HIV/AIDS research
HIV/AIDS research includes all medical research that attempts to prevent, treat, or cure HIV/AIDS, as well as fundamental research about the nature of HIV as an infectious agent and AIDS as the disease caused by HIV.
Transmission
A body of scientific evidence has shown that men who are circumcised are less likely to contract HIV than men who are uncircumcised.[1] Research published in 2014 concludes that the sex hormones estrogen and progesterone selectively impact HIV transmission.[2]
Pre- and post-exposure prophylaxis
"Pre-exposure prophylaxis" refers to the practice of taking some drugs before being exposed to HIV infection, and having a decreased chance of contracting HIV as a result of taking that drug. Post-exposure prophylaxis refers to taking some drugs quickly after being exposed to HIV, while the virus is in a person's body but before the virus has established itself. In both cases, the drugs would be the same as those used to treat persons with HIV, and the intent of taking the drugs would be to eradicate the virus before the person becomes irreversibly infected.
Post-exposure prophylaxis is recommended in anticipated cases of HIV exposure, such as if a nurse somehow has blood-to-blood contact with a patient in the course of work, or if someone without HIV requests the drugs immediately after having unprotected sex with a person who might have HIV. Pre-exposure prophylaxis is sometimes an option for HIV-negative persons who feel that they are at increased risk of HIV infection, such as an HIV-negative person in a serodiscordant relationship with an HIV-positive partner.
Current research in these agents include drug development, efficacy testing, and practice recommendations for using drugs for HIV prevention.
Within-host dynamics
The within-host dynamics of HIV infection include the spread of the virus in vivo, the establishment of latency, the effects of immune response on the virus, etc.[3][4] Early studies used simple models and only considered the cell-free spreading of HIV, in which virus particles bud from an infected T cell, enter the blood/extracellular fluid, and then infect another T cell.[4] A 2015 study[3] proposes a more realistic model of HIV dynamics that also incorporates the viral cell-to-cell spreading mechanism, where the virus is directly transited from one cell to another, as well as the T cell activation, the cellular immune response, and the immune exhaustion as the infection progresses.[3]
Virus characteristics
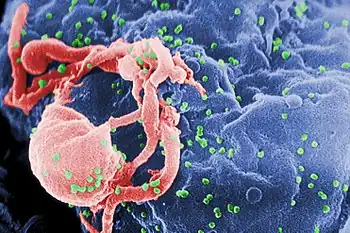
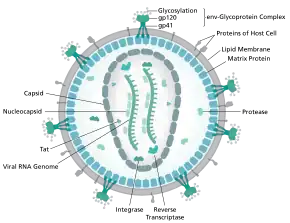
HIV binds to immune cell surface receptors, including CD 4 and CXCR4 or CD4 and CCR5. The binding causes conformation changes and results in the membrane fusion between HIV and cell membrane. Active infection occurs in most cells, while latent infection occurs in much fewer cells 1, 2 and at very early stages of HIV infection. 9, 35 In active infection, HIV pro virus is active and HIV virus particles are actively replicated; and the infected cells continuously release viral progeny; while in latent infection, HIV pro virus is transcriptionally silenced and no viral progeny is produced.[5]
Management of HIV/AIDS
Research to improve current treatments includes decreasing side effects of current drugs, further simplifying drug regimens to improve adherence, and determining better sequences of regimens to manage drug resistance. There are variations in the health community in recommendations on what treatment doctors should recommend for people with HIV. One question, for example, is determining when a doctor should recommend that a patient take antiretroviral drugs and what drugs a doctor may recommend. This field also includes the development of antiretroviral drugs.
Age acceleration effects due to HIV-1 infection
Infection with the Human Immunodeficiency Virus-1 (HIV) is associated with clinical symptoms of accelerated aging, as evidenced by increased incidence and diversity of age-related illnesses at relatively young ages. A significant age acceleration effect could be detected in brain (7.4 years) and blood (5.2 years) tissue due to HIV-1 infection[6] with the help of a biomarker of aging, which is known as epigenetic clock.
