Desquamation
| Desquamation | |
|---|---|
| Other names: Skin peeling | |
 | |
| Skin peeling in scarlet fever | |
| Specialty | Dermatology |
| Symptoms | Scales, flaky skin, itch, irritation, or not noticeable[1] |
| Complications | Typically none, bacterial infections, dehydration[1] |
| Causes | Eczema, scarlet fever, staphylococcal scalded skin syndrome, toxic shock syndrome, Kawasaki disease, sunburn, radiation treatment,[1] dandruff and seborrheic dermatitis[2] |
| Treatment | Often none, moisturiser, treat underlying condition[1] |
Desquamation, or peeling skin, is the shedding of dead cells from the outermost layer of skin.[3] It is typically seen following injury or infection of skin, and in some inflammatory skin conditions.[1] It is a characteristic feature of dandruff and seborrheic dermatitis.[2] Where there is no injury or underlying skin condition, peeling is not typically noticeable.[4] It may appear as scaly or flaky skin, and may be itchy or feel irritated.[1]
Desquamation occurs when enzymes in the stratum corneum cleave adhesion proteins between cells, resulting in a gradual shedding of cells as they lose their stickiness.[3] Conditions in which skin may peel include eczema, scarlet fever, staphylococcal scalded skin syndrome, toxic shock syndrome and Kawasaki disease.[1] Sunburn, in addition to burns from chemicals, direct flames or radiation treatment may cause skin to peel.[1] It may occur in an allergic reaction, following irritation from a fabric or after using some treatments for acne and treatments containing retinol.[1]
Definition
Desquamation is the shedding of dead cells from the outermost layer of skin.[3] The term is from Latin desquamare 'to scrape the scales off a fish'.
Physiologic desquamation
Keratinocytes are the predominant cells of the epidermis, the outermost layer of the skin. Living keratinocytes reside in the basal, spinous, or granular layers of the epidermis. The outermost layer of the epidermis is called the stratum corneum and it is composed of terminally differentiated keratinocytes, the corneocytes. In the absence of disease, desquamation occurs when corneocytes are individually shed unnoticeably from the surface of the skin.[5] Typically the time it takes for a corneocyte to be formed and then shed is about 14 weeks but this time can vary depending on the anatomical location that the skin is covering. For example, desquamation occurs more slowly at acral (palm and sole) surfaces and more rapidly where the skin is thin, such as the eyelids. Normal desquamation can be visualized by immersing skin in warm or hot water. This induces the outermost layer of corneocytes to shed, such as is the case after a hot shower or bath.
Corneocytes are held together by corneodesmosomes. In order for desquamation to occur these corneodesmosome connections must be degraded.[5] Keratinocytes residing in the stratum granulosum produce corneodesmosome-degrading kallikrein family members, especially KLK1, KLK5, and KLK7.[6] Kallikreins are serine proteases. They are packaged within lamellar bodies and released into the intercellular space between the keratinocytes as they transition into becoming corneocytes.[5] To prevent premature desquamation, granular layer keratincoytes also produce kallikrein-inhibitory proteins.[6] At acral surfaces, desquamation occurs more slowly because granular layer keratinocytes downregulate expression of KLK1 and KLK7 and upregulate expression of protease inhibitors, including the KLK5-specific SPINK9 and the cysteine protease inhibitors CSTA and CST3.[6] Slowing the process of corneocyte desquamation allows acral (palm and sole) skin to form a thick protective stratum corneum.[6]
Abnormal desquamation
Scale forms on the skin surface in various disease settings, and is the result of abnormal desquamation. In pathologic desquamation, such as that seen in X-linked ichthyosis, the stratum corneum becomes thicker (hyperkeratosis), imparting a "dry" or scaly appearance to the skin, and instead of detaching as single cells, corneocytes are shed in clusters, which forms visible scales.[5] Desquamation of the epidermis may result from disease or injury of the skin. For example, once the rash of measles fades, there is desquamation. Skin peeling typically follows healing of a first degree burn or sunburn. Toxic shock syndrome, a potentially fatal immune system reaction to a bacterial infection such as Staphylococcus aureus,[7] can cause severe desquamation; so can mercury poisoning. Other serious skin diseases involving extreme desquamation include Stevens–Johnson syndrome and toxic epidermal necrolysis (TEN).[8] Radiation can cause dry or moist desquamation.[9] Desquamation is also abnormal in patients with immune-mediated skin diseases such as psoriasis and atopic dermatitis.[6] Abnormal desquamation often results in scale formation on the skin's surface.[6] Lipid composition alterations in scale have been used to construct diagnostic models for human skin disease.[6]
Images
Burns
 Skin peeling following sunburn
Skin peeling following sunburn Skin peeling following burn
Skin peeling following burn.jpg.webp) Skin peeling following burn
Skin peeling following burn
Scarlet fever
 Skin peeling in scarlet fever
Skin peeling in scarlet fever Skin peeling in scarlet fever
Skin peeling in scarlet fever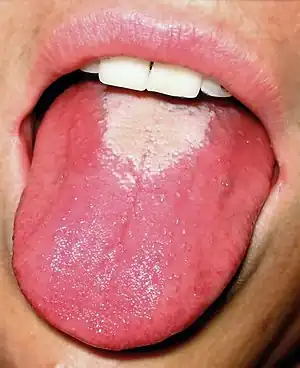 White coating sheds: strawberry tongue
White coating sheds: strawberry tongue Complete shedding of white coating: red strawberry tongue
Complete shedding of white coating: red strawberry tongue
Stevens–Johnson syndrome
 Stevens–Johnson syndrome
Stevens–Johnson syndrome Moist desquamation in Stevens–Johnson syndrome
Moist desquamation in Stevens–Johnson syndrome
Other conditions
.jpg.webp) Skin peeling in hand foot and mouth disease
Skin peeling in hand foot and mouth disease Peeling of gums
Peeling of gums Toxic epidermal hemolysis
Toxic epidermal hemolysis Palmar dyshidrosis
Palmar dyshidrosis
Eyes
Certain eye tissues, including the conjunctiva and cornea, may undergo pathological desquamation in diseases such as dry eye syndrome.[10] The anatomy of the human eye makes desquamation of the lens impossible.[11]
See also
References
- 1 2 3 4 5 6 7 8 9 Hogan, Lilianna. "What to Know About Peeling Skin (Desquamation)". WebMD. Archived from the original on 19 January 2023. Retrieved 19 January 2023.
