Penile implant
| Penile implant | |
|---|---|
 Penile implant | |
| Other names | Penile prosthesis |
| Specialty | Urology |
| ICD-10-PCS | 0VUS0JZ |
| CPT | 54400, 54405 |
A penile implant is an implanted device intended for the treatment of Erectile dysfunction, Peyronie's disease, ischemic Priapism, deformity and any traumatic injury of the penis, and for phalloplasty in men or phalloplasty and metoidioplasty in female-to-male gender reassignment surgery. Men also opt for penile implants for aesthetic purposes. Men’s satisfaction and sexual function is influenced by discomfort over genital size which leads to seek surgical and non-surgical solutions for penis alteration.[1] Although there are many distinct types of implants, most fall into one of two categories: malleable and inflatable transplants.[2]
Penile size
According to the British Journal of Urology International, a study that synthesizes data from 17 previous academic papers that included measurements from a total of 15,521 men from around the world, the average bone-pressed flaccid penis is 3.6 inches in length and 3.66 inches in girth, whereas the average bone-pressed erect penis is 5.1 inches long and 4.59 inches in girth. A 16-cm (6.3-inch) bone-pressed erect penis falls into the 95th percentile: Out of 100 men, only five would have a penis larger than 16 cm. Conversely, an erect penis measuring 10 cm (3.94 inches) falls into the 5th percentile: Only five out of 100 men would have a penis smaller than 10 cm.[3]
The researchers concluded that there was no strong evidence to link penis size to other physical features such as height, body mass index, or even shoe size.[3][4]
Women's preferences for penis size
Women’s preferences for penis size may affect men’s comfort with their own bodies and may have implications for sexual health. Studies of women’s penis size preferences typically have relied on their abstract ratings or selecting amongst 2D, flaccid images. According to a study that used haptic stimuli to allow assessment of women’s size recall accuracy for the first time, as well as examine their preferences for erect penis sizes in different relationship contexts. Women preferred a penis of slightly larger circumference and length for one-time (length = 6.4 inches/16.3 cm, circumference = 5.0 inches/12.7 cm) versus long-term (length = 6.3 inches/16.0 cm, circumference = 4.8 inches/12.2 cm) sexual partners. These first estimates of erect penis size preferences using 3D models suggest women accurately recall size and prefer penises slightly larger than the 95th percentile.[5]
History
The first modern prosthetic reconstruction of a penis is attributed to NA Borgus, a German physician who performed the first surgical attempts in 1936 on soldiers with traumatic amputations of the penis. He used rib cartilages as prosthetic material and reconstructed the genitals for both micturition and intercourse purposes.[6] Willard E. Goodwin and William Wallace Scott were the first to describe the placement of synthetic penile implants using acrylic prosthesis in 1952.[7] Silicone-based penile implants were developed by Harvey Lash and the first case series were published in 1964.[8] The development of a high-grade silicone that is currently used in penile implants is credited to NASA.[9] The prototypes of the contemporary inflatable and malleable penile implants were presented in 1973 during the annual meeting of the American Urological Association by two groups of physicians from Baylor University (Gerald Timm, William E. Bradley and F. Brantley Scott) and University of Miami (Michael P. Small and Hernan M. Carrion).[6][10][11] Small and Carrion pioneered the popularization of semi-rigid penile implants with the introduction of Small-Carrion prosthesis (Mentor, USA) in 1975. Brantley Scott described the initial device as composed of two inflatable cylindrical bodies made up of silicone, a reservoir containing radiopaque fluid and two pumping units.[10] The first generation products were marketed through American Medical Systems (AMS; currently Boston Scientific), with which Brantley Scott was associated.[9][12] Many device updates have been released by AMS since the first generation implants. In 1983, Mentor (currently Coloplast) joined the market.[9] In 2017, there were more than ten manufacturers of penile implants in the world, however only a few now remain in the market.[13] The latest additions to the market are Zephyr Surgical Implants and Rigicon Innovative Urological Solutions.[14][15] Zephyr Surgical Implants, along with penile implants for biological men, introduced the first line of inflatable and malleable penile implants designed for sex reassignment for trans men.