Long-term nonprogressor
A long-term nonprogressor is a person who is infected with HIV, but whose body, for whatever reason, naturally controls the virus so that the infection does not progress to the AIDS stage. Such persons are of great interest to researchers, who feel that a study of their physiologies could provide a deeper understanding of the virus and disease. There are also two cases where HIV was apparently entirely cleared by a person's immune system without a therapy.[7]
HIV vaccine
An HIV vaccine is a vaccine that would be given to a person who does not have HIV, in order to confer protection against subsequent exposures to HIV, thus reducing the likelihood that the person would become infected by HIV. Currently, no effective HIV vaccine exists. Various HIV vaccines have been tested in clinical trials almost since the discovery of HIV.
Only a vaccine is thought to be able to halt the pandemic. This is because a vaccine would cost less, thus being affordable for developing countries, and would not require daily treatment.[8] However, after over 20 years of research, HIV-1 remains a difficult target for a vaccine.[8][9]
In 2003 a clinical trial in Thailand tested an HIV vaccine called RV 144. In 2009, the researchers reported that this vaccine showed some efficacy in protecting recipients from HIV infection (31% efficiency). Results of this trial give the first supporting evidence of any vaccine being effective in lowering the risk of contracting HIV. Other vaccine trials continue worldwide including a mosaic vaccine using an adenovirus 26 vector[10] as well as a newer formulation of RV144 called HVTN 702.[11]
One recent trial was conducted by scientists at The Scripps Research Institute (TSRI) who found a way to attach HIV-fighting antibodies to immune cells, creating a HIV-resistant cell population.[12]
HIV cure
Three people have been reported cured of AIDS.[13][14][15] In 2019, the NIH and Bill & Melinda Gates Foundation announced making $200 million available for broad-based, multi-prong scientific efforts focused on developing a global cure for AIDS as well as for sickle cell disease, with NIH Director Francis S. Collins saying, "We aim to go big or we go home."[16] In 2020, Dr. Tony Fauci’s division at NIH, NIAID, issued its first solicitation exclusively focused on methods to cure HIV infection.[17] These announcements from NIH are not limited to stem cell therapies.
Excision is a biotechnology company with a first-in-human CRISPR-based one-time gene therapy to be evaluated in individuals with HIV.[18] Research Foundation to Cure AIDS is the first 501(c)(3) non-for-profit organization with a royalty-free license to research, develop and commercialize a cell engineering technology in the field of curing AIDS on a pro bono basis.[19][20]
Microbicides for sexually transmitted diseases
A microbicide for sexually transmitted diseases is a gel which would be applied to the skin – perhaps a rectal microbicide for persons who engage in anal sex or a vaginal microbicide for persons who engage in vaginal sex – and if infected body fluid such as blood or semen were to touch the gel, then HIV in that fluid would be destroyed and the people having sex would be less likely to spread infection between themselves.
On March 7, 2013, the Washington University in St. Louis website published a report by Julia Evangelou Strait, in which it was reported that ongoing nanoparticle research showed that nanoparticles loaded with various compounds could be used to target infectious agents whilst leaving healthy cells unaffected. In the study detailed by this report, it was found that nanoparticles loaded with Mellitin, a compound found in Bee venom, could deliver the agent to the HIV, causing the breakdown of the outer protein envelope of the virus. This, they say, could lead to the production of a vaginal gel which could help prevent infection by disabling the virus.[21] Dr Joshua Hood goes on to explain that beyond preventive measures in the form of a topical gel, he sees "potential for using nanoparticles with melittin as therapy for existing HIV infections, especially those that are drug-resistant. The nanoparticles could be injected intravenously and, in theory, would be able to clear HIV from the blood stream."[21]
Initial stem cell cures of HIV/AIDS
In 2007, Timothy Ray Brown,[22] a 40-year-old HIV-positive man, also known as "the Berlin Patient", was given a stem cell transplant as part of his treatment for acute myeloid leukemia (AML).[23] A second transplant was made a year later after a relapse. The donor was chosen not only for genetic compatibility but also for being homozygous for a CCR5-Δ32 mutation that confers resistance to HIV infection.[24][25] After 20 months without antiretroviral drug treatment, it was reported that HIV levels in Brown's blood, bone marrow, and bowel were below the limit of detection.[25] The virus remained undetectable over three years after the first transplant.[23] Although the researchers and some commentators have characterized this result as a cure, others suggest that the virus may remain hidden in tissues[26] such as the brain (which acts as a viral reservoir).[27] Stem cell treatment remains investigational because of its anecdotal nature, the disease and mortality risk associated with stem cell transplants, and the difficulty of finding suitable donors.[26][28]
Strategies to develop broadly-applicable cures
Scientists have been using different approaches of stem cell based gene therapy in an attempt to develop a cure as well as to propose an alternative to the conventional antiretroviral therapy (ART).[29] Specifically, advances had been made with a cure to HIV.
