Periodontology
| Occupation | |
|---|---|
Occupation type | Specialty |
Activity sectors | Dentistry |
| Description | |
Education required | Dental degree |
Fields of employment | Hospitals, private practices |
Periodontology or periodontics (from Ancient Greek περί, perí – 'around'; and ὀδούς, odoús – 'tooth', genitive ὀδόντος, odóntos) is the specialty of dentistry that studies supporting structures of teeth, as well as diseases and conditions that affect them. The supporting tissues are known as the periodontium, which includes the gingiva (gums), alveolar bone, cementum, and the periodontal ligament. A periodontist is a dentist that specializes in the prevention, diagnosis and treatment of periodontal disease and in the placement of dental implants.[1]
The periodontium
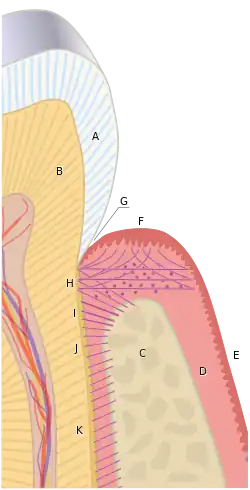
The term periodontium is used to describe the group of structures that directly surround, support and protect the teeth. The periodontium is composed largely of the gingival tissue and the supporting bone.[2]
Gingivae
Normal gingiva may range in color from light coral pink to heavily pigmented. The soft tissues and connective fibres that cover and protect the underlying cementum, periodontal ligament and alveolar bone are known as the gingivae. The gingivae are categorised into three anatomical groups: the free, attached and the interdental gingiva. Each of the gingival groups are considered biologically different; however, they are all specifically designed to help protect against mechanical and bacterial destruction.[3]
Free gingiva
The tissues that sit above the alveolar bone crest are considered the free gingiva. In healthy periodontium, the gingival margin is the fibrous tissue that encompasses the cemento-enamel junction, a line around the circumference of the tooth where the enamel surface of the crown meets the outer cementum layer of the root. A natural space called the gingival sulcus lies apically to the gingival margin, between the tooth and the free gingiva. A non-diseased, healthy gingival sulcus is typically 0.5-3mm in depth, however, this measurement can increase in the presence of periodontal disease. The gingival sulcus is lined by a non-keratinised layer called the oral sulcular epithelium; it begins at the gingival margin and ends at the base of the sulcus where the junctional epithelium and attached gingiva begins.[4]
Attached gingiva
The junctional epithelium is a collar-like band that lies at the base of the gingival sulcus and surrounds the tooth; it demarcates the areas of separation between the free and attached gingiva. The junctional epithelium provides a specialised protective barrier to microorganisms residing around the gingival sulcus.[4] Collagen fibres bind the attached gingiva tightly to the underlying periodontium including the cementum and alveolar bone and vary in length and width,[4] depending on the location in the oral cavity and on the individual.[5][6] The attached gingiva lies between the free gingival line or groove and the mucogingival junction. The attached gingiva dissipates functional and masticatory stresses placed on the gingival tissues during common activities such as mastication, tooth brushing and speaking.[7] In health it is typically pale pink or coral pink in colour and may present with surface stippling or racial pigmentation.[7]
Interdental gingiva
The interdental gingiva takes up the space beneath a tooth contact point, between two adjacent teeth. It is normally triangular or pyramidal in shape and is formed by two interdental papillae (lingual and facial).[4][5] The middle or centre part of the interdental papilla is made up of attached gingiva, whereas the borders and tip are formed by the free gingiva. The central point between the interdental papillae is called the col. It is a valley-like or concave depression that lies directly beneath the contact point, between the facial and lingual papilla.[6] However, the col may be absent if there is gingival recession or if the teeth are not contacting. The main purpose of the interdental gingiva is to prevent food impaction during routine mastication.[7]
Alveolar Mucosa
This area of tissue is non-keratinized and is located beyond the mucogingival junction. It is less firmly attached and is redder than attached gingiva. It provides for the movement of cheek and lips.[8]
Periodontal ligament
The periodontal ligament is the connective tissue that joins the outer layer of the tooth root, being the cementum, to the surrounding alveolar bone. It is composed of several complex fibre groups that run in different directions and which insert into the cementum and bone via Sharpey’s fibres.[4] The periodontal ligament is composed mostly of collagen fibres, however it also houses blood vessels and nerves within loose connective tissue.[6] Mechanical loads that are placed on the teeth during mastication and other external forces are absorbed by the periodontal ligament, which therefore protects the teeth within their sockets.[7]
Alveolar bone
In periodontal health, the alveolar bone surrounds the teeth and forms the bony socket that supports each tooth. The buccal and lingual plates and lining of the sockets are composed of thin, yet dense compact or cortical bone.[3] Within the cortical plates and dental sockets lies cancellous bone, a spongy or trabecular-type bone which is less dense than compact bone.[6]
Cementum
Cementum is the outer layer of the tooth root; it overlies the dentine layer of the tooth and provides attachment for the collagen fibres of the periodontal ligament. It also protects the dentine and provides a seal for the otherwise exposed ends of the dentinal tubules. It is not as hard as enamel or dentine and is typically a light yellow colour.[7]
Gingival diseases
Gingivitis is a common condition that affects the gingiva or mucosal tissues that surround the teeth. The condition is a form of periodontal disease; however, it is the least devastating, in that it does not involve irreversible damage or changes to the periodontium (gingiva, periodontal ligament, cementum or alveolar bone). It is commonly detected by patients when gingival bleeding occurs spontaneously during brushing or eating. It is also characterised by generalised inflammation, swelling, and redness of the mucosal tissues. Gingivitis is typically painless and is most commonly a result of plaque biofilm accumulation, in association with reduced or poor oral hygiene. Other factors may increase a person's risk of gingivitis, including but not limited to systemic conditions such as uncontrolled diabetes mellitus and some medications. The signs and symptoms of gingivitis can be reversed through improved oral hygiene measures and increased plaque disruption. If left untreated, gingivitis has the potential to progress to periodontitis and other related diseases that are more detrimental to periodontal and general health.[9]
Periodontal diseases
Periodontal disease encompasses a number of diseases of the periodontal tissues that result in attachment loss and destruction of alveolar bone.[10]
Periodontal diseases take on many different forms but are usually a result of a coalescence of bacterial plaque biofilm accumulation of the red complex bacteria (e.g., P. gingivalis, T. forsythia, and T. denticola) of the gingiva and teeth, combined with host immuno-inflammatory mechanisms and other risk factors that can lead to destruction of the supporting bone around natural teeth. Untreated, these diseases can lead to alveolar bone loss and tooth loss. As of 2013, periodontal disease accounted for 70.8% of teeth lost in patients with the disease in South Korea.[11] Periodontal disease is the second most common cause of tooth loss (second to dental caries) in Scotland.[12] Twice-daily brushing and flossing are a way to help prevent periodontal diseases.[13]
