Gallstone ileus
| Gallstone ileus | |
|---|---|
| Video explanation | |
| Specialty | Gastroenterology |
| Symptoms | Abdominal pain, vomiting, constipation, yellowish skin[1] |
| Complications | Sepsis, pancreatitis.[1] |
| Usual onset | Age > 60[1] |
| Causes | Obstruction of the bowels by a gallstone[1] |
| Risk factors | Gallstone > 2 cm, recurrent cholecystitis[1] |
| Diagnostic method | Medical imaging[1] |
| Differential diagnosis | Pancreatitis, bile duct stone, peptic ulcer disease, bile duct cancer[1] |
| Treatment | Surgery[1] |
| Frequency | 0.4% of people with gallstones[1] |
Gallstone ileus is a form of bowel obstruction caused by a gallstone within the gastrointestinal tract.[1] Symptoms may include abdominal pain that come and go, vomiting, and constipation.[1] Less commonly yellowish skin may occur.[1] Complications can include sepsis and pancreatitis.[1]
Risk factors include gallstones larger than 2 cm and recurrent episodes of cholecystitis.[1] The underlying mechanism involves inflammation resulting in the formation of a connection between the gallbladder and gastrointestinal tract through which gallstones can than pass.[1] These gallstones can than become stuck, most commonly in the lower part of the ileum.[1] Diagnosis may occur by medical imaging.[1]
Treatment is by surgery.[1] Surgery may involve removing the gallstone, closing the hole between the gallbladder and gastrointestinal tract, and removing the gallbladder.[1] Often only the first part is initial performed with a second surgery if symptoms continue.[1] The risk of death is about 20%.[1]
Gallstone ileus occurs in about 4 in 1,000 people with gallstones.[1] Women are three times more commonly affected than men.[1] It is more common in those over the age of 60.[1] The condition was first described by Thomas Bartholin in 1654.[1]
Signs and symptoms
Symptoms may include abdominal pain that come and go, vomiting, and constipation.[1] Less commonly yellowish skin may occur.[1] Complications can include sepsis and pancreatitis.[1]
Cause
It is believed to be due to impaction of a gallstone in the gastrointestinal tract after having gone through a biliary-enteric fistula.[2]
Diagnosis
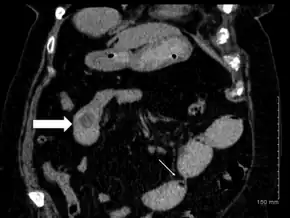
Diagnosis of gallstone ileus requires radiographic studies. Classic radiographic findings are known as Rigler's triad:[3]
- pneumobilia (air within the biliary tree)
- evidence of small bowel obstruction
- radiopaque gallstone on abdominal radiograph
Treatment
Initial management involves fluid resuscitation and potentially nasogastric suctioning.[4] Since gallstone ileus constitutes a form of mechanical small bowel obstruction, it can be a surgical emergency and requires open or laparoscopic surgery to remove an impacted stone.[4] The different strategies for surgical management are either enterolithotomy alone, allowing a delayed cholecystectomy after an inflammation-free period of 4–6 weeks (and therefore two-stage surgery) or enterolithotomy in combination with a cholecystectomy and fistula division (one-stage surgery). The different strategies for surgical management are controversial, and depend on factors such as patient fitness for surgery and comorbidities.[5]
Terminology
Bouveret's syndrome refers to reverse gallstone ileus where the gallstone propagates proximally and causes gastric outlet obstruction by being impacted in first part of duodenum.
The name "gallstone ileus" is a misnomer because an ileus is, by definition, a non-mechanical bowel motility failure (as opposed to a mechanical obstruction by a stone).
References
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 Turner, AR; Sharma, B; Mukherjee, S (January 2020). "Gallstone Ileus". PMID 28613584.
{{cite journal}}: Cite journal requires|journal=(help) - ↑ Turner, Anisha R.; Sharma, Bashar; Mukherjee, Sandeep (2022). "Gallstone Ileus". StatPearls. StatPearls Publishing. Archived from the original on 5 July 2022. Retrieved 19 August 2022.
- ↑ Ibrahim, Dalia; Gaillard, Frank. "Rigler's Triad". Radiopaedia. Archived from the original on 18 December 2013. Retrieved 17 December 2013.
- 1 2 Longo, DL; Fauci, AS; Kasper, DL; Hauser, SL; Jameson, JL; Loscalzo, J (2015). Harrison's Principles of Internal Medicine (19 ed.). New York: McGraw-Hill. pp. 2081–2082. ISBN 978-0-07-180216-1. Archived from the original on 17 December 2013. Retrieved 3 March 2017.
- ↑ Fitzgerald J, Fitzgerald L, Maxwell-Armstrong C, Brooks A (2009). "Recurrent gallstone ileus: time to change our surgery?". Journal of Digestive Diseases. 10 (2): 149–151. doi:10.1111/j.1751-2980.2009.00378.x. PMID 19426399.
External links
| Classification |
|---|