectiveness.[3][18] There are also no studies on the use of inhaled steroids in children.[18] Surgery, while commonly done, has not been well studied.[19][3] Lung transplantation may be an option in those with very severe disease.[9]
Bronchiectasis affects between 1 per 1000 and 1 per 250,000 adults.[10] The disease is more common in women and increases as people age.[3] It became less common since the 1950s with the introduction of antibiotics.[10] It is more common among certain ethnic groups such as indigenous people.[10] It was first described by Rene Laennec in 1819.[3] The economic costs in the United States are estimated at $630 million per year.[3]
Signs and symptoms

Symptom of bronchiectasis commonly include a cough productive of frequent green or yellow sputum lasting months to years.[3] Other common symptoms include difficulty breathing, wheezing (a whistling sound when you breath), and chest pain. Bronchiectasis may also present with coughing up blood in the absence of sputum, which has been called "dry bronchiectasis."
People often report frequent bouts of "bronchitis" requiring therapy with repeated courses of antibiotics. People with bronchiectasis may have bad breath from active infection. On examination, crepitations and expiratory rhonchi may be heard with auscultation. Nail clubbing is a rare symptom.[3]
The complications of bronchiectasis include serious health conditions, such as respiratory failure and atelectasis. Respiratory failure occurs when not enough oxygen passes from the lungs into the blood.[20] Atelectasis occur when one or more segments of the lungs collapse or do not inflate properly. Other pulmonary complications include lung abscess and empyema. Cardiovascular complications include cor pulmonale, in which there is enlargement and failure of the right side of the heart as a result of disease of the lungs.[21]
Causes
| Category | Causes |
|---|---|
| Autoimmune disease | Rheumatoid arthritis |
| Impaired host defenses | Cystic fibrosis |
| Post-infective | Bacterial pneumonia
Mycobacterium infection Viral infection |
| Congenital | Tracheobronchomegaly |
| Hypersensitivity | Allergic bronchopulmonary aspergillosis |
| Inflammatory bowel disease | Ulcerative colitis |
| Malignancy | Chronic lymphocytic leukemia |
| Obstruction | Tumor |
| Other | Pneumonia
Chronic aspiration Ammonia inhalation Radiation-induced lung disease |
There are many causes that can induce or contribute to the development of bronchiectasis. The frequency of these different causes varies with geographic location.[22] Cystic fibrosis is identified as a cause in up to half of cases.[3] Bronchiectasis without CF is known as non-CF bronchiectasis. Historically, about half of all case of non-CF bronchiectasis were found to be idiopathic, or without a known cause.[23] However, more recent studies with a more thorough diagnostic work-up have found an etiology in 60 to 90% of patients.[22][24][25]
Cystic fibrosis
Cystic fibrosis is the most common life-threatening autosomal recessive disease in the United States and Europe.[26] It is a genetic disorder that affects the lungs, but also the pancreas, liver, kidneys, and intestine.[27] It is caused by mutations in the CFTR protein, a chloride channel expressed in epithelial cells.[26] Lung disease results from clogging of the airways due to mucus build-up, decreased mucociliary clearance, and resulting inflammation.[28] In later stages, changes to the structure of the lung, such as bronchiectasis, occur. Around 5 to 10% of all patients with cystic fibrosis develop bronchiectasis.[29]
Airway obstruction
An airway obstruction can be caused by either an intraluminal mass such as a tumor or a foreign body.[30] The presence of an airway obstruction leads to a cycle of inflammation.[3] It is important to identify the presence of an obstruction because surgical resection is often curative if obstruction is the cause.[31] In adults, foreign body aspiration is often associated with an altered state of consciousness. The foreign body is often unchewed food, or part of a tooth or crown.[32] Bronchiectasis that results from foreign body aspiration generally occurs in the right lung in the lower lobe or posterior segments of the upper lobe.[33]
Lung infections
A range of bacterial, mycobacterial, and viral lung infections are associated with the development of bronchiectasis. Bacterial infections commonly associated with bronchiectasis include P. aeruginosa, H. influenzae, and S. pneumoniae.[3] Gram-negative bacteria are more commonly implicated than gram-positive bacteria.[3] A history of mycobacterial infections such as tuberculosis can lead to damage of the airways that predisposes to bacterial colonization.[34] Severe viral infections in childhood can also lead to bronchiectasis through a similar mechanism.[35] Nontuberculous mycobacteria infections such as Mycobacterium avium complex are found to be a cause in some patients.[36] Recent studies have also shown Nocardia infections to been implicated in bronchiectasis.[37]
Impaired host defenses
Impairments in host defenses that lead to bronchiectasis may be congenital, such as with primary ciliary dyskinesia, or acquired, such as with the prolonged use of immunosuppressive drugs.[38] Additionally, these impairments may be localized to the lungs, or systemic throughout the body. In these states of immunodeficiency, there is a weakened or absent immune system response to severe infections that repeatedly affect the lung and eventually result in bronchial wall injury.[39] HIV/AIDS is an example of an acquired immunodeficiency that can lead to the development of bronchiectasis.[40]
