Mucus
Mucus (/ˈmjuːkəs/ MEW-kəs) is a slippery aqueous secretion produced by, and covering, mucous membranes. It is typically produced from cells found in mucous glands, although it may also originate from mixed glands, which contain both serous and mucous cells. It is a viscous colloid containing inorganic salts, antimicrobial enzymes (such as lysozymes), immunoglobulins (especially IgA), and glycoproteins such as lactoferrin[1] and mucins, which are produced by goblet cells in the mucous membranes and submucosal glands. Mucus serves to protect epithelial cells in the linings of the respiratory, digestive, and urogenital systems, and structures in the visual and auditory systems from pathogenic fungi, bacteria[2] and viruses. Most of the mucus in the body is produced in the gastrointestinal tract.
Amphibians, fish, snails, slugs, and some other invertebrates also produce external mucus from their epidermis as protection against pathogens, and to help in movement and is also produced in fish to line their gills. Plants produce a similar substance called mucilage that is also produced by some microorganisms.[3]
Respiratory system
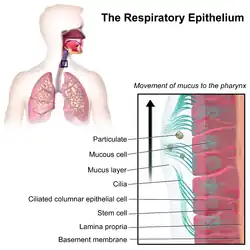
In the human respiratory system, mucus is part of the airway surface liquid (ASL), also known as epithelial lining fluid (ELF), that lines most of the respiratory tract. The airway surface liquid consists of a sol layer termed the periciliary liquid layer and an overlying gel layer termed the mucus layer. The periciliary liquid layer is so named as it surrounds the cilia and lies on top of the surface epithelium.[4][5][6] The periciliary liquid layer surrounding the cilia consists of a gel meshwork of cell-tethered mucins and polysaccharides.[7] The mucus blanket aids in the protection of the lungs by trapping foreign particles before they enter them, in particular through the nose during normal breathing.[8]
Mucus is made up of a fluid component of around 95% water, the mucin secretions from the goblet cells, and the submucosal glands (2–3% glycoproteins), proteoglycans (0.1–0.5%), lipids (0.3–0.5%), proteins, and DNA.[7] The major mucins secreted – MUC5AC and MUC5B - are large polymers that give the mucus its rheologic or viscoelastic properties.[7][4] MUC5AC is the main gel-forming mucin secreted by goblet cells, in the form of threads and thin sheets. MUC5B is a polymeric protein secreted from submucosal glands and some goblet cells, and this is in the form of strands.[9][10]
In the airways – the trachea, bronchi, and bronchioles -- the lining of mucus is produced by specialized airway epithelial cells called goblet cells, and submucosal glands. Small particles such as dust, particulate pollutants, and allergens, as well as infectious agents and bacteria are caught in the viscous nasal or airway mucus and prevented from entering the system. This process, together with the continual movement of the cilia on the respiratory epithelium toward the oropharynx (mucociliary clearance), helps prevent foreign objects from entering the lungs during breathing. This explains why coughing often occurs in those who smoke cigarettes. The body's natural reaction is to increase mucus production. In addition, mucus aids in moisturizing the inhaled air and prevents tissues such as the nasal and airway epithelia from drying out.[11]
Mucus is produced continuously in the respiratory tract. Mucociliary action carries it down from the nasal passages and up from the rest of the tract to the pharynx, with most of it being swallowed subconsciously. Sometimes in times of respiratory illness or inflammation, mucus can become thickened with cell debris, bacteria, and inflammatory cells. It is then known as phlegm which may be coughed up as sputum to clear the airway.[12][13]
Respiratory tract
Increased mucus production in the upper respiratory tract is a symptom of many common ailments, such as the common cold, and influenza. Nasal mucus may be removed by blowing the nose or by using nasal irrigation. Excess nasal mucus, as with a cold or allergies, due to vascular engorgement associated with vasodilation and increased capillary permeability caused by histamines,[14] may be treated cautiously with decongestant medications. Thickening of mucus as a "rebound" effect following overuse of decongestants may produce nasal or sinus drainage problems and circumstances that promote infection.