Healthy gingiva can be described as stippled, pale or coral pink in Caucasian people, with various degrees of pigmentation in other races. The gingival margin is located at the cemento-enamel junction without the presence of pathology. The gingival pocket between the tooth and the gingival should be no deeper than 1–3mm to be considered healthy. There is also the absence of bleeding on gentle probing.[10]

Periodontal diseases can be caused by a variety of factors, the most prominent being dental plaque. Dental plaque forms a bacterial biofilm on the tooth surface; if not adequately removed from the tooth surface in close proximity to the gingiva, a host-microbial interaction gets underway. This results in the imbalance between host and bacterial factors which can in turn result in a change from health to disease. Other local and/or systemic factors can result in or further progress the manifestation of periodontal disease. Other factors can include age, socio-economic status, oral hygiene education and diet. Systemic factors may include uncontrolled diabetes or tobacco smoking.[14]
Signs and symptoms of periodontal disease: bleeding gums, gingival recession, halitosis (bad breath), mobile teeth, ill-fitting dentures and build up of plaque and calculus.[15]
Individual risk factors include: gender, smoking and alcohol consumption, diabetes, obesity and metabolic syndrome, osteoporosis and Vitamin D conditions, stress and genetic factors.[16]
In 1999 the American Academy of Periodontology (AAP) reworked the existing classification of periodontal diseases from 1989 to alter the weaknesses present. The old classification placed too much emphasis on the age of disease onset and rate of progression, which are often difficult to determine. The 1999 classification was published in the Annals of Periodontology. Below is the abbreviated version of the 1999 classification of periodontal diseases and conditions.[16]
I. Gingival Diseases
A. Dental plaque-induced gingival diseases
B. Non-plaque-induced gingival lesions

II. Chronic Periodontitis
(slight: 1–2 mm CAL; moderate: 3–4 mm CAL;
severe: > 5 mm CAL)
A. Localised
B. Generalised (> 30% of sites are involved)
III. Aggressive Periodontitis
(slight: 1–2 mm CAL; moderate: 3–4 mm CAL;
severe: > 5 mm CAL)
A. Localised
B. Generalised (> 30% of sites are involved)

IV. Periodontitis as a Manifestation of Systemic Diseases
A. Associated with haematological disorders
B. Associated with genetic disorders
C. Not otherwise specified

V. Necrotizing Periodontal Diseases
A. Necrotizing ulcerative gingivitis
B. Necrotizing ulcerative periodontitis
VI. Abscesses of the Periodontium
A. Gingival abscess
B. Periodontal abscess
C. Pericoronal abscess
VII. Periodontitis Associated With Endodontic Lesions
A. Combined periodontic-endodontic lesions

VIII. Developmental or Acquired Deformities and Conditions
A. Localised tooth-related factors that modify or predispose
to plaque-induced gingival diseases/periodontitis
B. Mucogingival deformities and conditions around teeth
C. Mucogingival deformities and conditions on edentulous
ridges
D. Occlusal trauma
In 2018 a new classification of periodontal disease was announced. It was determined that the previous AAP 1999 classification did not cater for the needs of patients with peri-implant diseases and conditions. The new 2018 classification of periodontal and peri-implant diseases and conditions is as follows:[17]
Periodontal Health, Gingival Diseases and Conditions:
Periodontal Health and Gingival Health
Gingivitis: Dental-Biofilm Induced
Gingival Diseases: Non-Dental Biofilm-Induced
Periodontitis:
Necrotizing Periodontal Diseases
Periodontitis
Periodontitis as a Manifestation of Systemic Disease
Other Conditions Affecting The Periodontium:
Systemic Diseases or conditions affecting the periodontal supporting tissues
Periodontal Abscesses and Endodontic-Periodontal Lesions
Mucogingival Deformities and Conditions
Traumatic Occlusal Forces
Tooth and Prosthesis Related Factors
Peri-Implant Diseases and Conditions:
Peri-Implant Health
Peri-Implant Mucositis
Peri-implantitis
Peri-Implant Soft and Hard Tissue Deficiencies
Prevention:
The most effective prevention method is what can be achieved by the patient at home, for example, using the correct tooth brushing technique, interdental cleaning aids such as interdental brushes or floss and using a fluoridated toothpaste. It is also advised that patients receive bi-annual check ups from their dental health provider along with thorough cleaning.
[15]
Treatment:
Along with specialist periodontist treatment, a general dentist or oral health therapist/dental hygienist can perform routine scale and cleans using either hand instruments or an ultrasonic scaler (or a combination of both). The practitioner can also prescribe specialised plaque-removal techniques (tooth brushing, interdental cleaning). The practitioner can also perform a plaque index to indicate to the patient areas of plaque they are not removing on their own. This can be removed through the procedure of a dental prophylaxis.[15]
Aetiology
The primary aetiological factor for periodontal disease is plaque biofilm of dental biofilm. A dental biofilm is a community of microorganisms attached to a hard, non-shedding surface. In the oral cavity, hard non-shedding surfaces include teeth, dental restorative materials and fixed or removable dental appliance such dentures.[14] It is this adherence to non-shedding surfaces that allows bacteria in a dental biofilm to have unique characteristics of clinical significance. The stages of biofilm formation:
- Formation of an acquired pellicle: involves selective absorption of salivary and GCF molecules through an electrostatic affinity with hydroxyapatite.[18]
- Bacterial transportation: bacteria will readily adhere to the acquired pellicle through adhesins, proteins and enzymes within one to two hours.[18]
- Reversible interaction: there is electrostatic attraction or hydrophobic interaction between microorganisms and the tooth surface.[18]
- Irreversible interaction: bacterial adhesins recognise specific host receptors such as pili and outer membrane proteins. The different species of bacteria bind together and require specific receptors to interact with the pellicle.[19]
- Co-adehsion: there is a natural affinity for oral microorganisms to adhere to one another which is termed co‐adhesion. Co-adhesion involves the adherence of planktonic or single culture cells to already attached organisms on a surface. The organisms which make first contact with the surface and allow the platform for later co-adhesion of bacteria are called early colonisers; they facilitate the formation of complex multispecies dental biofilms.[18]
- Multiplication: through continued growth and maturation of existing plaque micro-organisms and the further recruitment of later colonisers.[18]
- Climax community (homeostasis): after a prolonged period of stability, the bacterial community has sufficient nutrients and protection to survive. These complex biofilms are usually found in hard to cleanse areas. Nutrition is provided from dietary consumption of the host for supra-gingival biofilm organisms and from blood and GCF for the sub gingival biofilm organisms.[18]
- Detachment: from one surface to another or within biofilm allows colonisation at remote sites.[20]
