Autoimmune inner ear disease
| Autoimmune inner ear disease | |
|---|---|
| Other names | AIED |
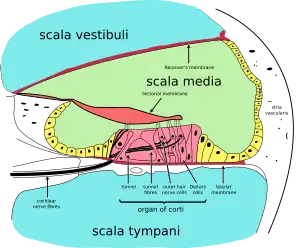 | |
| Cochlea, which is affected by this condition | |
| Specialty | Audiology, immunology |
Autoimmune inner ear disease was first defined by Dr. Brian McCabe in a landmark paper describing an autoimmune loss of hearing.[1] The disease results in progressive sensorineural hearing loss (SNHL) that acts bilaterally and asymmetrically, and sometimes affects an individual's vestibular system. AIED is used to describe any disorder in which the inner ear is damaged as a result of an autoimmune response.[2] Some examples of autoimmune disorders that have presented with AIED are Cogan's syndrome, relapsing polychondritis, systemic lupus erythematosus, granulomatosis with polyangiitis, polyarteritis nodosa, Sjogren's syndrome, and Lyme disease.[3]
Research has come to the consensus that AIED is the result of antibodies or other immune cells that cause damage to structures of the inner ear such as the cochlea and vestibular system. Of note, AIED is the only known SNHL that responds to medical treatment, but withholding treatment for longer than three months may result in permanent hearing loss and the need for cochlear implant installation.[4]
Although AIED has been studied extensively over the past 25 years, no clear mechanism of pathogenesis has emerged. A recent paper[5] performed a literature review of all relevant articles dating back to 1980, and proposed a mechanism of pathogenesis which includes an inflammatory response and immune cell attack on inner ear structures. This response leads to an over-activation of other immune cells such as T helper cells, resulting in vascular changes and cochlear harm. AIED appears to be a consequence of damaged sensorineural hearing due to electrochemical disturbances, microthrombosis, and immune cell deposition. Additionally, self-reactive antibodies and T-cells contribute to the aforementioned damage. Research has suggested a valuable next step in uncovering AIED pathogenesis is inquiry into the role of interleukin-1β (IL-1β).[6][7]
Signs and symptoms
Signs and symptoms of AIED are:[3]
- Progressive hearing loss in both ears
- Typically will begin in one ear and gradually affect the other
- Hearing loss may begin suddenly
- Tinnitus (ringing or buzzing in ears)
- Decrease in word recognition capability
- Loss of balance (vestibular symptoms)
- Degree of balance loss can change throughout the course of the disease
Causes
AIED is generally caused by either antibodies or immune cells that cause damage to the inner ear. There are several theories that propose a cause of AIED:
- Bystander damage – Physical damage to the inner ear may lead to cytokine release that signals for an immune response. This may be a component of the "attack/remission cycle" of Meniere's disease.[8]
- Cross-reactions – Accidental damage of the inner ear by antibodies or T-cells that recognize an inner ear antigen that is similar to a bacterial or viral antigen[9]
- Genetic factors – Predisposition to developing an autoimmune disorder based on genes inherited[9]
- Intolerance – The immune system may not be aware of all the antigens present in the inner ear until physical damage releases some of these antigens. As a result, the immune system treats these unfamiliar antigens as foreign and mounts an immune response.[9]
Currently, the cross-reactions theory appears to be the favored mechanism of AIED pathogenesis.[10]
Diagnosis
Since AIED symptoms are fairly common to many hearing loss disorders, it may be difficult to diagnose AIED without performing multiple medical tests. Some examples of these tests include:[10]
- Hearing Tests for Progressive Hearing and Balance loss
- Audiometry (measure of hearing acuity and sound intensity)
- Rotatory Chair Test (determines if inner ear is responsible for balance loss)
- Electrocochleography (ECOG) (recording of electrical potential in inner ear due to sound)
- Blood Tests for General Autoimmune Diseases
- Erythrocyte sedimentation rate (test for inflammation)
- Rheumatoid Factor (indicator of autoimmune disorders)
There are also blood tests specific to inner ear disorders:
- Anti-cochlear antibody test (testing for antibodies against cochlear cells)
- Lymphocyte Transformation Assay (testing whether an individual has developed a T-cell response against a certain drug)[11]
Though it has also been proposed that the use of anti heat shock protein 70 antibodies may be useful in the detection and diagnosis of AIED, there is not enough evidence to confirm the reliability of this method.[12]
Treatment
AIED treatment is a rapidly changing field. Several medical therapies have been proposed in the treatment of AIED, with corticosteroid therapy being the most effective. However, corticosteroid therapy (specifically with prednisone and dexamethasone) has demonstrated limited effectiveness in some patients, suggesting the need for novel treatment methods. The goal of most AIED treatments is to administer corticosteroids over a certain period of time, re-evaluate hearing at each appointment, and eventually taper off corticosteroid administration. Ideally, patients can be tapered off with hearing fully recovered, though this is the least likely outcome. Often, tumor necrosis factor-α (TNF-α) inhibitors must be administered alongside corticosteroids to achieve a favorable outcome and eventual end to corticosteroid treatment. Recent papers have indicated that the TNF-α inhibitor, infliximab, has the potential to allow for sustained patient improvement and alleviation of symptoms.[6][13][14]
Cytotoxic agents such as cyclophosphamide and methotrexate have been used in AIED treatment in the past; however, findings have suggested limited symptom alleviation from these drugs.[6][15]
References
- ↑ McCabe, Brian (September 1979). "Autoimmune sensorineural hearing loss". Annals of Otology, Rhinology, and Laryngology. 88 (5 Pt 1): 585–9. doi:10.1177/000348947908800501. PMID 496191. S2CID 21133298.