Aspergillosis
Allergic bronchopulmonary aspergillosis (ABPA) is an inflammatory disease caused by hypersensitivity to the fungus Aspergillus fumigatus.[41] It is suspected in patients with a long history of asthma and symptoms of bronchiectasis such as a productive, mucopurulent cough.[42] Imaging often shows peripheral and central airway bronchiectasis, which is unusual in patients with bronchiectasis caused by other disorders.[43]
Autoimmune diseases
Several autoimmune diseases have been associated with bronchiectasis. Specifically, individuals with rheumatoid arthritis and Sjögren syndrome have increased rates of bronchiectasis.[44][45] In these diseases, the symptoms of bronchiectasis usually presents later in the disease course.[46] Other autoimmune diseases such as ulcerative colitis and Crohn's disease also have an association with bronchiectasis.[47] Additionally, graft-versus-host disease in patients who have underwent stem cell transplantation can lead to bronchiectasis as well.[38]
Lung injury
Bronchiectasis could be caused by: inhalation of ammonia and other toxic gases,[48] chronic pulmonary aspiration of stomach acid from esophageal reflux,[49] or a hiatal hernia.[49]
Congenital
Bronchiectasis may result from congenital disorders that affect cilia motility or ion transport.[50] A common genetic cause is cystic fibrosis, which affects chloride ion transport.[26] Another genetic cause is primary ciliary dyskinesia, a rare disorder that leads to immotility of cilia and can lead to situs inversus.[51] When situs inversus is accompanied by chronic sinusitis and bronchiectasis, this is known as Kartagener's syndrome.[52] Other rare genetic causes include Young's syndrome[53] and Williams-Campbell syndrome.[54] Tracheobronchomegaly, or Mournier-Kuhn syndrome is a rare condition characterized by significant tracheobronchial dilation and recurrent lower respiratory tract infections.[55] Individuals with alpha 1-antitrypsin deficiency have been found to be particularly susceptible to bronchiectasis, due to the loss of inhibition to enzyme elastase which cleaves elastin.[56] This decreases the ability of the alveoli to return to normal shape during expiration.[57]
Cigarette smoking
A causal role for tobacco smoke in bronchiectasis has not been demonstrated.[38] Nonetheless, tobacco smoking can worsen pulmonary function and accelerate the progression of disease that is already present.[58][59]
Pathophysiology

The development of bronchiectasis requires two factors: an infectious insult and impaired drainage, obstruction, or a defect in host defense.[3] This triggers a host immune response from neutrophils (elastases), reactive oxygen species, and inflammatory cytokines that results in progressive destruction of normal lung architecture. In particular, the elastic fibers of bronchi are affected.[12] The result is permanent abnormal dilation and destruction of the major bronchi and bronchiole walls.
The "vicious cycle" theory is the generally accepted explanation for the pathogenesis of bronchiectasis.[60] In this model, a predisposed individual develops an excessive inflammatory response to pulmonary infection or tissue injury. The inflammation that results is partially responsible for the structural damage to the airways. The structural abnormalities allow for the stasis of mucus, which favors continued chronic infection and the persistence of the vicious cycle.[3]
Endobronchial tuberculosis commonly leads to bronchiectasis, either from bronchial stenosis or secondary traction from fibrosis.[61] Traction bronchiectasis characteristically affects peripheral bronchi (which lack cartilage support) in areas of end-stage fibrosis.[62]
Diagnosis

The goals of a diagnostic evaluation for bronchiectasis are radiographic confirmation of the diagnosis, identification of potential treatable causes, and functional assessment of the patient. A comprehensive evaluation consists of radiographic imaging, laboratory testing, and lung function testing.[63]
A chest x-ray is abnormal in most patients with bronchiectasis. Computed tomography is recommended to confirm the diagnosis and is also used to describe the distribution and grade the severity of the disease. Radiographic findings include airway dilation, bronchial wall thickening, and atelectasis.[3]
Laboratory tests that are commonly part of the initial evaluation include a complete blood count, sputum cultures for bacteria, mycobacteria, and fungi, testing for cystic fibrosis, and immunoglobulin levels.[64] Additional tests that are sometimes indicated include testing for specific genetic disorders.
Lung function testing is used for the assessment and monitoring of functional impairment due to bronchiectasis. These tests may include spirometry and walking tests.[60] Obstructive lung impairment is the most common finding but restrictive lung impairment can be seen in advanced disease. Flexible bronchoscopy may be performed when sputum studies are negative and a focal obstructing lesion is suspected.[30]
.jpg.webp) Bronchiectasis primarily in the middle lobe of the right lung.
Bronchiectasis primarily in the middle lobe of the right lung. Bronchiectasis secondary to a large carcinoid tumor (not shown) that was completely obstructing the bronchus proximally. Dilation of the airways is present.
Bronchiectasis secondary to a large carcinoid tumor (not shown) that was completely obstructing the bronchus proximally. Dilation of the airways is present.