Bacteria contained within the biofilm are protected by a slimy extracellular polysaccharide matrix which helps to protect them from the outside environment and chemotherapeutics agents. An example of a chemotherapeutic agent is an antiseptic such as chlorhexidine mouth-rinse or antibiotics. Thus, antibiotics are not generally used in the treatment of periodontal disease, unlike other bacterial infections around the body. The most effective way to control the plaque biofilm is via mechanical removal such as toothbrushing, interdental cleaning or periodontal debridement performed by a dental professional.[20]
Pathogenesis
An individual's host response plays an important role in the pathogenesis of periodontal disease. Even in a mouth where the gingiva appear healthy, there is constant low-level inflammatory response facilitated by the host to manage the constant bacterial load of plaque micro-organisms. Leukocytes and neutrophils are the main cells that phagocytose bacteria found in the gingival crevice or pocket. They migrate from the tissues in a specialised exudate called gingival crevicular fluid also known as GCF. Neutrophils are recruited to the gingival crevice area as they are signalled to by molecules released by plaque microorganisms. Damage to epithelial cells releases cytokines which attract leukocytes to assist with the inflammatory response. The balance between normal cell responses and the beginning of gingival disease is when there is too much plaque bacteria for the neutrophils to phagocytose and they degranulate, releasing toxic enzymes that cause tissue damage. This appears in the mouth as red, swollen and inflamed gingiva which may bleed when probed clinically or during tooth brushing. These changes are due to increased capillary permeability and an influx of inflammatory cells into the gingival tissues. When gingival disease remains established and the aetiology is not removed, there is further recruitment of cells such as macrophages, which assist with the phagocytic digestion of bacteria, and lymphocytes, which begin to initiate an immune response.[21] Pro-inflammatory cytokines are produced inside the gingival tissues and further escalate inflammation, which impacts the progression of chronic systemic inflammation and disease. The result is collagen breakdown, infiltrate accumulation as well as collagen breakdown in the periodontal ligament and alveolar bone resorption. At this stage, the disease has progressed from gingivitis to periodontitis and the loss of supporting periodontium structure is irreversible.[20]
Risk factors
A risk factor is a variable that in health can be defined as "a characteristic associated with an increased rate of a subsequently occurring disease".[22] Risk factors are variables that contribute to disease, rather than being factors that induce disease. Risk factors may be seen as modifiable and non-modifiable. Modifiable risk factors are often behavioural in nature and can be changed by the individual or environmental circumstances, whereas non-modifiable factors are usually intrinsic to an individual's genetics and cannot be changed. To determine risk factors for a disease, evidence-based research and studies are needed for evidence, with longitudinal studies giving the most statistically significant outcomes and the best reliability for determining risk factors. Risk factors often coexist with other variables, rarely acting alone to contribute to a disease. Risk factors can be genetic, environmental, behavioural, psychological, and demographic in nature.[23]
There are many risk factors that contribute to placing an individual at higher risk for developing gingival and periodontal diseases. However, the only aetiological factor for periodontal disease is bacterial plaque, or biofilm. Identification of one's risk factors plays an important role in the diagnosis, treatment and management of periodontal diseases. It was previously believed that each human being had the same risk of developing periodontal diseases, but through the identification and classification of risk factors, it has become well understood that each individual will have a differing array of risk factors that generate susceptibility and contribute to severity of periodontal disease.
Individual, modifiable risk factors include:
- Tobacco smoking: tobacco smoking is firmly established as a major risk factor for periodontal disease, with the relationship between smoking exposure and periodontal tissue destruction being supported strongly by various research papers.[24] Smoking decreases the healing abilities of the oral tissues by destroying blood vessels and supply and preventing essential immune-defence organisms from penetrating the tissues. Therefore, pathogenic bacteria are able to destruct the periodontal tissues more rapidly and escalate the severity of disease.[25] Although the clinical signs of inflammation are less pronounced, smokers have a larger portion of sites with deep pocketing depths and loss of clinical attachment when compared with nonsmokers.[26] Smoking cessation and counselling is an integral part of a dental professional's work with periodontal disease patients. Smoking cessation has been proven to prevent progression of periodontal disease and to return the oral microflora to a less pathogenic microbial state.[27]
- Alcohol consumption: more research needs to be conducted in the form of longitudinal studies on the effects of alcohol on the periodontal tissues. However, current studies suggest that alcohol consumption moderately increases one's risk for progression of periodontal disease.[28]
- Diabetes Mellitus: diabetes falls under the category of modifiable risk factors as although it cannot be cured, it can be controlled, which greatly helps periodontal disease control. A clear two-way relationship has been established with blood glucose control directly affecting periodontal disease severity and progression, and vice versa. Periodontal disease patients with diabetes mellitus also have poorer healing abilities than those without diabetes, and hence are at an increased risk for more severe diseases if blood glucose control is poor and when healing abilities are affected by systemic disease.[22]
- Obesity and vitamin D deficiency are both risk factors for periodontal disease that go hand in hand. Obesity is generally associated with a decreased consumption of fruits and vegetables, with an increase in foods high in fat, salt and sugar. Having a poor diet not only contributes to obesity but also results in a lack of essential nutrients, including vitamin C, D, and calcium, which all play important roles in ensuring a healthy immune system and healthy oral tissues and bone.[29]
- Poor oral hygiene: as plaque is the only aetiological factor for periodontal disease,[30] poor oral hygiene is the most prominent risk factor in initiating, progressing and determining severity of disease. Performing brushing and interdental cleaning is perhaps one of the most effective ways at removing dental plaque biofilm and prevention of periodontal diseases.
- Cardiovascular disease: not only does poor oral hygiene have a clear relationship with an increased risk of developing cardiovascular disease, high concentrations of cholesterol and the mechanisms of oral bacteria in the process of atherosclerosis may increase in individuals with chronic periodontitis.[31]
- Stress: various studies have demonstrated that individuals under psychological, ongoing chronic stress are more likely to have clinical attachment loss and decreased levels of alveolar bone due to periodontal destruction.[32] This is due to the increased production of certain immune cells and interleukins, which decrease the defensive mechanisms against pathogenic bacteria, therefore increasing chances of developing periodontal disease.