- ↑ "Autoimmune Inner Ear Disease | Vestibular Disorders Association". vestibular.org. 2012-03-07. Retrieved 2016-02-11.
- 1 2 "Autoimmune Inner Ear Disease". www.asha.org. Archived from the original on 2016-02-16. Retrieved 2016-02-11.
- ↑ "Autoimmune Inner Ear Disease (AIED) | American Hearing Research Foundation". american-hearing.org. Retrieved 2016-02-11.
- ↑ Goodall, A. F.; Siddiq, M. A. (2015-10-01). "Current understanding of the pathogenesis of autoimmune inner ear disease: a review". Clinical Otolaryngology. 40 (5): 412–419. doi:10.1111/coa.12432. ISSN 1749-4486. PMID 25847404. S2CID 41616626.
- 1 2 3 Rauch, Steven D. (2014-09-01). "IL-1β inhibition in autoimmune inner ear disease: can you hear me now?". The Journal of Clinical Investigation. 124 (9): 3685–3687. doi:10.1172/JCI77197. ISSN 1558-8238. PMC 4151210. PMID 25133418.
- ↑ Zhao, Ruijuan; Zhou, Hongyan; Su, Shao Bo (2013-11-01). "A critical role for interleukin-1β in the progression of autoimmune diseases". International Immunopharmacology. 17 (3): 658–669. doi:10.1016/j.intimp.2013.08.012. ISSN 1878-1705. PMID 24012439.
- ↑ Greco, A.; Gallo, A.; Fusconi, M.; Marinelli, C.; Macri, G.F.; Vincentiis, M. de (2012). "Meniere's disease might be an autoimmune condition?". Autoimmunity Reviews. 11 (10): 731–738. doi:10.1016/j.autrev.2012.01.004. PMID 22306860.
- 1 2 3 Kommareddi, Pavan K.; Nair, Thankam S.; Vallurupalli, Mounica; Telian, Steven A.; Arts, H. Alexander; El-Kashlan, Hussam K.; Sataloff, Robert T.; Carey, Thomas E. (2009-05-01). "Autoantibodies to recombinant human CTL2 in autoimmune hearing loss". The Laryngoscope. 119 (5): 924–932. doi:10.1002/lary.20136. ISSN 1531-4995. PMC 4128554. PMID 19319905.
- 1 2 "Autoimmune Inner Ear Disease (AIED) | American Hearing Research Foundation". american-hearing.org. Retrieved 2016-02-11.
- ↑ Pichler, Werner J. (2014-01-01). "Lymphocyte Transformation Test". In Vohr, Hans-Werner (ed.). Encyclopedia of Immunotoxicology. Springer Berlin Heidelberg. pp. 1–5. doi:10.1007/978-3-642-27786-3_924-5. ISBN 9783642277863.
- ↑ Ianuale, Carolina; Cadoni, Gabriella; De Feo, Emma; Liberati, Luca; Simo, Rachel Kamgaing; Paludetti, Gaetano; Ricciardi, Walter; Boccia, Stefania (2013-02-01). "A systematic review and meta-analysis of the diagnostic accuracy of anti-heat shock protein 70 antibodies for the detection of autoimmune hearing loss". Otology & Neurotology. 34 (2): 214–219. doi:10.1097/MAO.0b013e31827d0b8b. ISSN 1537-4505. PMID 23295728. S2CID 1580427.
- ↑ Heywood, R. L.; Hadavi, S.; Donnelly, S.; Patel, N. (2013-11-01). "Infliximab for autoimmune inner ear disease: case report and literature review". The Journal of Laryngology and Otology. 127 (11): 1145–1147. doi:10.1017/S002221511300217X. ISSN 1748-5460. PMID 24125068. S2CID 7912213.
- ↑ Gazeau, Pierre; Saraux, Alain; Devauchelle-Pensec, Valérie; Cornec, Divi (2014-09-01). "Long-term efficacy of infliximab in autoimmune sensorineural hearing loss associated with rheumatoid arthritis". Rheumatology (Oxford, England). 53 (9): 1715–1716. doi:10.1093/rheumatology/keu025. ISSN 1462-0332. PMID 24625506.
- ↑ Broughton, Shelley S.; Meyerhoff, William E.; Cohen, Stanley B. (2004-10-01). "Immune-mediated inner ear disease: 10-year experience". Seminars in Arthritis and Rheumatism. 34 (2): 544–548. doi:10.1016/j.semarthrit.2004.07.001. ISSN 0049-0172. PMID 15505770.