A cellular receptor, generally CCR5 or CXCR4 is required in order for HIV entry into CD4 cells. Cells of individuals homozygous for the CCR5 gene variant Δ32 (CCR5Δ32/Δ32) lack the CCR5 cell-surface expression, meaning that they are naturally resistant to infection with CCR5 tropic HIV strains (R5 HIV).[30] One study done in 2011 achieves successful CD4+ T-cell reconstitution as a result of CCR5Δ32/Δ32 stem cell transplantation at the systemic level and in the gut mucosal immune system in a patient with HIV. Additionally, it provides evidence for the reduction in the size of the potential HIV reservoir over time. The patient in this study even remained HIV free without any evidence of having it for more than 3.5 years.[23]
Other theoretical cures to HIV-1 have been proposed. One supposed cure to HIV-1 involves the creation of a disease-resistant immune system through transplantation of autologous, gene-modified (HIV-1-resistant) hematopoietic stem cells and progenitor cells (GM-HSPC). Though this study does involve several early stage clinical trials that have demonstrated the safety and feasibility of this technique only for HIV-1, none have resulted in improvement of the disease state itself.[31] Therefore, this strategy is intended to go alongside already existing treatment techniques such as drugs and vaccines. However, future technology regarding this approach of single treatment cell therapy could potentially replace current therapy altogether as a functional or sterilizing cure to HIV-1.[31]
An additional study involves the use of genetically engineered CD34+ hematopoietic stem and progenitor cells. Experimental long-term in vivo HIV gene therapy have had huge issues due to both transduction ending in multiple copies of heterologous DNA in target cells as well as low efficacy of cell transduction at the time of transplantation. This study demonstrated the efficacy of a transplantation approach that ultimately allows for an enriched population of HSPCs expressing a single copy of a CCR5 miRNA.[32] Since positive selection of modified cells is likely to be insufficient below the threshold they found of at least 70% of the HIV target cells resulting in gene modification from efficient maintenance of CD34+ T cell and a low viral titer, the findings show evidence that clinical protocols of HIV gene therapy require a selective enrichment of genetically targeted cells.[32]
Immunomodulatory agents
Complementing efforts to control viral replication, immunotherapies that may assist in the recovery of the immune system have been explored in past and ongoing trials, including IL-2 and IL-7.[33]
The failure of vaccine candidates to protect against HIV infection and progression to AIDS has led to a renewed focus on the biological mechanisms responsible for HIV latency. A limited period of therapy combining anti-retrovirals with drugs targeting the latent reservoir may one day allow for total eradication of HIV infection.[34] Researchers have discovered an abzyme that can destroy the protein gp120 CD4 binding site. This protein is common to all HIV variants as it is the attachment point for B lymphocytes and subsequent compromising of the immune system.[35]
New developments
A turning point for HIV research occurred in 2007, following the bone marrow transplant of HIV sufferer Timothy Ray Brown. Brown underwent the procedure after he developed leukaemia and the donor of the bone marrow possessed a rare genetic mutation that caused Brown's cells to become resistant to HIV. Brown attained the title of the "Berlin Patient" in the HIV research field and is the first man to have been cured of the virus. As of April 2013, two primary approaches are being pursued in the search for a HIV cure: The first is gene therapy that aims to develop a HIV-resistant immune system for patients, and the second is being led by Danish scientists, who are conducting clinical trials to strip the HIV from human DNA and have it destroyed permanently by the immune system.[36]