During cold, dry seasons, the mucus lining nasal passages tends to dry out, meaning that mucous membranes must work harder, producing more mucus to keep the cavity lined. As a result, the nasal cavity can fill up with mucus. At the same time, when air is exhaled, water vapor in breath condenses as the warm air meets the colder outside temperature near the nostrils. This causes an excess amount of water to build up inside nasal cavities. In these cases, the excess fluid usually spills out externally through the nostrils.[15]

In the lower respiratory tract impaired mucociliary clearance due to conditions such as primary ciliary dyskinesia may result in mucus accumulation in the bronchi.[16] The dysregulation of mucus homeostasis is the fundamental characteristic of cystic fibrosis, an inherited disease caused by mutations in the CFTR gene, which encodes a chloride channel. This defect leads to the altered electrolyte composition of mucus, which triggers its hyperabsorption and dehydration. Such low-volume, viscous, acidic mucus has a reduced antimicrobial function, which facilitates bacterial colonisation.[17] The thinning of the mucus layer ultimately affects the periciliary liquid layer, which becomes dehydrated, compromising ciliary function, and impairing mucociliary clearance.[16][17] A respiratory therapist can recommend airway clearance therapy which uses a number of clearance techniques to help with the clearance of mucus.[18]
Mucus hypersecretion
In the lower respiratory tract excessive mucus production in the bronchi and bronchioles is known as mucus hypersecretion.[10] Chronic mucus hypersecretion results in the chronic productive cough of chronic bronchitis,[19] and is generally synonymous with this.[20] Excessive mucus can narrow the airways, limit airflow, and accelerate a decline in lung function.[10]
Digestive system
In the human digestive system, mucus is used as a lubricant for materials that must pass over membranes, e.g., food passing down the esophagus. Mucus is extremely important in the gastrointestinal tract. It forms an essential layer in the colon and in the small intestine that helps reduce intestinal inflammation by decreasing bacterial interaction with intestinal epithelial cells.[21] The layer of mucus of the gastric mucosa lining the stomach is vital to protect the stomach lining from the highly acidic environment within it.[scientific 1]
Reproductive system
In the human female reproductive system, cervical mucus prevents infection and provides lubrication during sexual intercourse. The consistency of cervical mucus varies depending on the stage of a woman's menstrual cycle. At ovulation cervical mucus is clear, runny, and conducive to sperm; post-ovulation, mucus becomes thicker and is more likely to block sperm. Several Fertility Awareness methods rely on observation of cervical mucus, as one of three primary fertility signs, to identify a woman's fertile time at the mid-point of the cycle. Awareness of the woman's fertile time allows a couple to time intercourse to improve the odds of pregnancy. It is also proposed as a method to avoid pregnancy.[22]
Clinical significance
In general, nasal mucus is clear and thin, serving to filter air during inhalation. During times of infection, mucus can change color to yellow or green either as a result of trapped bacteria[23] or due to the body's reaction to viral infection. The green color of mucus comes from the heme group in the iron-containing enzyme myeloperoxidase secreted by white blood cells as a cytotoxic defense during a respiratory burst.