- 1 2 Borda, LJ; Wikramanayake, TC (December 2015). "Seborrheic Dermatitis and Dandruff: A Comprehensive Review". Journal of clinical and investigative dermatology. 3 (2). doi:10.13188/2373-1044.1000019. PMID 27148560. Archived from the original on 2023-01-19. Retrieved 2023-01-19.
- 1 2 3 Miller, Claire; Crampin, Edmund; Osborne, James M. (August 2022). "Multiscale modelling of desquamation in the interfollicular epidermis". PLoS computational biology. 18 (8): e1010368. doi:10.1371/journal.pcbi.1010368. ISSN 1553-7358. PMID 36037236. Archived from the original on 2023-01-19. Retrieved 2023-01-19.
- ↑ Milstone, Leonard M. (December 2004). "Epidermal desquamation". Journal of Dermatological Science. 36 (3): 131–140. doi:10.1016/j.jdermsci.2004.05.004. ISSN 0923-1811. PMID 15541634. Archived from the original on 2023-01-19. Retrieved 2023-01-19.
- 1 2 3 4 Jackson, Simon M.; Williams, Mary L.; Feingold, Kenneth R.; Elias, Peter M. (1993). "Pathobiology of the Stratum Corneum". The Western Journal of Medicine. 158 (3): 279–85. PMC 1311754. PMID 8460510.
- 1 2 3 4 5 6 7 Merleev, Alexander A.; Le, Stephanie T.; Alexanian, Claire; Toussi, Atrin; Xie, Yixuan; Marusina, Alina I.; Watkins, Steven M.; Patel, Forum; Billi, Allison C.; Wiedemann, Julie; Izumiya, Yoshihiro; Kumar, Ashish; Uppala, Ranjitha; Kahlenberg, J. Michelle; Liu, Fu-Tong (2022-08-22). "Biogeographic and disease-specific alterations in epidermal lipid composition and single-cell analysis of acral keratinocytes". JCI Insight. 7 (16): e159762. doi:10.1172/jci.insight.159762. ISSN 2379-3708. PMC 9462509. PMID 35900871.
- ↑ Dinges, MM; Orwin, PM; Schlievert, PM (January 2000). "Exotoxins of Staphylococcus aureus". Clinical Microbiology Reviews. 13 (1): 16–34, table of contents. doi:10.1128/cmr.13.1.16. PMC 88931. PMID 10627489.
- ↑ Parillo, Steven J; Parillo, Catherine V. (2010-05-25). "Stevens-Johnson Syndrome". eMedicine. Medcape. Archived from the original on 2011-10-12. Retrieved 2010-09-06.
- ↑ Centers for Disease Control and Prevention (2005-06-30). "Cutaneous Radiation Injury". CDC. Archived from the original on 2019-06-05. Retrieved 2011-05-15.
- ↑ Gilbard, Jeffrey P. (November 1, 2003). "Dry Eye: Natural History, Diagnosis and Treatment". Wolters Kluwer Pharma Solutions. Archived from the original on January 30, 2013. Retrieved February 3, 2012.
- ↑ Lynnerup, Niels; Kjeldsen, Henrik; Heegaard, Steffen; Jacobsen, Christina; Heinemeier, Jan (2008). Gazit, Ehud (ed.). "Radiocarbon Dating of the Human Eye Lens Crystallines Reveal Proteins without Carbon Turnover throughout Life". PLOS ONE. 3 (1): e1529. Bibcode:2008PLoSO...3.1529L. doi:10.1371/journal.pone.0001529. PMC 2211393. PMID 18231610.
External links
| Classification |
|---|