Three more cases with similarities to the Brown case have occurred since the 2007 discovery; however, they differ because the transplanted marrow has not been confirmed as mutated. Two of the cases were publicized in a July 2013 CNN story that relayed the experience of two patients who had taken antiretroviral therapy for years before they developed lymphoma, a cancer of the lymph nodes. They then underwent lymphoma chemotherapy and bone marrow transplantation, while remaining on an antiretroviral regimen; while they retained traces of HIV four months afterwards, six to nine months after the transplant, the two patients had no detectable trace of HIV in their blood. However, the managing clinician Dr. Timothy Heinrich stated at the Malaysian International AIDS Society Conference where the findings were presented:
It's possible, again, that the virus could return in a week, it could return in a month—in fact, some mathematical modeling predicts that virus could even return one to two years after we stop antiretroviral therapy, so we really don't know what the long-term or full effects of stem cell transplantation and viral persistence is.[37]
In 2014, Dr Warner C. Greene and Dr Gilad Doitsh at the Gladstone Institutes identified pyroptosis as the predominant mechanism that causes the two signature pathogenic events in HIV infection––CD4 T-cell depletion and chronic inflammation.[38][39][40] Identifying pyroptosis may provide novel therapeutic opportunities targeting caspase-1, which controls the pyroptotic cell death pathway. Specifically, these findings could open the door to an entirely new class of "anti-AIDS" therapies that act by targeting the host rather than the virus.[41] Recently, pyroptosis and downstream pathways were also identified as promising targets for treatment of severe coronavirus disease 2019–associated diseases.[42]
In March 2016, researchers at Temple University, Philadelphia, reported that they have used genome editing to delete HIV from T cells. According to the researchers, this approach could lead to a dramatic reduction of the viral load in patient cells.[43][44]
In April 2016, it was announced the publication of a preclinical animal study using SupT1 cells as a decoy target for the HIV virus,[45][46] aiming to move infection from the patient's cells to the inoculated cells, and therefore to induce the virus to become less aggressive by replicating in such permissive cells.
In March 2019, a patient with Hodgkin's lymphoma was also reported to possibly have been cured using similar treatment to Brown.[47]
In 2022, Moderna announced that the first participants have been vaccinated in a Phase 1 clinical trial of an experimental HIV vaccine that utilizes Moderna's mRNA technology.[48]
See also
- Discovery and development of CCR5 receptor antagonists
- Discovery and development of HIV-protease inhibitors
- Discovery and development of non-nucleoside reverse-transcriptase inhibitors
- Broadly neutralizing HIV-1 antibodies
- Innate resistance to HIV
- Health interventions
- HIV superinfection
- History of HIV/AIDS
- Sex education
References
- ↑ "Male Circumcision". Centers for Disease Control and Prevention. U.S. Department of Health & Human Services. 8 November 2019. Archived from the original on 16 July 2022. Retrieved 15 July 2022.
- ↑ Goode D, Aravantinou M, Jarl S, Truong R, Derby N, Guerra-Perez N, et al. (May 15, 2014). "Sex hormones selectively impact the endocervical mucosal microenvironment: implications for HIV transmission". PLOS ONE. 9 (5): e97767. Bibcode:2014PLoSO...997767G. doi:10.1371/journal.pone.0097767. PMC 4022654. PMID 24830732.
- 1 2 3 Zhang C, Zhou S, Groppelli E, Pellegrino P, Williams I, Borrow P, et al. (April 2015). "Hybrid spreading mechanisms and T cell activation shape the dynamics of HIV-1 infection". PLOS Computational Biology. 11 (4): e1004179. arXiv:1503.08992. Bibcode:2015PLSCB..11E4179Z. doi:10.1371/journal.pcbi.1004179. PMC 4383537. PMID 25837979.
- 1 2 Perelson AS, Ribeiro RM (September 2013). "Modeling the within-host dynamics of HIV infection". BMC Biology. 11 (1): 96. doi:10.1186/1741-7007-11-96. PMC 3765939. PMID 24020860.
- ↑ Ophinni Y, Inoue M, Kotaki T, Kameoka M (May 2018). "CRISPR/Cas9 system targeting regulatory genes of HIV-1 inhibits viral replication in infected T-cell cultures". Scientific Reports. 8 (1): 7784. Bibcode:2018NatSR...8.7784O. doi:10.1038/s41598-018-26190-1. PMC 5958087. PMID 29773895.