Non-modifiable risk factors include:
- Genetics and the host response have been shown to play an important role in periodontal disease development in studies on identical twins and isolated indigenous populations.[33] Periodontal disease also may result due to an abnormal or decreased immune response, rather than aggressive properties of bacterial pathogens.[34]
- Osteoporosis: in individuals with osteoporosis, studies have shown that alveolar bone is less dense than in a healthy adult. However, this does not demonstrate a relationship with periodontal pathogens or clinical attachment loss, therefore more research is needed to investigate if osteoporosis is a true risk factor for periodontal disease.[22]
- Drug-induced disorders: many drugs and medications can have an adverse effect on the periodontal tissues, through contributing to various oral conditions such as dry mouth and gingival hyperplasia.[35] It is crucial that dental professionals ensure that poly-pharmacy patients have medical history reviewed at each visit to correctly evaluate the patient's risk and determine appropriate course of action for dental treatment.
- Haematological disorders: important cells and nutrients carried in the blood to the periodontal tissues are crucial for the tissues' defence mechanisms and response to toxins and pathogens, gas exchange and efficient hemostasis. Therefore, red blood cells have a pivotal role in maintaining the health of the periodontium, meaning haematological disorders can have profound detriment to the periodontal tissues and the onset of disease.[36]
- Pregnancy: studies have shown that the oral tissues are affected and altered during pregnancy due to a decreased immune response and increased vascular blood supply and volume systemically. it is important to note that pregnancy does not cause gingival and periodontal diseases but may exacerbate the inflammatory response to a pre-existing disease. It is also important to note that pregnancy does not detract minerals from the oral tissues or teeth as previously thought and heard in old wives' tales. Existing disease often presents during pregnancy due to an altered oral environment, and not merely due to pregnancy causing disease. These effects can be prevented by good oral hygiene through toothbrushing and interdental cleaning.[37]
Risk characteristics must be considered in conjunction with risk factors as variables that may also contribute to increasing or decreasing one's chances of developing periodontal disease. Numerous studies show that age, gender, race, socioeconomic status, education and genetics also have strong relationships on influencing periodontal disease.
Periodontal disease is multifactorial, requiring dental and oral health professionals to have a clear and thorough understanding of the risk factors and their mechanisms in order to implement effective disease management in clinical practice.[23]
Diagnosis
Periodontitis and associated conditions are recognised as a wide range of inflammatory diseases that have unique symptoms and varying consequences. In order to identify disease, classification systems have been used to categorise periodontal and gingival diseases based on their severity, aetiology and treatments.[10] Having a system of classification is necessary to enable dental professionals to give a label to a patient's condition and make a periodontal diagnosis. A diagnosis is reached by firstly undertaking thorough examination of the patient's medical, dental and social histories, to note any predisposing risk factors (see above) or underlying systemic conditions. Then, this is combined with findings from a thorough intra and extra oral examination. Indices such as the periodontal screening record (PSR) and the Community Periodontal Index of Treatment Needs (CPITN) are also used in making a diagnosis and to order or classify the severity of disease.[38]
If disease is identified through this process, then a full periodontal analysis is performed, often by dental hygienists, oral health therapists or specialist periodontists. This involves full mouth periodontal probing and taking measurements of pocket depths, clinical attachment loss and recession. Along with this other relevant parameters such as plaque, bleeding, furcation involvement and mobility are measured to gain an overall understanding of the level of disease. Radiographs may also be performed to assess alveolar bone levels and levels of destruction.[39]
Treatment
Phases of periodontal therapy
Contemporary periodontal treatment is designed based on the trimeric model, and is performed in four phases. These phases are structured to ensure that periodontal therapy is conducted in a logical sequence, consequently improving the prognosis of the patient, in comparison to indecisive treatment plan without a clear goal.
Phase I therapy (initial therapy – disease control phase)
Non-surgical phase
The non-surgical phase is the initial phase in the sequence of procedures required for periodontal treatment.[40] This phase aims to reduce and eliminate any gingival inflammation by removing dental plaque and calculus, restoration of tooth decay and correction of defective restoration, as these all contribute to gingival inflammation, also known as gingivitis.[40] Phase I consists of treatment of emergencies, antimicrobial therapy, diet control, patient education and motivation, correction of iatrogenic factors, deep caries, hopeless teeth, preliminary scaling, temporary splinting, occlusal adjustment, minor orthodontic tooth movement and debridement.[40]
Re-evaluation phase
During this phase, patients are seen 3–6 weeks after initial therapy; it is required to re-evaluate the steps carried out after the phase I therapy.[40] Usually 3–6 week re-evaluation is crucial in severe cases of periodontal disease. The elements which are required to be re-evaluated are the results of initial therapy (phase I therapy), oral hygiene and status, bleeding and plaque scores and a review of diagnosis and prognosis and modification of the whole treatment plan if necessary.[41]
Phase II therapy (surgical phase)
After post-phase I, it is necessary to evaluate the requirement of periodontium for surgery.[41] Factors identifying if the surgical phase is required are: periodontal pocket management in specific situations, irregular bony contours or deep craters, areas of suspected incomplete removal of local deposits, degree II and III furcation involvements, distal areas of last molars with expected mucogingival junction problems, persistent inflammation, root coverage and removal of gingival enlargement.
Phase III therapy (restorative phase)
During this phase, any defects need to be restored with removable or fixed through dental prosthesis, prosthodontics, or other restoration processes.[40]
Phase IV therapy (maintenance phase)
The last phase of periodontal therapy requires the preservation of periodontal health. In this phase, patients are required to re-visit through a scheduled plan for maintenance care to prevent any re-occurrence of the disease.[41] The maintenance phase constitutes the long-term success for periodontal treatment, thus contributing to a long relationship between the oral health therapist/dentist/periodontist and the patient.[41]
Periodontal and restorative interface
The prognosis of the restorative treatment is determined by the periodontal health. The goals for establishing periodontal health prior to restorative treatment are as follows:
- Periodontal treatment should be managed to assure the establishment of firm gingival margin prior to tooth preparation for restoration. Absence of bleeding tissue during restorative manipulation provides accessibility and aesthetic outcome.[41]
- Certain periodontal treatment is formulated to increase sufficient tooth length for retention. Failure to accomplish these methods prior restorations can lead to the complexity or risk of failure of treatment such as impression making, tooth preparation and restoration.