Prevention
In preventing bronchiectasis, it is necessary to prevent the lung infections and lung damage that can cause it.[20] Children should be immunized against measles, pertussis, pneumonia, and other acute respiratory infections of childhood. Additionally, parents should stay alert to keep children from inhaling objects such as pieces of food or small toys that may get stuck in small airways.[20] Smoking and other toxic fumes and gases should be avoided by all patients with bronchiectasis to decrease the development of infections (such as bronchitis) and further complications.[65]
Treatments to slow down the progression of this chronic disease include keeping bronchial airways clear and secretions weakened through various forms of airway clearance. Aggressively treating bronchial infections with antibiotics to prevent the destructive cycle of infection, damage to bronchi and bronchioles, and more infection is also standard treatment. Regular vaccination against pneumonia, influenza, and pertussis are generally advised. A healthy body mass index and regular doctor visits may have beneficial effects on the prevention of progressing bronchiectasis. The presence of hypoxemia, hypercapnia, dyspnea level and radiographic extent can greatly affect the mortality rate from this disease.[66]
Management
A comprehensive approach to the management of bronchiectasis is recommended.[67] It is important to establish whether an underlying modifiable cause, such as immunoglobulin deficiency or alpha-1 antitrypsin deficiency is present.[67] The next steps include controlling infections and bronchial secretions, relieving airway obstructions, removing affected portions of lung by surgery, and preventing complications.[68]
Airway clearance
The goal of airway clearance therapy is to loosen secretions and interrupt the cycle of inflammation and infection.[69] Airway clearance techniques improve difficulty breathing, cough, and help patients cough up phlegm and mucus plugs.[70] Airway clearance usually uses an inhaled agent (hypertonic saline) with chest physiotherapy, such as high-frequency chest wall oscillation.[3] Many airway clearance techniques and devices exist. The choice of a technique or device is based on the frequency and tenacity of phlegm, patient comfort, cost, and the patient's ability to use the technique or device with minimal interference to their lifestyle.[71] Mucolytic agents such as dornase alfa are not recommended for individuals with non-CF bronchiectasis.[3] Mannitol is a hyperosmolar agent that is thought to hydrate airway secretions, however, clinical trials with it have not demonstrated efficacy.[71]
Anti-inflammatories
The two most commonly used classes of anti-inflammatory therapies are macrolides and corticosteroids.[3]
Despite also being antibiotics, macrolides exert immunomodulatory effects on the host inflammatory response without systemic suppression of the immune system.[3] These effects include modifying mucus production, inhibition of biofilm production, and suppression of inflammatory mediators.[38] Three large multicenter, randomized trials have shown reduced rates of exacerbations and improved cough and dyspnea with use of macrolide therapy.[72] The impact of adverse effects of macrolides such as gastrointestinal symptoms, hepatotoxicity, and increased antimicrobial resistance needs ongoing review and study.[16]
Inhaled corticosteroid therapy can reduce sputum production and decrease airway constriction over a period of time, helping prevent progression of bronchiectasis.[73] Long term use of high-dose inhaled corticosteroids can lead to adverse consequences such as cataracts and osteoporosis.[3] It is not recommended for routine use in children.[74] One commonly used therapy is beclometasone dipropionate.[75]
Antibiotics
_tablets.jpg.webp)
Antibiotics are used to eradicate P. aeruginosa or MRSA, to suppress the burden of chronic bacterial colonization, and to treat exacerbations.[3] The use of daily oral non-macrolide antibiotic treatment has been studied in small case series, but not in randomized trials.[72] The role of inhaled antibiotics in non-CF bronchiectasis has recently evolved with two society guidelines and a systematic review suggesting a therapeutic trial of inhaled antibiotics in patients with three or more exacerbations per year and P. aeruginosa in their sputum.[76][77] Options for inhaled antibiotics include aerosolized tobramycin, inhaled ciprofloxacin, aerosolized aztreonam, and aerosolized colistin.[38]
Bronchodilators
Some clinical trials have shown a benefit with inhaled bronchodilators in certain people with bronchiectasis.[3] In people with demonstrated bronchodilator reversibility on spirometry, the use of inhaled bronchodilators resulted in improved dyspnea, cough, and quality of life without any increase in adverse events.[63] However, overall there is a lack of data to recommend use of bronchodilators in all patients with bronchiectasis.[78]
Surgery
The primary role of surgery in the management of bronchiectasis is in localized disease to remove segments of the lung or to control massive hemoptysis.[38] Additionally, surgery is used to remove an airway obstruction that is contributing to bronchiectasis. The goals are conservative, aiming to control specific disease manifestations rather than cure or eliminate all areas of bronchiectasis.[79] Surgical case series have shown low operative mortality rate (less than 2%) and improvement of symptoms in the majority of patients selected to receive surgery.[80] However, no randomized clinical trials have been performed evaluating the efficacy of surgery in bronchiectasis.[79]
Epidemiology
The disease affects between 1 per 1000 and 1 per 250,000 adults.[10] The disease is more common in women and increases as people age.[3] It became less common since the 1950s, with the introduction of antibiotics.[10] It is more common among certain ethnic groups such as indigenous people.[10]
An estimated 350,000 to 500,000 adults have bronchiectasis in the United States.[81] The disease is more common in women and in elderly individuals over the age of 65.[3] Specifically, children of the indigenous populations of Australia, Alaska, Canada and New Zealand have significantly higher rates than other populations.[82] Overall, a shortage of data exists concerning the epidemiology of bronchiectasis in Asia, Africa, and South America.[82]
The exact rates of bronchiectasis are often unclear as the symptoms are variable.[83] Rates of disease appeared to have increased in the United States between 2000 and 2007.[3]
History
René Laennec, the man who invented the stethoscope, used his invention to first discover bronchiectasis in 1819.[84]
The disease was researched in greater detail by Sir William Osler, one of the four founding professors of Johns Hopkins Hospital, in the late 1800s. It is suspected that Osler himself died of complications from undiagnosed bronchiectasis. His biographies mention that he suffered frequent severe chest infections for many years.[85]
The term "bronchiectasis" comes from the Greek words bronkhia (meaning "airway") and ektasis (meaning "widening").[86]
References
- ↑ "Bronchiectasis | Definition of Bronchiectasis by Lexico". Lexico Dictionaries | English. Archived from the original on 2019-11-09. Retrieved 2019-11-09.
- 1 2 3 "What Are the Signs and Symptoms of Bronchiectasis?". NHLBI. June 2, 2014. Archived from the original on 23 August 2016. Retrieved 10 August 2016.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 McShane, PJ; Naureckas, ET; Tino, G; Strek, ME (Sep 15, 2013). "Non-cystic fibrosis bronchiectasis". American Journal of Respiratory and Critical Care Medicine. 188 (6): 647–56. doi:10.1164/rccm.201303-0411CI. PMID 23898922.