In the case of bacterial infection, the bacterium becomes trapped in already-clogged sinuses, breeding in the moist, nutrient-rich environment. Sinusitis is an uncomfortable condition which may include congestion of mucus. A bacterial infection in sinusitis will cause discolored mucus and would respond to antibiotic treatment; viral infections typically resolve without treatment.[24] Almost all sinusitis infections are viral and antibiotics are ineffective and not recommended for treating typical cases.[25]
In the case of a viral infection such as cold or flu, the first stage and also the last stage of the infection cause the production of a clear, thin mucus in the nose or back of the throat. As the body begins to react to the virus (generally one to three days), mucus thickens and may turn yellow or green. Viral infections cannot be treated with antibiotics, and are a major avenue for their misuse. Treatment is generally symptom-based; often it is sufficient to allow the immune system to fight off the virus over time.[26]
Obstructive lung diseases often result from impaired mucociliary clearance that can be associated with mucus hypersecretion, and these are sometimes referred to as mucoobstructive lung diseases.[27] Techniques of airway clearance therapy can help to clear secretions, maintain respiratory health, and prevent inflammation in the airways.[18]
A unique umbilical cord lining epithelial stem cell expresses MUC1, termed (CLEC-muc). This has been shown to have good potential in the regeneration of the cornea.[28][29]
Properties of mucus
Tunable swelling capacity
Mucus is able to absorb water or dehydrate through pH variations. The swelling capacity of mucus stems from the bottlebrush structure[30] of mucin within which hydrophilic segments provide a large surface area for water absorption. Moreover, the tunability of swelling effect is controlled by polyelectrolyte effect.
Polyelectrolyte effect in mucus
Polymers with charged molecules are called polyelectrolytes. Mucins, a kind of polyelectrolyte proteoglycans, are the main component of mucus, which provides the polyelectrolyte effect in mucus.[31] The process of inducing this effect comprises two steps: attraction of counter-ions and water compensation. When exposed in physiological ionic solution, the charged groups in the polyelectrolytes attract counter-ions with opposite charges, thereby leading to a solute concentration gradient. An osmotic pressure is introduced to equalize the concentration of solute throughout the system by driving water to flow from the low concentration areas to the high concentration areas. In short, the influx and outflux of water within mucus, managed by the polyelectrolyte effect, contribute to mucus' tunable swelling capacity.[32]
Mechanism of pH-tunable swelling
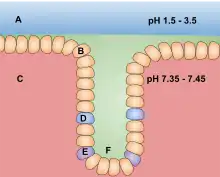
The ionic charges of mucin are mainly provided by acidic amino acids including aspartic acid (pKa=3.9) and glutamic acid (pKa=4.2). The charges of acidic amino acids will change with environmental pH value due to acid dissociation and association. Aspartic acid, for example, has a negative side chain when the pH value is above 3.9, while a neutrally charged side chain will be introduced as pH value drops below 3.9. Thus, the number of negative charges in mucus is influenced by the pH value of surrounding environment. That is, the polyelectrolyte effect of mucus is largely affected by the pH value of solution due to the charge variation of acidic amino acid residues on the mucin backbone. For instance, the charged residue on mucin is protonated at a normal pH value of the stomach, approximately pH 2. In this case, there is scarcely polyelectrolyte effect, thereby causing compact mucus with little swelling capacity. However, a kind of bacteria, Helicobacter pylori, is prone to producing base to elevate the pH value in stomach, leading to the deprotonation of aspartic acids and glutamic acids, i.e., from neutral to negative-charged. The negative charges in the mucus greatly increase, thus inducing the polyelectrolyte effect and the swelling of the mucus. This swelling effect increases the pore size of the mucus and decreases mucus' viscosity, which allows bacteria to penetrate and migrate into the mucus and cause disease.[33]
Charge selectivity
The high selective permeability of mucus plays a crucial role in the healthy state of human beings by limiting the penetration of molecules, nutrients, pathogens, and drugs. The charge distribution within mucus serves as a charge selective diffusion barrier, thus significantly affecting the transportation of agents. Among particles with various surface zeta potentials, cationic particles tend to have a low depth of penetration, neutral ones possess medium penetration, and anionic ones have the largest penetration depth. Furthermore, the effect of charge selectivity changes when the status of the mucus varies, i.e., native mucus has a threefold higher potential to limit agent penetration than purified mucus.[34]
Other animals
Mucus is also produced by a number of other animals.[35] All fish are covered in mucus secreted from glands all over their bodies.[36] Invertebrates such as snails and slugs secrete mucus called snail slime to enable movement, and to prevent their bodies from drying out. Their reproductive systems also make use of mucus for example in the covering of their eggs. In the unique mating ritual of Limax maximus the mating slugs lower themselves from elevated locations by a mucus thread. Mucus is an essential constituent of hagfish slime used to deter predators.[37] Mucus is produced by the endostyle in some tunicates and larval lampreys to help in filter feeding.