- ↑ Horvath S, Levine AJ (November 2015). "HIV-1 Infection Accelerates Age According to the Epigenetic Clock". The Journal of Infectious Diseases. 212 (10): 1563–73. doi:10.1093/infdis/jiv277. PMC 4621253. PMID 25969563.
- ↑ "Rare case of woman's body ridding itself of HIV". BBC News. 2021-11-16. Archived from the original on 2021-11-16. Retrieved 2021-11-16.
- 1 2 Ferrantelli F, Cafaro A, Ensoli B (December 2004). "Nonstructural HIV proteins as targets for prophylactic or therapeutic vaccines". Current Opinion in Biotechnology. 15 (6): 543–56. doi:10.1016/j.copbio.2004.10.008. PMID 15560981.
- ↑ Karlsson Hedestam GB, Fouchier RA, Phogat S, Burton DR, Sodroski J, Wyatt RT (February 2008). "The challenges of eliciting neutralizing antibodies to HIV-1 and to influenza virus". Nature Reviews. Microbiology. 6 (2): 143–55. doi:10.1038/nrmicro1819. PMID 18197170.
- ↑ "HPX2008/ HVTN 705". AVAC. 2017-01-19. Archived from the original on 2019-01-22. Retrieved 2019-02-13.
- ↑ "HVTN 702". AVAC. 2015-04-17. Archived from the original on 2019-01-22. Retrieved 2019-02-13.
- ↑ "First-in-human clinical trial confirms novel HIV vaccine approach developed by IAVI and Scripps Research". Archived from the original on 2021-11-30. Retrieved 2022-07-15.
- ↑ McNeil Jr DG (2008-11-14). "Rare Treatment Is Reported to Cure AIDS Patient". The New York Times. ISSN 0362-4331. Archived from the original on 2021-12-12. Retrieved 2021-09-24.
- ↑ Mandavilli A (2020-03-09). "The 'London Patient,' Cured of H.I.V., Reveals His Identity". The New York Times. ISSN 0362-4331. Archived from the original on 2021-09-27. Retrieved 2021-09-24.
- ↑ Mandavilli, Apoorva (15 February 2022). "A Woman Is Cured of H.I.V. Using a Novel Treatment". The New York Times. Archived from the original on 25 June 2022. Retrieved 15 July 2022.
- ↑ "NIH launches new collaboration to develop gene-based cures for sickle cell disease and HIV on global scale". National Institutes of Health (NIH). 2019-10-23. Archived from the original on 2021-09-04. Retrieved 2021-09-24.
- ↑ "RFA-AI-20-076: New Technologies for the In vivo Delivery of Gene Therapeutics for an HIV Cure (R01 Clinical Trial Not Allowed)". grants.nih.gov. Archived from the original on 2021-09-18. Retrieved 2021-09-24.
- ↑ Armstrong A (17 September 2021). "Excision's CRISPR gene editing therapy for HIV is heading into human testing after FDA clearance". FierceBiotech. Archived from the original on 2021-09-24. Retrieved 2021-09-24.
- ↑ Shekdar K (22 September 2021). "Novel cell engineering method for drug discovery, biologics and cell therapy". sciencex.com. Archived from the original on 2021-09-24. Retrieved 2021-09-24.
- ↑ Shekdar K, Langer J, Venkatachalan S, Schmid L, Anobile J, Shah P, et al. (May 2021). "Cell engineering method using fluorogenic oligonucleotide signaling probes and flow cytometry". Biotechnology Letters. 43 (5): 949–958. doi:10.1007/s10529-021-03101-5. PMC 7937778. PMID 33683511.
- 1 2 Strait JE (7 March 2013). "Nanoparticles loaded with bee venom kill HIV". Archived from the original on 2 February 2016. Retrieved 15 July 2022.
- ↑ "German HIV patient cured after stem cell transplant". Belfast Telegraph. December 15, 2010. Archived from the original on December 22, 2013. Retrieved December 15, 2010.
- 1 2 3 Allers K, Hütter G, Hofmann J, Loddenkemper C, Rieger K, Thiel E, Schneider T (March 2011). "Evidence for the cure of HIV infection by CCR5Δ32/Δ32 stem cell transplantation". Blood. 117 (10): 2791–9. doi:10.1182/blood-2010-09-309591. PMID 21148083.