- ↑ Maguire, G (November 2012). "Bronchiectasis – a guide for primary care". Australian Family Physician. 41 (11): 842–50. PMID 23145413.
- 1 2 "What Is Bronchiectasis?". NHLBI. June 2, 2014. Archived from the original on 10 August 2016. Retrieved 10 August 2016.
- ↑ Bird, K; Memon, J (January 2019). "Bronchiectasis". PMID 28613561.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 3 "Quality Standards for Clinically Significant Bronchiectasis in Adults". British Thoracic Society. July 2012. Archived from the original on 7 July 2017. Retrieved 29 April 2017.
- 1 2 3 4 "How Is Bronchiectasis Treated?". NHLBI. June 2, 2014. Archived from the original on 28 July 2016. Retrieved 10 August 2016.
- 1 2 Corris, PA (Jun 2013). "Lung transplantation for cystic fibrosis and bronchiectasis". Seminars in Respiratory and Critical Care Medicine. 34 (3): 297–304. doi:10.1055/s-0033-1348469. PMID 23821505.
- 1 2 3 4 5 6 7 Cottin, Vincent; Cordier, Jean-Francois; Richeldi, Luca (2015). Orphan Lung Diseases: A Clinical Guide to Rare Lung Disease. Springer. p. 30. ISBN 9781447124016. Archived from the original on 2016-08-21.
- ↑ José, R. J.; Brown, J. S. (2014). "Bronchiectasis". British Journal of Hospital Medicine. 75 (Suppl 10:C146–51): C146–C151. doi:10.12968/hmed.2014.75.Sup10.C146. PMID 25289486.
- 1 2 Nicki R. Colledge; Brian R. Walker; Stuart H. Ralston, eds. (2010). Davidson's principles and practice of medicine. illustrated by Robert Britton (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- ↑ Brant, William E.; Helms, Clyde A., eds. (2006). Fundamentals of diagnostic radiology (3rd ed.). Philadelphia: Lippincott Williams & Wilkins. p. 518. ISBN 9780781761352. Archived from the original on 2017-09-06.
- ↑ Michael Filbin; Lisa M. Lee; Shaffer, Brian L. (2003). Blueprints pathophysiology II : pulmonary, gastrointestinal, and rheumatology : notes & cases (1st ed.). Malden, Mass.: Blackwell Pub. p. 12. ISBN 9781405103510. Archived from the original on 2017-09-06.
- ↑ Brent, Andrew; Davidson, Robert; Seale, Anna (2014). Oxford Handbook of Tropical Medicine. OUP Oxford. p. 223. ISBN 9780191503078. Archived from the original on 2016-08-21.
- 1 2 Wu, Qibiao; Shen, Weixing; Cheng, Haibo; Zhou, Xiqiao (April 2014). "Long-term macrolides for non-cystic fibrosis bronchiectasis: a systematic review and meta-analysis". Respirology (Carlton, Vic.). 19 (3): 321–329. doi:10.1111/resp.12233. ISSN 1440-1843. PMID 24417869.
- ↑ Lee, AL; Burge, AT; Holland, AE (23 November 2015). "Airway clearance techniques for bronchiectasis". The Cochrane Database of Systematic Reviews (11): CD008351. doi:10.1002/14651858.CD008351.pub3. PMC 7175838. PMID 26591003.
- 1 2 Kapur, Nitin; Petsky, Helen L.; Bell, Scott; Kolbe, John; Chang, Anne B. (16 May 2018). "Inhaled corticosteroids for bronchiectasis". The Cochrane Database of Systematic Reviews. 5: CD000996. doi:10.1002/14651858.CD000996.pub3. ISSN 1469-493X. PMC 6494510. PMID 29766487.
- ↑ Corless, JA; Warburton, CJ (2000). "Surgery vs non-surgical treatment for bronchiectasis". The Cochrane Database of Systematic Reviews (4): CD002180. doi:10.1002/14651858.CD002180. PMID 11034745. S2CID 72965871.
- 1 2 3 "Bronchiectasis | National Heart, Lung, and Blood Institute (NHLBI)". www.nhlbi.nih.gov. Archived from the original on 2019-12-21. Retrieved 2019-11-20.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - ↑ "Bronchiectasis: Practice Essentials, Background, Pathophysiology". 2019-11-11. Archived from the original on 2020-04-03. Retrieved 2019-11-21.
{{cite journal}}: Cite journal requires|journal=(help) - 1 2 McShane, Pamela J.; Naureckas, Edward T.; Strek, Mary E. (July 2012). "Bronchiectasis in a diverse US population: effects of ethnicity on etiology and sputum culture". Chest. 142 (1): 159–167. doi:10.1378/chest.11-1024. ISSN 1931-3543. PMID 22267679.
- ↑ Gao, Yong-Hua; Guan, Wei-Jie; Liu, Shao-Xia; Wang, Lei; Cui, Juan-Juan; Chen, Rong-Chang; Zhang, Guo-Jun (November 2016). "Aetiology of bronchiectasis in adults: A systematic literature review". Respirology (Carlton, Vic.). 21 (8): 1376–1383. doi:10.1111/resp.12832. ISSN 1440-1843. PMID 27321896.
- ↑ Lonni, Sara; Chalmers, James D.; Goeminne, Pieter C.; McDonnell, Melissa J.; Dimakou, Katerina; De Soyza, Anthony; Polverino, Eva; Van de Kerkhove, Charlotte; Rutherford, Robert; Davison, John; Rosales, Edmundo (December 2015). "Etiology of Non-Cystic Fibrosis Bronchiectasis in Adults and Its Correlation to Disease Severity". Annals of the American Thoracic Society. 12 (12): 1764–1770. doi:10.1513/AnnalsATS.201507-472OC. ISSN 2325-6621. PMC 5467084. PMID 26431397.