See also
- Alkaline mucus
- Empty nose syndrome
- Mucoadhesion
- Mucophagy
- Sniffle
- Spinnbarkeit
- Feces
Notes
- ↑ Purves, William. "Why don't our digestive acids corrode our stomach linings?". Scientific American. Retrieved 6 December 2012.
Second, HCl in the lumen doesn't digest the mucosa because goblet cells in the mucosa secrete large quantities of protective mucus that line the mucosal surface.
References
- ↑ Singh, PK; Parsek, MR; Greenberg, EP; Welsh, MJ (May 2002). "A component of innate immunity prevents bacterial biofilm development". Nature. 417 (6888): 552–555. Bibcode:2002Natur.417..552S. doi:10.1038/417552a. PMID 12037568. S2CID 4423528.
- ↑ Barr et al. Bacteriophage adhering to mucus provide a non–host-derived immunity PNAS 2013
- ↑ "Modes of locomotion in protists: 5 modes". biology discussion. 2016-09-06.
- 1 2 Atanasova, KR; Reznikov, LR (21 November 2019). "Strategies for measuring airway mucus and mucins". Respiratory Research. 20 (1): 261. doi:10.1186/s12931-019-1239-z. PMC 6873701. PMID 31752894.
- ↑ Althaus, M (March 2013). "ENaC inhibitors and airway re-hydration in cystic fibrosis: state of the art". Curr Mol Pharmacol. 6 (1): 3–12. doi:10.2174/18744672112059990025. PMID 23547930.
- ↑ Hiemstra, PS; McCray PB, Jr; Bals, R (April 2015). "The innate immune function of airway epithelial cells in inflammatory lung disease". The European Respiratory Journal. 45 (4): 1150–1162. doi:10.1183/09031936.00141514. PMC 4719567. PMID 25700381.
- 1 2 3 Ohar, JA; Donohue, JF; Spangenthal, S (23 October 2019). "The Role of Guaifenesin in the Management of Chronic Mucus Hypersecretion Associated with Stable Chronic Bronchitis: A Comprehensive Review". Chronic Obstructive Pulmonary Diseases. 6 (4): 341–349. doi:10.15326/jcopdf.6.4.2019.0139. PMC 7006698. PMID 31647856.
- ↑ Lillehoj, ER; Kim, KC (December 2002). "Airway mucus: its components and function". Archives of Pharmacal Research. 25 (6): 770–780. doi:10.1007/bf02976990. PMID 12510824. S2CID 21467111.
- ↑ Ostedgaard, LS; Moninger, TO; McMenimen, JD; Sawin, NM; Parker, CP; Thornell, IM; Powers, LS; Gansemer, ND; Bouzek, DC; Cook, DP; Meyerholz, DK; Abou Alaiwa, MH; Stoltz, DA; Welsh, MJ (27 June 2017). "Gel-forming mucins form distinct morphologic structures in airways". Proceedings of the National Academy of Sciences of the United States of America. 114 (26): 6842–6847. doi:10.1073/pnas.1703228114. PMC 5495256. PMID 28607090.
- 1 2 3 Shen, Y (2018). "Management of airway mucus hypersecretion in chronic airway inflammatory disease: Chinese expert consensus (English edition)". International Journal of Chronic Obstructive Pulmonary Disease. 13: 399–407. doi:10.2147/COPD.S144312. PMC 5796802. PMID 29430174.
- ↑ Thorton, DJ; Rousseau, K; MucGuckin, MA (2008). "Structure and function of the polymeric mucins in airways mucus". Annual Review of Physiology. 70 (44): 459–486. doi:10.1146/annurev.physiol.70.113006.100702. PMID 17850213.