- Periodontal therapy should follow restorative method as the resolution of gingival inflammation may result in the repositioning of teeth or in soft tissue and mucosal changes.[41]
Standard of periodontal treatment
Non-surgical therapy is the golden standard of periodontal therapy which consists of debridement with a combination of oral hygiene instructions and patient motivation. It mainly focuses on the elimination and reduction of putative pathogens and shifting the microbial flora to a favourable environment to stabilise periodontal disease.[42] Debridement is thorough mechanical removal of calculus and dental biofilm from the root surfaces of the tooth.[43] Debridement is the basis of treatment for inflammatory periodontal diseases and remains the golden standard for surgical and non-surgical treatment in the initial therapy. It is conducted by hand instrumentation such as curettes or scalers and ultrasonic instrumentation.[44] It requires a few appointments, depending on time and clinician skills, for effective removal of supragingival and subgingival calculus, when periodontal pockets are involved. It can assist in periodontal healing and reduce periodontal pocketing by changing the subgingival ecological environment.[44] Prevention of periodontal disease and maintenance of the periodontal tissues following initial treatment requires the patient's ability to perform and maintain effective dental plaque removal.[44] This requires the patient to be motivated in improving their oral hygiene and requires behaviour change in terms of tooth brushing, interdental cleaning, and other oral hygiene techniques.[45] Personal oral hygiene is often considered an essential aspect of controlling chronic periodontitis. Research has shown that it is important to appreciate the motivation of the patient behaviour changes that have originated from the patient.[45] Patients must want to improve their oral hygiene and feel confident that they have the skills to do so. It is crucial for the clinician to encourage patient changes and to educate the patient appropriately. Motivational interviewing is a good technique to ask open-ended questions and express empathy towards the patient.
Role of the oral health therapist
An oral health therapist is a member of the dental team who is dual-qualified as a dental hygienist and dental therapist. They work closely with dentists and a number of dental specialists including Periodontists. It is common for the oral health therapist to be involved in the treatment of gingival and periodontal diseases for patients. Their scope of practice in this area includes oral health assessment, diagnosis, treatment and maintenance and referral where necessary. They also have expertise in providing oral health education and promotion to support the patient to maintain their at-home oral care.[46] Oral health therapists are employed by the dental team to share the responsibilities of care. They are an important asset as they have been uniquely and specifically trained in preventative dentistry and risk minimisation. This allows the dental team to work more competently and effectively as dentists can manage more complex treatments or significantly medically compromised patients.[47]
Periodontist
A periodontist is a specialist dentist who treats patients for periodontal-related diseases and conditions. They are involved in the prevention, diagnosis and treatment of periodontal disease. Periodontists receive further specialist training in periodontics after completing a dental degree. Periodontists provide treatments for patients with severe gingival diseases and/or complex medical histories. Periodontists offer a wide range of treatments including root scaling and planing, periodontal surgery, implant surgery and other complex periodontal procedures.[48]
List of procedures performed by a periodontist:[48]
- non-surgical treatments
- gum graft surgery
- laser treatment
- regenerative procedures
- dental crown lengthening
- dental implants
- pocket reduction procedures
- plastic surgery procedures
Patients are able to access treatment from a specialist periodontist with an appropriate referral from a dental practitioner. The dental hygienist, oral health therapist or dentist will decide whether or not the patient requires further treatment from a periodontist. The practitioner will then fill out a referral form outlining both patient and practitioner concerns, needs and wants.
Training
Before applying to any postgraduate training program in periodontology, one must first complete a dental degree.
Europe
Although each European country has its own independent system, an umbrella organisation—the European Federation of Periodontology (EFP)—has the ability to accredit post-graduate programs according to specific guidelines. The EFP awards a certificate of specialized training in periodontology, periodontics and implant dentistry to every successful European candidate after three years of full-time training in an accredited post-graduate program. The EFP organizes bi-annual meetings around Europe under the title EuroPerio, where many thousands of dentists attend the sessions featuring over one hundred of the world's top periodontal speakers.[49][50] The graduate programs that have been approved are the following: Academic Centre for Dentistry Amsterdam, University of Bern, Sahlgrenska University Hospital, Institute for Postgraduate Dental Education Jönköping, UCL Eastman Dental Institute, University of Louvain (UCLouvain), University Complutense in Madrid, University of Dublin, Trinity College, University of Strasbourg in France, Paris Diderot University at Rothschild hospital.
Australia
Australian programs are accredited by the Australian Dental Council (ADC) and are three years in length and culminate with either a master's degree (MDS) or a Doctor of Clinical Dentistry degree (DClinDent). Fellowship can then be obtained with the Royal Australasian College of Dental Surgeons, FRACDS (Perio).
Canada
Canadian programs are accredited by the Commission on Dental Accreditation of Canada[51] and are a minimum of three years in length and usually culminate with a master (MSc or MDent) degree. Graduates are then eligible to sit for the fellowship exams with the Royal College of Dentists of Canada. Dentistry is a regulated profession. To become a licensed dentist in Canada one must have a BDS, DDS, or DMD degree and be certified by the National Dental Examining Board of Canada.[52] To further specialise into periodontics, accredited dentists are required to undertake a specialty core knowledge examination and complete a postgraduate degree.
India
Periodontics is offered as a specialization field of dentistry in India. Periodontists attend a Master of Dental Surgery (M.D.S.) program affiliated with dental schools in India. The minimum qualification required for the M.D.S. degree is a Bachelor of Dental Surgery. A majority of dental schools in India offer M.D.S. degrees specializing in periodontology. The course is three years and students are trained for implantology as well as diagnosis and treatment of peri-implant diseases along with periodontology.
United Kingdom
The British Society of Periodontology exists to promote the art and science of periodontology. Their membership includes specialist practitioners, periodontists, general dentists, consultants and trainees in restorative dentistry, clinical academics, dental hygienists and therapists, specialist trainees in periodontology and many others.
Specialist training in periodontics in the UK is either a three-year full-time program or four years at three days per week. At the end of the training, candidates are awarded a Master of Clinical Dentistry (MClinDent) before being entered on the specialist list held by the General Dental Council.
United States

The American Dental Association (ADA)-accredited programs are a minimum of three years in length. According to the American Academy of Periodontology, U.S.-trained periodontists are specialists in the prevention, diagnosis and treatment of periodontal diseases and oral inflammation, and in the placement and maintenance of dental implants.[53] Many periodontists also diagnose and treat oral pathology. Historically, periodontics served as the basis for the specialty of oral medicine. Following successful completion of post-graduate training a periodontist becomes board-eligible for the American Board of Periodontology examination. Successful completion of board certification results in Diplomate status in the American Board of Periodontology.