- ↑ Brower, Kelly S.; Del Vecchio, Michael T.; Aronoff, Stephen C. (2014-12-10). "The etiologies of non-CF bronchiectasis in childhood: a systematic review of 989 subjects". BMC Pediatrics. 14: 4. doi:10.1186/s12887-014-0299-y. ISSN 1471-2431. PMC 4275950. PMID 25492164.
- 1 2 3 Rowe, Steven M.; Miller, Stacey; Sorscher, Eric J. (2005-05-12). "Cystic Fibrosis". New England Journal of Medicine. 352 (19): 1992–2001. doi:10.1056/NEJMra043184. ISSN 0028-4793. PMID 15888700.
- ↑ O'Sullivan, Brian P.; Freedman, Steven D. (2009-05-30). "Cystic fibrosis". Lancet. 373 (9678): 1891–1904. doi:10.1016/S0140-6736(09)60327-5. ISSN 1474-547X. PMID 19403164.
- ↑ Elborn, J. Stuart (19 November 2016). "Cystic fibrosis". Lancet. 388 (10059): 2519–2531. doi:10.1016/S0140-6736(16)00576-6. ISSN 1474-547X. PMID 27140670.
- ↑ Contarini, Martina; Finch, Simon; Chalmers, James D. (2018-09-30). "Bronchiectasis: a case-based approach to investigation and management". European Respiratory Review. 27 (149): 180016. doi:10.1183/16000617.0016-2018. ISSN 1600-0617. PMID 29997246.
- 1 2 Kwon, K. Y.; Myers, J. L.; Swensen, S. J.; Colby, T. V. (March 1995). "Middle lobe syndrome: a clinicopathological study of 21 patients". Human Pathology. 26 (3): 302–307. doi:10.1016/0046-8177(95)90062-4. ISSN 0046-8177. PMID 7890282.
- ↑ Priftis, Kostas N.; Mermiri, Despina; Papadopoulou, Athina; Anthracopoulos, Michael B.; Vaos, George; Nicolaidou, Polyxeni (October 2005). "The role of timely intervention in middle lobe syndrome in children". Chest. 128 (4): 2504–2510. doi:10.1378/chest.128.4.2504. ISSN 0012-3692. PMID 16236916. S2CID 5902678.
- ↑ Rafanan, A. L.; Mehta, A. C. (June 2001). "Adult airway foreign body removal. What's new?". Clinics in Chest Medicine. 22 (2): 319–330. doi:10.1016/s0272-5231(05)70046-0. ISSN 0272-5231. PMID 11444115.
- ↑ "Aspiration Pneumonitis and Pneumonia: Overview of Aspiration Pneumonia, Predisposing Conditions for Aspiration Pneumonia, Pathophysiology of Aspiration Pneumonia". 2019-10-19. Archived from the original on 2019-12-09. Retrieved 2019-11-08.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Kwak, Hyun Jung; Moon, Ji-Yong; Choi, Yo Won; Kim, Tae Hyung; Sohn, Jang Won; Yoon, Ho Joo; Shin, Dong Ho; Park, Sung Soo; Kim, Sang-Heon (December 2010). "High prevalence of bronchiectasis in adults: analysis of CT findings in a health screening program". The Tohoku Journal of Experimental Medicine. 222 (4): 237–242. doi:10.1620/tjem.222.237. ISSN 1349-3329. PMID 21127394.
- ↑ Kim, C. K.; Chung, C. Y.; Kim, J. S.; Kim, W. S.; Park, Y.; Koh, Y. Y. (February 2000). "Late abnormal findings on high-resolution computed tomography after Mycoplasma pneumonia". Pediatrics. 105 (2): 372–378. doi:10.1542/peds.105.2.372. ISSN 1098-4275. PMID 10654958. S2CID 25928060.
- ↑ Dimakou, Katerina; Triantafillidou, Christina; Toumbis, Michail; Tsikritsaki, Kyriaki; Malagari, Katerina; Bakakos, Petros (July 2016). "Non CF-bronchiectasis: Aetiologic approach, clinical, radiological, microbiological and functional profile in 277 patients". Respiratory Medicine. 116: 1–7. doi:10.1016/j.rmed.2016.05.001. ISSN 1532-3064. PMID 27296814.
- ↑ Woodworth, Michael H.; Saullo, Jennifer L.; Lantos, Paul M.; Cox, Gary M.; Stout, Jason E. (March 2017). "Increasing Nocardia Incidence Associated with Bronchiectasis at a Tertiary Care Center". Annals of the American Thoracic Society. 14 (3): 347–354. doi:10.1513/AnnalsATS.201611-907OC. ISSN 2325-6621. PMID 28231023.
- 1 2 3 4 5 6 Chalmers, James D.; Chang, Anne B.; Chotirmall, Sanjay H.; Dhar, Raja; McShane, Pamela J. (15 November 2018). "Bronchiectasis". Nature Reviews. Disease Primers. 4 (1): 45. doi:10.1038/s41572-018-0042-3. ISSN 2056-676X. PMID 30442957.
- ↑ Rook, Mieneke; Postma, Dirkje S.; van der Jagt, Eric J.; van Minnen, Cees A.; van der Heide, Jaap J. Homan; Ploeg, Rutger J.; van Son, Willem J. (2006-01-27). "Mycophenolate mofetil and bronchiectasis in kidney transplant patients: a possible relationship". Transplantation. 81 (2): 287–289. doi:10.1097/01.tp.0000188638.28003.96. ISSN 0041-1337. PMID 16436974.