- ↑ Schoofs M (November 7, 2008). "A Doctor, a Mutation and a Potential Cure for AIDS". The Wall Street Journal. Archived from the original on 2013-09-16. Retrieved 2008-11-09.
- 1 2 Hütter G, Nowak D, Mossner M, Ganepola S, Müssig A, Allers K, et al. (February 2009). "Long-term control of HIV by CCR5 Delta32/Delta32 stem-cell transplantation". The New England Journal of Medicine. 360 (7): 692–8. doi:10.1056/NEJMoa0802905. PMID 19213682.
- 1 2 Levy JA (February 2009). "Not an HIV cure, but encouraging new directions". The New England Journal of Medicine. 360 (7): 724–5. doi:10.1056/NEJMe0810248. PMID 19213687.
- ↑ Nath A, Clements JE (March 2011). "Eradication of HIV from the brain: reasons for pause". AIDS. 25 (5): 577–80. doi:10.1097/QAD.0b013e3283437d2f. PMC 3681810. PMID 21160414.(subscription required)
- ↑ van Lunzen J, Fehse B, Hauber J (June 2011). "Gene therapy strategies: can we eradicate HIV?". Current HIV/AIDS Reports. 8 (2): 78–84. doi:10.1007/s11904-011-0073-9. PMID 21331536. S2CID 43463970.(subscription required)
- ↑ Younan P, Kowalski J, Kiem HP (February 2014). "Genetically modified hematopoietic stem cell transplantation for HIV-1-infected patients: can we achieve a cure?". Molecular Therapy. 22 (2): 257–264. doi:10.1038/mt.2013.264. PMC 3916050. PMID 24220323.
- ↑ Dean M, Carrington M, Winkler C, Huttley GA, Smith MW, Allikmets R, et al. (September 1996). "Genetic restriction of HIV-1 infection and progression to AIDS by a deletion allele of the CKR5 structural gene. Hemophilia Growth and Development Study, Multicenter AIDS Cohort Study, Multicenter Hemophilia Cohort Study, San Francisco City Cohort, ALIVE Study". Science. 273 (5283): 1856–62. Bibcode:1996Sci...273.1856D. doi:10.1126/science.273.5283.1856. PMID 8791590. S2CID 21160580. Archived from the original on 2022-04-08. Retrieved 2022-07-15.
- 1 2 DiGiusto DL, Stan R, Krishnan A, Li H, Rossi JJ, Zaia JA (November 2013). "Development of hematopoietic stem cell based gene therapy for HIV-1 infection: considerations for proof of concept studies and translation to standard medical practice". Viruses. 5 (11): 2898–919. doi:10.3390/v5112898. PMC 3856421. PMID 24284880.
- 1 2 Myburgh R, Ivic S, Pepper MS, Gers-Huber G, Li D, Audigé A, et al. (July 2015). "Lentivector Knockdown of CCR5 in Hematopoietic Stem and Progenitor Cells Confers Functional and Persistent HIV-1 Resistance in Humanized Mice". Journal of Virology. 89 (13): 6761–72. doi:10.1128/JVI.00277-15. PMC 4468501. PMID 25903342.
- ↑ Tincati C, d'Arminio Monforte A, Marchetti G (January 2009). "Immunological mechanisms of interleukin-2 (IL-2) treatment in HIV/AIDS disease". Current Molecular Pharmacology. 2 (1): 40–5. doi:10.2174/1874467210902010040. PMID 20021444.
- ↑ Bowman MC, Archin NM, Margolis DM (February 2009). "Pharmaceutical approaches to eradication of persistent HIV infection". Expert Reviews in Molecular Medicine. 11 (e6): e6. doi:10.1017/S1462399409000970. PMID 19208267. S2CID 9620595.
- ↑ Planque S, Nishiyama Y, Taguchi H, Salas M, Hanson C, Paul S (June 2008). "Catalytic antibodies to HIV: physiological role and potential clinical utility". Autoimmunity Reviews. 7 (6): 473–9. doi:10.1016/j.autrev.2008.04.002. PMC 2527403. PMID 18558365.
- ↑ Simons JW (27 April 2013). "Scientists on brink of HIV cure". The Telegraph. Archived from the original on 27 April 2013. Retrieved 2 May 2013.