Maintenance
After periodontal treatment, whether it be surgical or non-surgical, maintenance periodontal therapy is essential for a long-term result and stabilization of periodontal disease. There is also a difference in the maintenance of different types of periodontal disease, as there are different types, such as:[54]
Gingivitis
The reversible inflammation of the gums is easily prevented by patients. After the removal of the inflammatory product, usually plaque or calculus, this allows the gums room to heal. This is done by patients thoroughly cleaning teeth every day with a soft bristle toothbrush and an interdental aid. This can be floss, interdental brushes, or whatever is preferred by the patient. Without patient compliance and constant removal of plaque and calculus, gingivitis cannot be treated completely and can progress to irreversible periodontitis.[55]
Necrotising ulcerative gingivitis (NUG)
Also acute necrotising ulcerative gingivitis and necrotising ulcerative periodontitis, it is a type of periodontal disease different than many other periodontal diseases. Clinical characteristics include gingival necrosis (breakdown of the gums), gingival pain, bleeding, halitosis (bad breath), as well as a grey colour to the gingiva and a punched out appearance. It is treated through debridement, usually under local anaesthetic due to immense pain. To maintain and treat the condition completely, a chlorhexidine mouthwash should be recommended to the patient to use twice daily, oral health instruction should be provided (using a soft bristle toothbrush or electric toothbrush twice a day) and an interdental cleaning aid, such as floss or interdental brushes, which cleans the areas that the toothbrush cannot reach. The patient should also be educated on proper nutrition and diet and healthy fluid intake. Smoking cessation should occur not only to completely eradicate the disease but also for the health of the patient. Pain control can be done through ibuprofen or paracetamol/acetaminophen. In the case of an immunocompromised patient, antibiotics should be prescribed. Assessment of treatment should be done after 24 hours of treatment and continued every 3–6 months until signs and symptoms are resolved and gingival health and function restored.[56]
Chronic periodontitis
The inflammation of the gums and irreversible destruction of the alveolar bone and surrounding structures of the teeth, which is usually slow progressing but can have bursts. Local factors explain presence of disease, such as diet, lack of oral hygiene, plaque accumulation, smoking, etc. It is characterised by pocket formation and recession of the gingiva (shrinkage of the gums). Treatment and maintenance are important in stopping disease progression and to resolve the inflammation. Treatment usually consists of scaling and root planning, surgical therapy, and regenerative surgical therapy. After treatment, patient care and regular maintenance check-ups are important to completely eradicate the disease and present its recurrence. This is done through plaque control and removal: twice daily toothbrushing and daily interdental cleaning; chlorhexidine mouthwash can also be effective. The patient should also present to a dentist for maintenance check-ups at least every three months for an in-office check-up and if necessary, plaque control.[57]
Aggressive periodontitis
Aggressive periodontitis involves inflammation of the gingiva and rapid and severe destruction of the periodontal ligament, alveolar bone and surrounding structures. Unlike chronic periodontitis, it often occurs in patients with good oral health and plaque control and can be genetic. Patients generally appear clinically healthy. It can be localised, which generally has a circumpubertal onset, or generalised, which usually occurs in individuals above the age of 35. Treatment is determined on the severity of the disease and the age of the patient. Supragingival (above gums) and subgingival (under gums) debridement and antibiotics are sometimes necessary. To maintain the treatment and prevent reoccurrence of disease, patient care is necessary. This involves good oral hygiene like for all other forms of periodontitis and gingivitis. Brushing twice a day and interdental cleaning are necessary in maintaining a healthy periodontium and preventing the continuation of periodontal destruction. Regular periodontal check ups are also necessary every 3–6 months.
Periodontitis as a manifestation of systemic disease
Periodontitis may be caused by systemic disease. There are currently at least 16 systemic diseases that have been linked with periodontal disease, such as diabetes mellitus, haematological disorders such as acquired neutropenia and leukemia, Down syndrome, etc. Treatment and prevention are very important concepts in the management and maintenance of periodontitis as a manifestation of systemic disease. Treatment can consist of either surgical or non-surgical treatment depending on severity. After treatment, patient compliance is important, which includes oral hygiene: tooth brushing twice a day and interdental brushing at least once a day; chlorohexidine mouthwash may also be helpful.
See also
- Bone grafting
- Chronic periodontitis
- Dental implant
- Gingival graft
- Gingival recession
- Journal of Periodontology
- Periodontitis
- Scaling and root planing
- Sinus lift
References
- ↑ "What is a Periodontist?". Perio.org. Retrieved 2019-10-21.
- ↑ "Anatomy of the Periodontium | An Overview of Dental Anatomy | CE Course | dentalcare.com". www.dentalcare.com. Retrieved 2019-10-21.
- 1 2 Clerehugh, V., Tugnait, A., & Genco, R. J. (2009). Periodontology at a glance. Chichester: John Wiley & Sons Ltd
- 1 2 3 4 5 Cope, Graham; Cope, Anwen (1 July 2011). "The periodontium: an anatomical guide". Dental Nursing. 7 (7): 376–378. doi:10.12968/denn.2011.7.7.376.
- 1 2 Newman, M., Takei, H. Klokkevold, P. R., Carranza, F. A. (2015). Carranza’s Clinical Periodontology (12th ed.). St. Louis: Elsevier Inc
- 1 2 3 4 Weinberg, M., Westphal, C., Froum, S. J., Palat, M. P., & Schoor, R. S. (2010). Comprehensive Periodontics for the Dental Hygienist (3rd ed.). Upper Saddle River, N.J.: Pearson Education
- 1 2 3 4 5 Gehrig, J., & Willmann, D. E. (2011). Foundations of Periodontics for the Dental Hygienist (3rd ed.). Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health.
- ↑ "Search the Glossary - AAP Connect". members.perio.org. Retrieved 2019-10-21.
- ↑ de Vries, Kevin (July 2015). "Primary care: Gingivitis". The Australian Journal of Pharmacy. 96 (1141): 64.
- 1 2 3 Highfield, J (September 2009). "Diagnosis and classification of periodontal disease". Australian Dental Journal. 54: S11–S26. doi:10.1111/j.1834-7819.2009.01140.x. PMID 19737262.
- ↑ Lee, Jae-Hong; Oh, Jin-Young; Choi, Jung-Kyu; Kim, Yeon-Tae; Park, Ye-Sol; Jeong, Seong-Nyum; Choi, Seong-Ho (October 2017). "Trends in the incidence of tooth extraction due to periodontal disease: results of a 12-year longitudinal cohort study in South Korea". Journal of Periodontal & Implant Science. 47 (5): 264–272. doi:10.5051/jpis.2017.47.5.264. PMC 5663665. PMID 29093985.
- ↑ McCaul, L. K.; Jenkins, W. M. M.; Kay, E. J. (June 2001). "The reasons for extraction of permanent teeth in Scotland: a 15-year follow-up study". British Dental Journal. 190 (12): 658–662. doi:10.1038/sj.bdj.4801068. PMID 11453155.
- ↑ "Periodontology: an overview". Retrieved 17 September 2018.