- ↑ Attia, Engi F.; Miller, Robert F.; Ferrand, Rashida A. (February 2017). "Bronchiectasis and other chronic lung diseases in adolescents living with HIV". Current Opinion in Infectious Diseases. 30 (1): 21–30. doi:10.1097/QCO.0000000000000325. ISSN 1473-6527. PMC 5408733. PMID 27753690.
- ↑ Greenberger, Paul A.; Bush, Robert K.; Demain, Jeffrey G.; Luong, Amber; Slavin, Raymond G.; Knutsen, Alan P. (November 2014). "Allergic bronchopulmonary aspergillosis". The Journal of Allergy and Clinical Immunology. In Practice. 2 (6): 703–708. doi:10.1016/j.jaip.2014.08.007. ISSN 2213-2201. PMC 4306287. PMID 25439360.
- ↑ De Soyza, Anthony; Aliberti, Stefano (2017-01-01). "Bronchiectasis and Aspergillus: How are they linked?". Medical Mycology. 55 (1): 69–81. doi:10.1093/mmy/myw109. ISSN 1460-2709. PMID 27794529.
- ↑ Agarwal, R.; Chakrabarti, A.; Shah, A.; Gupta, D.; Meis, J. F.; Guleria, R.; Moss, R.; Denning, D. W.; ABPA complicating asthma ISHAM working group (August 2013). "Allergic bronchopulmonary aspergillosis: review of literature and proposal of new diagnostic and classification criteria". Clinical and Experimental Allergy. 43 (8): 850–873. doi:10.1111/cea.12141. ISSN 1365-2222. PMID 23889240. S2CID 24077597.
- ↑ Wilczynska, Maria M.; Condliffe, Alison M.; McKeon, Damian J. (April 2013). "Coexistence of bronchiectasis and rheumatoid arthritis: revisited". Respiratory Care. 58 (4): 694–701. doi:10.4187/respcare.01857. ISSN 1943-3654. PMID 22782500.
- ↑ Soto-Cardenas, M.-J.; Perez-De-Lis, M.; Bove, A.; Navarro, C.; Brito-Zeron, P.; Diaz-Lagares, C.; Gandia, M.; Akasbi, M.; Siso, A.; Ballester, E.; Torres, A. (September 2010). "Bronchiectasis in primary Sjögren's syndrome: prevalence and clinical significance". Clinical and Experimental Rheumatology. 28 (5): 647–653. ISSN 0392-856X. PMID 20883638.
- ↑ Chatzidionisyou, Aikaterini; Catrina, Anca I. (January 2016). "The lung in rheumatoid arthritis, cause or consequence?". Current Opinion in Rheumatology. 28 (1): 76–82. doi:10.1097/BOR.0000000000000238. ISSN 1531-6963. PMID 26599384.
- ↑ Black, Hugh; Mendoza, Mark; Murin, Susan (February 2007). "Thoracic manifestations of inflammatory bowel disease". Chest. 131 (2): 524–532. doi:10.1378/chest.06-1074. ISSN 0012-3692. PMID 17296657.
- ↑ Magis-Escurra, Cecile; Reijers, Monique He (2015-02-25). "Bronchiectasis". BMJ Clinical Evidence. 2015. ISSN 1752-8526. PMC 4356176. PMID 25715965.
- 1 2 Li, A. M.; Sonnappa, S.; Lex, C.; Wong, E.; Zacharasiewicz, A.; Bush, A.; Jaffe, A. (July 2005). "Non-CF bronchiectasis: does knowing the aetiology lead to changes in management?". The European Respiratory Journal. 26 (1): 8–14. doi:10.1183/09031936.05.00127704. ISSN 0903-1936. PMID 15994383.
- ↑ Nicki R. Colledge; Brian R. Walker; Stuart H. Ralston, eds. (2010). Davidson's principles and practice of medicine. illustrated by Robert Britton (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- ↑ Goutaki, Myrofora; Meier, Anna Bettina; Halbeisen, Florian S.; Lucas, Jane S.; Dell, Sharon D.; Maurer, Elisabeth; Casaulta, Carmen; Jurca, Maja; Spycher, Ben D.; Kuehni, Claudia E. (October 2016). "Clinical manifestations in primary ciliary dyskinesia: systematic review and meta-analysis". The European Respiratory Journal. 48 (4): 1081–1095. doi:10.1183/13993003.00736-2016. ISSN 1399-3003. PMID 27492829.
- ↑ Mishra, Mayank; Kumar, Naresh; Jaiswal, Ashish; Verma, Ajay K.; Kant, Surya (October 2012). "Kartagener's syndrome: A case series". Lung India. 29 (4): 366–369. doi:10.4103/0970-2113.102831. ISSN 0970-2113. PMC 3519024. PMID 23243352.
- ↑ Hendry, W. F.; A'Hern, R. P.; Cole, P. J. (18–25 December 1993). "Was Young's syndrome caused by exposure to mercury in childhood?". BMJ (Clinical Research Ed.). 307 (6919): 1579–1582. doi:10.1136/bmj.307.6919.1579. ISSN 0959-8138. PMC 1697782. PMID 8292944.
{{cite journal}}: CS1 maint: date format (link) - ↑ WILLIAMS H, CAMPBELL P (April 1960). "Generalized Bronchiectasis associated with Deficiency of Cartilage in the Bronchial Tree". Arch. Dis. Child. 35 (180): 182–91. doi:10.1136/adc.35.180.182. PMC 2012546. PMID 13844857.