- ↑ Rubin, BK (January 2010). "The role of mucus in cough research". Lung. 188 Suppl 1: S69–72. doi:10.1007/s00408-009-9198-7. PMID 19936981. S2CID 33857446.
- ↑ Hall, John (2011). Guyton and Hall textbook of medical physiology (Twelfth ed.). p. 473. ISBN 9781416045748.
- ↑ Monroe EW, Daly AF, Shalhoub RF (February 1997). "Appraisal of the validity of histamine-induced wheal and flare to predict the clinical efficacy of antihistamines". J. Allergy Clin. Immunol. 99 (2): S798–806. doi:10.1016/s0091-6749(97)70128-3. PMID 9042073.
- ↑ "Why Does Cold Weather Cause Runny Noses?". NPR. Retrieved 2011-09-22.
- 1 2 Mall, MA (March 2008). "Role of Cilia, Mucus, and Airway Surface Liquid in Mucociliary Dysfunction: Lessons from Mouse Models". Journal of Aerosol Medicine and Pulmonary Drug Delivery. 21 (1): 13–24. doi:10.1089/jamp.2007.0659. PMID 18518828. S2CID 18362681.
- 1 2 Haq, Iram J; Gray, Michael A; Garnett, James P; Ward, Christopher; Brodlie, Malcolm (March 2016). "Airway surface liquid homeostasis in cystic fibrosis: pathophysiology and therapeutic targets". Thorax. 71 (3): 284–287. doi:10.1136/thoraxjnl-2015-207588. PMID 26719229.
- 1 2 Volsko, TA (October 2013). "Airway clearance therapy: finding the evidence". Respiratory Care. 58 (10): 1669–1678. doi:10.4187/respcare.02590. PMID 24064626.
- ↑ Global Initiative for Chronic Obstructive Lung Disease – GOLD (PDF). 2018. p. 15. Retrieved 10 November 2019.
- ↑ Novartis Foundation (2002). Mucus hypersecretion in respiratory disease. Wiley. p. 3. ISBN 0470844787.
- ↑ Johansson, Malin E. V.; Gustafsson, Jenny K.; Sjöberg, Karolina E.; Petersson, Joel; Holm, Lena; Sjövall, Henrik; Hansson, Gunnar C. (2010-01-01). "Bacteria penetrate the inner mucus layer before inflammation in the dextran sulfate colitis model". PLOS ONE. 5 (8): e12238. Bibcode:2010PLoSO...512238J. doi:10.1371/journal.pone.0012238. ISSN 1932-6203. PMC 2923597. PMID 20805871.
- ↑ Han, Leo; Taub, Rebecca; Jensen, Jeffrey T. (November 2017). "Cervical mucus and contraception: what we know and what we don't". Contraception. 96 (5): 310–321. doi:10.1016/j.contraception.2017.07.168. PMID 28801053.
- ↑ "Runny Nose (with green or yellow mucus)". Get Smart: Know When Antibiotics Work. Centers for Disease Control and Prevention. March 9, 2006. Archived from the original on March 8, 2008.
- ↑ Consumer Reports; American Academy of Family Physicians (April 2012), "Treating sinusitis: Don't rush to antibiotics" (PDF), Choosing Wisely: an initiative of the ABIM Foundation, Consumer Reports, retrieved August 17, 2012
- ↑ American Academy of Family Physicians, presented by ABIM Foundation, "Five Things Physicians and Patients Should Question" (PDF), Choosing Wisely: an initiative of the ABIM Foundation, American Academy of Family Physicians, archived from the original (PDF) on June 24, 2012, retrieved August 14, 2012
- ↑ "Definition of Viral Infection". MedicineNet.com. Retrieved 2010-04-04.