- 1 2 Hasan, A.; Palmer, R. M. (25 April 2014). "A clinical guide to periodontology: Pathology of periodontal disease". British Dental Journal. 216 (8): 457–461. doi:10.1038/sj.bdj.2014.299. PMID 24762896.
- 1 2 3 "Gum Disease: Causes, Prevention, & Treatment of Gum Disease". Colgate® Australia.
- 1 2 Genco, Robert J.; Borgnakke, Wenche S. (June 2013). "Risk factors for periodontal disease". Periodontology 2000. 62 (1): 59–94. doi:10.1111/j.1600-0757.2012.00457.x. PMID 23574464.
- ↑ Caton, Jack G.; Armitage, Gary; Berglundh, Tord; Chapple, Iain L.C.; Jepsen, Søren; Kornman, Kenneth S.; Mealey, Brian L.; Papapanou, Panos N.; Sanz, Mariano; Tonetti, Maurizio S. (June 2018). "A new classification scheme for periodontal and peri-implant diseases and conditions - Introduction and key changes from the 1999 classification" (PDF). Journal of Periodontology. 89: S1–S8. doi:10.1002/JPER.18-0157. PMID 29926946.
- 1 2 3 4 5 6 Marsh, P. D.; Zaura, Egija (March 2017). "Dental biofilm: ecological interactions in health and disease". Journal of Clinical Periodontology. 44: S12–S22. doi:10.1111/jcpe.12679. PMID 28266111.
- ↑ O'Toole, George; Kaplan, Heidi B.; Kolter, Roberto (October 2000). "Biofilm Formation as Microbial Development". Annual Review of Microbiology. 54 (1): 49–79. doi:10.1146/annurev.micro.54.1.49. PMID 11018124.
- 1 2 3 Gurenlian, JoAnn R. (31 December 2007). "The Role of Dental Plaque Biofilm in Oral Health". American Dental Hygienists' Association. 81 (suppl 1): 116.
- ↑ Kinane, Denis F. (February 2001). "Causation and pathogenesis of periodontal disease". Periodontology 2000. 25 (1): 8–20. doi:10.1034/j.1600-0757.2001.22250102.x. PMID 11155179./
- 1 2 3 Van Dyke, Thomas E.; Dave, Sheilesh (2005). "Risk Factors for Periodontitis". Journal of the International Academy of Periodontology. 7 (1): 3–7. PMC 1351013. PMID 15736889.
- 1 2 AlJehani, Yousef A. (2014). "Risk Factors of Periodontal Disease: Review of the Literature". International Journal of Dentistry. 2014: 182513. doi:10.1155/2014/182513. PMC 4055151. PMID 24963294.
- ↑ Chahal, GurparkashSingh; Chhina, Kamalpreet; Chhabra, Vipin; Chahal, Amna (2017). "Smoking and its effect on periodontium – Revisited". Indian Journal of Dental Sciences. 9 (1): 44. doi:10.4103/ijds.ijds_96_16.
- ↑ Rivera-Hidalgo, Francisco (October 1986). "Smoking and Periodontal Disease: A Review of the Literature". Journal of Periodontology. 57 (10): 617–624. doi:10.1902/jop.1986.57.10.617. PMID 3534210.
- ↑ Grossi, Sara G.; Zambon, Joseph J.; Ho, Alex W.; Koch, Gary; Dunford, Robert G.; Machtei, Eli E.; Norderyd, Ola M.; Genco, Robert J. (March 1994). "Assessment of Risk for Periodontal Disease. I. Risk Indicators for Attachment Loss". Journal of Periodontology. 65 (3): 260–267. doi:10.1902/jop.1994.65.3.260. PMID 8164120.
- ↑ Grossi, SG; Zambon, J; Machtei, EE; Schifferle, R; Andreana, S; Genco, RJ; Cummins, D; Harrap, G (May 1997). "Effects of smoking and smoking cessation on healing after mechanical periodontal therapy". Journal of the American Dental Association. 128 (5): 599–607. doi:10.14219/jada.archive.1997.0259. PMID 9150643.
- ↑ Tezal, Miné; Grossi, Sara G.; Ho, Alex W.; Genco, Robert J. (February 2001). "The Effect of Alcohol Consumption on Periodontal Disease". Journal of Periodontology. 72 (2): 183–189. doi:10.1902/jop.2001.72.2.183. PMID 11288791.
- ↑ Neiva, Rodrigo F.; Steigenga, Jennifer; Al-Shammari, Khalaf F.; Wang, Hom-Lay (July 2003). "Effects of specific nutrients on periodontal disease onset, progression and treatment". Journal of Clinical Periodontology. 30 (7): 579–589. doi:10.1034/j.1600-051x.2003.00354.x. PMID 12834494.
- ↑ Brogden, K., & Guthmiller, J. (2002). Polymicrobial diseases (p. Chapert 8 – Periodontal diseases). [Washington, D.C.]: ASM Press.
- ↑ Izumi, Aki; Yoshihara, Akihiro; Hirotomi, Toshinobu; Miyazaki, Hideo (May 2009). "The Relationship Between Serum Lipids and Periodontitis in Elderly Non-Smokers". Journal of Periodontology. 80 (5): 740–748. doi:10.1902/jop.2009.080584. PMID 19405827.
- ↑ Hugoson, A.; Ljungquist, B.; Breivik, T. (March 2002). "The relationship of some negative events and psychological factors to periodontal disease in an adult Swedish population 50 to 80 years of age". Journal of Clinical Periodontology. 29 (3): 247–253. doi:10.1034/j.1600-051x.2002.290311.x. PMID 11940145.
- ↑ Michalowicz, Bryan S.; Diehl, Scott R.; Gunsolley, John C.; Sparks, Brandon S.; Brooks, Carol N.; Koertge, Thomas E.; Califano, Joseph V.; Burmeister, John A.; Schenkein, Harvey A. (November 2000). "Evidence of a Substantial Genetic Basis for Risk of Adult Periodontitis". Journal of Periodontology. 71 (11): 1699–1707. doi:10.1902/jop.2000.71.11.1699. PMID 11128917.
- ↑ Van Dyke, T. E.; Serhan, C.N. (13 December 2016). "Resolution of Inflammation: A New Paradigm for the Pathogenesis of Periodontal Diseases". Journal of Dental Research. 82 (2): 82–90. doi:10.1177/154405910308200202. PMID 12562878.
- ↑ Taylor, Barbara Anne (1 February 2003). "Management of drug-induced gingival enlargement". Australian Prescriber. 26 (1): 11–3. doi:10.18773/austprescr.2003.007. PMID 11709926.