- ↑ Young S (3 July 2013). "Patients HIV-free for now after transplant". CNN. Archived from the original on 17 December 2013. Retrieved 4 July 2013.
- ↑ Doitsh, Gilad; Galloway, Nicole LK; Geng, Xin; Yang, Zhiyuan; Monroe, Kathryn M.; Zepeda, Orlando; Hunt, Peter W.; Hatano, Hiroyu; Sowinski, Stefanie; Muñoz-Arias, Isa; Greene, Warner C. (2014-01-23). "Pyroptosis drives CD4 T-cell depletion in HIV-1 infection". Nature. 505 (7484): 509–514. doi:10.1038/nature12940. ISSN 0028-0836. PMC 4047036. PMID 24356306.
- ↑ Monroe, Kathryn M.; Yang, Zhiyuan; Johnson, Jeffrey R.; Geng, Xin; Doitsh, Gilad; Krogan, Nevan J.; Greene, Warner C. (2014-01-24). "IFI16 DNA Sensor Is Required for Death of Lymphoid CD4 T-cells Abortively Infected with HIV". Science. 343 (6169): 428–432. Bibcode:2014Sci...343..428M. doi:10.1126/science.1243640. ISSN 0036-8075. PMC 3976200. PMID 24356113.
- ↑ Doitsh, Gilad; Greene, Warner C. (2016-03-09). "Dissecting How CD4 T Cells Are Lost During HIV Infection". Cell Host & Microbe. 19 (3): 280–291. doi:10.1016/j.chom.2016.02.012. ISSN 1934-6069. PMC 4835240. PMID 26962940.
- ↑ "Gladstone Labs". Gladstone Labs. Archived from the original on 2021-06-08. Retrieved 2022-03-14.
- ↑ Yap, Jeremy K. Y.; Moriyama, Miyu; Iwasaki, Akiko (2020-07-15). "Inflammasomes and pyroptosis as therapeutic targets for COVID-19". Journal of Immunology. 205 (2): 307–312. doi:10.4049/jimmunol.2000513. ISSN 0022-1767. PMC 7343621. PMID 32493814.
- ↑ Kaminski R, Chen Y, Fischer T, Tedaldi E, Napoli A, Zhang Y, et al. (March 2016). "Elimination of HIV-1 Genomes from Human T-lymphoid Cells by CRISPR/Cas9 Gene Editing". Scientific Reports. 6: 22555. Bibcode:2016NatSR...622555K. doi:10.1038/srep22555. PMC 4778041. PMID 26939770.
- ↑ Dvorsky G (22 March 2016). "HIV Genes Successfully Edited Out of Immune Cells". Gizmodo. Archived from the original on 22 March 2016. Retrieved 23 March 2016.
- ↑ Fior, Jonathan (2016-04-26). "SupT1 Cell Infusion as a Possible Cell-Based Therapy for HIV: Results from a Pilot Study in Hu-PBMC BRGS Mice". Vaccines. 4 (2): E13. doi:10.3390/vaccines4020013. ISSN 2076-393X. PMC 4931630. PMID 27128948. Archived from the original on 2022-07-02. Retrieved 2022-07-15.
- ↑ "Innovative Bioresearch announces publication of pioneering pilot study exploring SupT1 cell infusion as a cell-based therapy for HIV in humanized mice". Medical News Today. Archived from the original on 2022-07-05. Retrieved 2022-07-05.
- ↑ Brueck H (6 March 2019). "Scientists may have cured a man of HIV by injecting him with 'superpower' cells. Here's what it means for the future of AIDS treatment". Business Insider. Archived from the original on 6 March 2019. Retrieved 6 March 2019.
- ↑ Anokhi Saklecha. "First patients vaccinated in clinical trial of HIV vaccine that uses Moderna's mRNA technology". CNN. Archived from the original on 2022-03-14. Retrieved 2022-03-14.
External links
- HIV and AIDS News Archived 2022-07-17 at the Wayback Machine (ScienceDaily)
- HIV and AIDS News Archived 2022-06-10 at the Wayback Machine (Medical News Today)
- Treatment Action Group – Clinical Trials Archived 2022-06-24 at the Wayback Machine