- ↑ Celik, Burcin; Bilgin, Salih; Yuksel, Canan (2011). "Mounier-Kuhn syndrome: a rare cause of bronchial dilation". Texas Heart Institute Journal. 38 (2): 194–196. ISSN 1526-6702. PMC 3066798. PMID 21494536.
- ↑ Parr, David G.; Guest, Peter G.; Reynolds, John H.; Dowson, Lee J.; Stockley, Robert A. (2007-12-15). "Prevalence and impact of bronchiectasis in alpha1-antitrypsin deficiency". American Journal of Respiratory and Critical Care Medicine. 176 (12): 1215–1221. doi:10.1164/rccm.200703-489OC. ISSN 1535-4970. PMID 17872489.
- ↑ Shin MS, Ho KJ (1993). "Bronchiectasis in patients with alpha 1-antitrypsin deficiency. A rare occurrence?". Chest. 104 (5): 1384–86. doi:10.1378/chest.104.5.1384. PMID 8222792. S2CID 72998738.
- ↑ Martínez-García, Miguel Ángel; Soler-Cataluña, Juan José; Donat Sanz, Yolanda; Catalán Serra, Pablo; Agramunt Lerma, Marcos; Ballestín Vicente, Javier; Perpiñá-Tordera, Miguel (November 2011). "Factors associated with bronchiectasis in patients with COPD". Chest. 140 (5): 1130–1137. doi:10.1378/chest.10-1758. ISSN 1931-3543. PMID 21546440.
- ↑ Goeminne, P. C.; Nawrot, T. S.; Ruttens, D.; Seys, S.; Dupont, L. J. (February 2014). "Mortality in non-cystic fibrosis bronchiectasis: a prospective cohort analysis". Respiratory Medicine. 108 (2): 287–296. doi:10.1016/j.rmed.2013.12.015. ISSN 1532-3064. PMID 24445062.
- 1 2 Chalmers, James D.; Chang, Anne B.; Chotirmall, Sanjay H.; Dhar, Raja; McShane, Pamela J. (15 November 2018). "Bronchiectasis". Nature Reviews. Disease Primers. 4 (1): 45. doi:10.1038/s41572-018-0042-3. ISSN 2056-676X. PMID 30442957.
- ↑ Catanzano, Tara (5 September 2005). "Primary Tuberculosis". eMedicine Specialties Encyclopedia. Connecticut: WebMD. Archived from the original on 5 June 2007. Retrieved 2007-06-22.
- ↑ John M Holbert. "Bronchiectasis Imaging". Medscape. Archived from the original on 2017-08-15. Retrieved 2017-08-15. Updated: Oct 13, 2015
- 1 2 Pasteur, M. C.; Bilton, D.; Hill, A. T.; British Thoracic Society Bronchiectasis non-CF Guideline Group (July 2010). "British Thoracic Society guideline for non-CF bronchiectasis". Thorax. 65 Suppl 1: i1–58. doi:10.1136/thx.2010.136119. ISSN 1468-3296. PMID 20627931.
- ↑ Polverino, Eva; Goeminne, Pieter C.; McDonnell, Melissa J.; Aliberti, Stefano; Marshall, Sara E.; Loebinger, Michael R.; Murris, Marlene; Cantón, Rafael; Torres, Antoni; Dimakou, Katerina; De Soyza, Anthony (September 2017). "European Respiratory Society guidelines for the management of adult bronchiectasis". The European Respiratory Journal. 50 (3): 1700629. doi:10.1183/13993003.00629-2017. ISSN 1399-3003. PMID 28889110.
- ↑ Crofton J (1966). "Diagnosis and Treatment of Bronchiectasis: I. Diagnosis". Br Med J. 1 (5489): 721–3 contd. doi:10.1136/bmj.1.5489.721. PMC 1844268. PMID 5909486.
- ↑ Onen ZP, Eris Gulbay B, Sen E, Akkoca Yildiz O, Saryal S, Acican T, Karabiyikoglu G (2007). "Analysis of the factors related to mortality in patients with bronchiectasis". Respir. Med. 101 (7): 1390–97. doi:10.1016/j.rmed.2007.02.002. PMID 17374480.
- 1 2 Chalmers, James D.; Aliberti, Stefano; Blasi, Francesco (May 2015). "Management of bronchiectasis in adults". The European Respiratory Journal. 45 (5): 1446–1462. doi:10.1183/09031936.00119114. ISSN 1399-3003. PMID 25792635.
- ↑ José, RJ; Brown, JS (October 2014). "Bronchiectasis". British Journal of Hospital Medicine. 75 Suppl 10: C146-51. doi:10.12968/hmed.2014.75.Sup10.C146. PMID 25289486.
- ↑ Flude, Lizzie J.; Agent, Penny; Bilton, Diana (June 2012). "Chest physiotherapy techniques in bronchiectasis". Clinics in Chest Medicine. 33 (2): 351–361. doi:10.1016/j.ccm.2012.02.009. ISSN 1557-8216. PMID 22640850.
- ↑ Hill, Adam T.; Barker, Alan F.; Bolser, Donald C.; Davenport, Paul; Ireland, Belinda; Chang, Anne B.; Mazzone, Stuart B.; McGarvey, Lorcan (April 2018). "Treating Cough Due to Non-CF and CF Bronchiectasis With Nonpharmacological Airway Clearance: CHEST Expert Panel Report". Chest. 153 (4): 986–993. doi:10.1016/j.chest.2018.01.014. ISSN 1931-3543. PMC 6689075. PMID 29355548.
- 1 2 McIlwaine, Maggie; Bradley, Judy; Elborn, J. Stuart; Moran, Fidelma (January 2017). "Personalising airway clearance in chronic lung disease". European Respiratory Review. 26 (143): 160086. doi:10.1183/16000617.0086-2016. ISSN 1600-0617. PMID 28223396.