- ↑ Lewis, BW; Patial, S; Saini, Y (2019). "Immunopathology of Airway Surface Liquid Dehydration Disease". Journal of Immunology Research. 2019: 2180409. doi:10.1155/2019/2180409. PMC 6664684. PMID 31396541.
- ↑ Saleh, R; Reza, HM (10 October 2017). "Short review on human umbilical cord lining epithelial cells and their potential clinical applications". Stem Cell Research & Therapy. 8 (1): 222. doi:10.1186/s13287-017-0679-y. PMC 5634865. PMID 29017529.
- ↑ Bains, KK; et al. (August 2019). "Recovering vision in corneal epithelial stem cell deficient eyes". Contact Lens & Anterior Eye : The Journal of the British Contact Lens Association. 42 (4): 350–358. doi:10.1016/j.clae.2019.04.006. PMC 6611221. PMID 31047800.
- ↑ Chremos, A; Douglas, JF (2018). "A comparative study of thermodynamic, conformational, and structural properties of bottlebrush with star and ring polymer melts". J. Chem. Phys. 149 (4): 044904. Bibcode:2018JChPh.149d4904C. doi:10.1063/1.5034794. PMID 30068167. S2CID 51894232.
- ↑ Sircar, S.; Keener, J. P.; Fogelson, A. L. (2013-01-07). "The effect of divalent vs. monovalent ions on the swelling of Mucin-like polyelectrolyte gels: Governing equations and equilibrium analysis". The Journal of Chemical Physics. 138 (1): 014901. Bibcode:2013JChPh.138a4901S. doi:10.1063/1.4772405. ISSN 0021-9606. PMC 3555968. PMID 23298059.
- ↑ Harding, S. E.; Creeth, J. M. (1983-07-28). "Polyelectrolyte behaviour in mucus glycoproteins". Biochimica et Biophysica Acta (BBA) - Protein Structure and Molecular Enzymology. 746 (1–2): 114–119. doi:10.1016/0167-4838(83)90017-1. ISSN 0006-3002. PMID 6871229.
- ↑ Celli, Jonathan P.; Turner, Bradley S.; Afdhal, Nezam H.; Keates, Sarah; Ghiran, Ionita; Kelly, Ciaran P.; Ewoldt, Randy H.; McKinley, Gareth H.; So, Peter (2009-08-25). "Helicobacter pylori moves through mucus by reducing mucin viscoelasticity". Proceedings of the National Academy of Sciences. 106 (34): 14321–14326. Bibcode:2009PNAS..10614321C. doi:10.1073/pnas.0903438106. ISSN 0027-8424. PMC 2732822. PMID 19706518.
- ↑ Crater, Jason S.; Carrier, Rebecca L. (2010-12-08). "Barrier Properties of Gastrointestinal Mucus to Nanoparticle Transport". Macromolecular Bioscience. 10 (12): 1473–1483. doi:10.1002/mabi.201000137. ISSN 1616-5195. PMID 20857389. S2CID 20013702.
- ↑ Rühs, Patrick A.; Bergfreund, Jotam; Bertsch, Pascal; Gstöhl, Stefan J.; Fischer, Peter (2021). "Complex fluids in animal survival strategies". Soft Matter. 17 (11): 3022–3036. arXiv:2005.00773. doi:10.1039/D1SM00142F. PMID 33729256.
- ↑ Dash, S; Das, SK; Samal, J; Thatoi, HN (Spring 2018). "Epidermal mucus, a major determinant in fish health: a review". Iranian Journal of Veterinary Research. 19 (2): 72–81. PMC 6056142. PMID 30046316.
- ↑ Böni, Lukas; Fischer, Peter; Böcker, Lukas; Kuster, Simon; Rühs, Patrick A. (September 2016). "Hagfish slime and mucin flow properties and their implications for defense". Scientific Reports. 6 (1): 30371. doi:10.1038/srep30371. PMC 4961968. PMID 27460842.
| Authority control: National libraries |
|---|