- ↑ Kinane, DF; Marshall, GJ (March 2001). "Peridonatal manifestations of systemic disease". Australian Dental Journal. 46 (1): 2–12. doi:10.1111/j.1834-7819.2001.tb00267.x. PMID 11355236.
- ↑ Laine, Merja Anneli (2 July 2009). "Effect of pregnancy on periodontal and dental health". Acta Odontologica Scandinavica. 60 (5): 257–264. doi:10.1080/00016350260248210. PMID 12418714.
- ↑ Armitage, Gary C. (February 2004). "Periodontal diagnoses and classification of periodontal diseases". Periodontology 2000. 34 (1): 9–21. doi:10.1046/j.0906-6713.2002.003421.x. PMID 14717852.
- ↑ Preshaw, Philip M (15 September 2015). "Detection and diagnosis of periodontal conditions amenable to prevention". BMC Oral Health. 15 (S1): S5. doi:10.1186/1472-6831-15-s1-s5. PMC 4580822. PMID 26390822.
- 1 2 3 4 5 Duarte, Poliana Mendes; da Rocha, Marcelo; Sampaio, Eduardo; Mestnik, Maria Josefa; Feres, Magda; Figueiredo, Luciene Cristina; Bastos, Marta Ferreira; Faveri, Marcelo (July 2010). "Serum Levels of Cytokines in Subjects With Generalized Chronic and Aggressive Periodontitis Before and After Non-Surgical Periodontal Therapy: A Pilot Study". Journal of Periodontology. 81 (7): 1056–1063. doi:10.1902/jop.2010.090732. PMID 20192617.
- 1 2 3 4 5 6 Mohd-Dom, Tuti; Ayob, Rasidah; Mohd-Nur, Amrizal; Abdul-Manaf, Mohd R; Ishak, Noorlin; Abdul-Muttalib, Khairiyah; Aljunid, Syed M; Ahmad-Yaziz, Yuhaniz; Abdul-Aziz, Hanizah; Kasan, Noordin; Mohd-Asari, Ahmad S (20 May 2014). "Cost analysis of Periodontitis management in public sector specialist dental clinics". BMC Oral Health. 14 (1): 56. doi:10.1186/1472-6831-14-56. PMC 4033493. PMID 24884465.
- ↑ Mordohai, N.; Reshad, M.; Jivraj, S.; Chee, W. (27 January 2007). "Factors that affect individual tooth prognosis and choices in contemporary treatment planning". British Dental Journal. 202 (2): 63–72. doi:10.1038/bdj.2007.23. PMID 17255985.
- ↑ Oshman, Sarah; El Chaar, Edgard; Lee, Yoonjung Nicole; Engebretson, Steven (25 July 2016). "Effect of patient age awareness on diagnostic agreement of chronic or aggressive periodontitis between clinicians; a pilot study". BMC Oral Health. 17 (1): 27. doi:10.1186/s12903-016-0258-0. PMC 4960759. PMID 27456238.
- 1 2 3 Allen, E; Ziada, H; Irwin, CR; Mullally, B; Byrne, PJ (2 April 2008). "Periodontics: 10. Maintenance in Periodontal Therapy". Dental Update. 35 (3): 150–156. doi:10.12968/denu.2008.35.3.150. PMID 18507223.
- 1 2 Martinez-Canut, Pedro; Llobell, Andrés; Romero, Antonio (June 2017). "Predictors of long-term outcomes in patients undergoing periodontal maintenance". Journal of Clinical Periodontology. 44 (6): 620–631. doi:10.1111/jcpe.12730. PMC 5519943. PMID 28419497.
- ↑ "Guidelines for scope of practice". Dental Board of Australia. Retrieved 8 May 2019.
- ↑ Nash, David A. (October 2012). "Envisioning an oral healthcare workforce for the future". Community Dentistry and Oral Epidemiology. 40: 141–147. doi:10.1111/j.1600-0528.2012.00734.x. PMID 22998319.
- 1 2 American Academy of Periodontology. (2019). What is a periodontist?. Retrieved from https://www.perio.org/consumer/what-is-a-periodontist
- ↑ "EuroPerio Congress – EFP". efp.org. 2019-12-23.
- ↑ PERIO PEOPLE. "PerioPeople Home". efp.org.
- ↑ CDAC. (2013). Retrieved from https://www.cda-adc.ca/cdacweb/en/
- ↑ Becoming a licensed dentist in Canada | The National Dental Examining Board of Canada. (2019). Retrieved from https://ndeb-bned.ca/en/requirements
- ↑ "What is a Periodontist?". Perio.org. American Academy of Periodontology. Retrieved 2015-01-26.
- ↑ Hou, Yue; Wang, Xin; Zhang, Cong-Xiao; Wei, Yu-Dan; Jiang, Li-Li; Zhu, Xiao-Yu; Du, Yu-Jun (1 September 2017). "Risk factors of periodontal disease in maintenance hemodialysis patients". Medicine. 96 (35): e7892. doi:10.1097/MD.0000000000007892. PMC 5585499. PMID 28858105.
- ↑ Azaripour, Adriano; Weusmann, Jens; Eschig, Carl; Schmidtmann, Irene; Van Noorden, Cornelis J. F.; Willershausen, Brita (23 May 2016). "Efficacy of an aluminium triformate mouthrinse during the maintenance phase in periodontal patients: a pilot double blind randomized placebo-controlled clinical trial". BMC Oral Health. 16 (1): 57. doi:10.1186/s12903-016-0214-z. PMC 4878033. PMID 27216479.
- ↑ Dufty, J; Gkranias, N; Donos, N (2017). "Necrotising Ulcerative Gingivitis: A Literature Review". Oral Health & Preventive Dentistry. 15 (4): 321–327. doi:10.3290/j.ohpd.a38766. PMID 28761942.
- ↑ Furuta, Michiko; Fukai, Kakuhiro; Aida, Jun; Shimazaki, Yoshihiro; Ando, Yuichi; Miyazaki, Hideo; Kambara, Masaki; Yamashita, Yoshihisa (2019). "Periodontal status and self-reported systemic health of periodontal patients regularly visiting dental clinics in the 8020 Promotion Foundation Study of Japanese Dental Patients". Journal of Oral Science. 61 (2): 238–245. doi:10.2334/josnusd.18-0128. PMID 31217373.
External links
- AAP Directory of Periodontists
- American Academy of Periodontology's (AAP) article on Periodontal Disease
- British Society of Periodontology
- Canadian Academy directory of Periodontists
- Dental Council of India
- European Federation of Periodontology
- The National Institute of Cranialfacial Research's article on Periodontal Disease
- South African Society for Periodontology
| Authority control: National libraries |
|---|