- 1 2 Polverino, Eva; Goeminne, Pieter C.; McDonnell, Melissa J.; Aliberti, Stefano; Marshall, Sara E.; Loebinger, Michael R.; Murris, Marlene; Cantón, Rafael; Torres, Antoni; Dimakou, Katerina; De Soyza, Anthony (September 2017). "European Respiratory Society guidelines for the management of adult bronchiectasis". The European Respiratory Journal. 50 (3): 1700629. doi:10.1183/13993003.00629-2017. ISSN 1399-3003. PMID 28889110.
- ↑ Kapur, Nitin; Petsky, Helen L.; Bell, Scott; Kolbe, John; Chang, Anne B. (16 May 2018). "Inhaled corticosteroids for bronchiectasis". The Cochrane Database of Systematic Reviews. 5: CD000996. doi:10.1002/14651858.CD000996.pub3. ISSN 1469-493X. PMC 6494510. PMID 29766487.
- ↑ Hill, Adam T; Pasteur, Mark; Cornford, Charles; Welham, Sally; Bilton, Diana (1 January 2011). "Primary care summary of the British Thoracic Society Guideline on the management of non-cystic fibrosis bronchiectasis". Primary Care Respiratory Journal. 20 (2): 135–40. doi:10.4104/pcrj.2011.00007. PMC 6549837. PMID 21336465.
- ↑ Elborn JS, Johnston B, Allen F, Clarke J, McGarry J, Varghese G (1992). "Inhaled steroids in patients with bronchiectasis". Respir Med. 86 (2): 121–4. doi:10.1016/S0954-6111(06)80227-1. PMID 1615177.
- ↑ Chang, Anne B.; Bell, Scott C.; Torzillo, Paul J.; King, Paul T.; Maguire, Graeme P.; Byrnes, Catherine A.; Holland, Anne E.; O'Mara, Peter; Grimwood, Keith; extended voting group (2015-01-19). "Chronic suppurative lung disease and bronchiectasis in children and adults in Australia and New Zealand Thoracic Society of Australia and New Zealand guidelines". The Medical Journal of Australia. 202 (1): 21–23. doi:10.5694/mja14.00287. ISSN 1326-5377. PMID 25588439.
- ↑ Brodt, Alessandra Monteiro; Stovold, Elizabeth; Zhang, Linjie (August 2014). "Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review". The European Respiratory Journal. 44 (2): 382–393. doi:10.1183/09031936.00018414. ISSN 1399-3003. PMID 24925920.
- ↑ Goyal, Vikas; Chang, Anne B. (2014-06-10). "Combination inhaled corticosteroids and long-acting beta2-agonists for children and adults with bronchiectasis". The Cochrane Database of Systematic Reviews (6): CD010327. doi:10.1002/14651858.CD010327.pub2. ISSN 1469-493X. PMC 6483496. PMID 24913725.
- 1 2 Agasthian, T.; Deschamps, C.; Trastek, V. F.; Allen, M. S.; Pairolero, P. C. (October 1996). "Surgical management of bronchiectasis". The Annals of Thoracic Surgery. 62 (4): 976–978, discussion 979–980. doi:10.1016/0003-4975(96)00469-9. ISSN 0003-4975. PMID 8823075.
- ↑ Zhang, Peng; Jiang, Gening; Ding, Jiaan; Zhou, Xiao; Gao, Wen (July 2010). "Surgical treatment of bronchiectasis: a retrospective analysis of 790 patients". The Annals of Thoracic Surgery. 90 (1): 246–250. doi:10.1016/j.athoracsur.2010.03.064. ISSN 1552-6259. PMID 20609785.
- ↑ Weycker, Derek; Hansen, Gary L.; Seifer, Frederic D. (November 2017). "Prevalence and incidence of noncystic fibrosis bronchiectasis among US adults in 2013". Chronic Respiratory Disease. 14 (4): 377–384. doi:10.1177/1479972317709649. ISSN 1479-9731. PMC 5729734. PMID 28555504.
- 1 2 Chandrasekaran, Ravishankar; Mac Aogáin, Micheál; Chalmers, James D.; Elborn, Stuart J.; Chotirmall, Sanjay H. (2018-05-22). "Geographic variation in the aetiology, epidemiology and microbiology of bronchiectasis". BMC Pulmonary Medicine. 18 (1): 83. doi:10.1186/s12890-018-0638-0. ISSN 1471-2466. PMC 5964678. PMID 29788932.
- ↑ "Bronchiectasis, Chapter 4, Dean E. Schraufnagel (ed.)". Breathing in America: Diseases, Progress, and Hope. American Thoracic Society. 2010. Archived from the original on 2017-04-15. Retrieved 2017-04-30.
- ↑ Roguin, A (2006). "Rene Theophile Hyacinthe Laënnec (1781–1826): The Man Behind the Stethoscope". Clin Med Res. 4 (3): 230–35. doi:10.3121/cmr.4.3.230. PMC 1570491. PMID 17048358.
- ↑ Wrong O (2003). "Osler and my father". J R Soc Med. 96 (6): 462–64. doi:10.1258/jrsm.96.9.462. PMC 539606. PMID 12949207.
- ↑ "Bronchiectasis | Definition of Bronchiectasis by Lexico". Lexico Dictionaries | English. Archived from the original on 2019-11-09. Retrieved 2019-11-21.
External links
| Wikisource has the text of the 1911 Encyclopædia Britannica article Bronchiectasis. |
| Classification | |
|---|---|
| External resources |