According to analysis of the 5% Medicare Public Use Files from 2001 to 2010 approximately 3% of patients diagnosed with erectile dysfunction opt for penile implantation.[16] Each year nearly 25,000 inflatable penile prostheses are implanted in the USA.[17]
The list shows penile implants available in the market in 2020.
| Product | Company | Country of origin | Type of the implant | Introduced in |
|---|---|---|---|---|
| AMS Spectra | Boston Scientific (formerly American Medical Systems) | United States of America | Malleable | 2009 |
| Tactra | Boston Scientific (formerly American Medical Systems) | United States of America | Malleable | 2019 |
| Genesis | Coloplast | United States of America | Malleable | 2004 |
| ZSI 100, ZSI 100 FtM and ZSI 100 D4 | Zephyr Surgical Implants | Switzerland | Malleable | 2012 |
| Tube | Promedon | Argentina | Malleable | 2007 |
| AMS Ambicor | Boston Scientific (formerly American Medical Systems) | United States of America | Inflatable | 1994 |
| AMS 700 series (LGX, CX, CXR) | Boston Scientific (formerly American Medical Systems) | United States of America | Inflatable | 1983 |
| Titan | Coloplast | United States of America | Inflatable | 2002 |
| ZSI 475 and ZSI 475 FtM | Zephyr Surgical Implants | Switzerland | Inflatable | 2012 |
| Infla10 series (AX, X, NarrowBody) | Rigicon Innovative Urological Solutions | United States of America | Inflatable | 2019 |
| Rigi10[18] | Rigicon Innovative Urological Solutions | United States of America | Malleable | 2017 |
| Rigi10 Hydrophilic | Rigicon Innovative Urological Solutions | United States of America | Malleable | 2019 |
Types
Malleable penile implant


The malleable (also known as non-inflatable or semi-rigid) penile prosthesis is a set of a pair of rods implanted into the corpora of the penis. The rods are hard, but 'malleable' in the sense that they can be adjusted manually into the erect position.[19] There are two types of malleable implants: one that is made of silicone and does not have a rod inside, also called soft implants, and another with a silver or steel spiral wire core inside coated with silicone. Some of the models have trimmable tails intended for length adjustment.[13] Currently, a variety of malleable penile implants are available worldwide.[20]
Inflatable penile implant
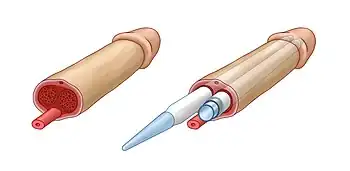
The inflatable penile implant (IPP), more recently developed, is a set of inflatable cylinders and a pump system. Based on the differences in structure, there are two types of inflatable penile implants: two-piece and three-piece IPPs. Both types of inflatable devices are filled with sterile saline solution which is pumped into cylinders when in process. The cylinders are implanted into the cavernous body of the penis. The pump system is attached to the cylinders and placed in the scrotum.[13] Three-piece implants have a separate large reservoir connected to the pump. The reservoir is commonly placed in the retropubic space (Retzius' space), however other locations have also been described, such as between the transverse muscle and rectus muscle. Three-piece implants provide more desirable rigidity and girth of the penis resembling natural erection. Additionally, due to the presence of a large reservoir, three-piece implants provide full flaccidity of the penis when deflated, thus bringing more comfort than two-piece inflatable and malleable implants.[9]
The saline solution is pumped manually from the reservoir into bilateral chambers of cylinders implanted in the shaft of the penis, which replaces the non- or minimally-functioning erectile tissue. This produces an erection. The glans of the penis, however, remains unaffected. Ninety to ninety-five percent of inflatable prostheses produce erections suitable for sexual intercourse. In the United States, the inflatable prosthesis has largely replaced the malleable one, due to its lower rate of infections, high device survival rate and 80-90% satisfaction rate.[2]
The first IPP prototype presented in 1975 by Scott and colleagues was a three-piece prosthesis (two cylinders, two pumps and a fluid reservoir). Since then, the IPP has undergone multiple modifications and improvements for device reliability and durability, including change in the chemical material used in implant manufacturing, using hydrophilic and antibiotic eluting coatings to reduce the rates of infections, introducing one-touch release etc.[13] Surgical techniques used for the implantation of penile prostheses have also improved along with evolution of the device. Inflatable penile implants were one of the first interventions in urology where the "no-touch" surgical technique was introduced. This has significantly reduced the rates of post-operative infections.[21]
Medical use

Erectile dysfunction
In spite of recent rapid and extensive development of non-surgical management options for erectile dysfunction, especially novel targeted medications and gene therapy, the penile implants remain the mainstay and the gold standard choice for the treatment of erectile dysfunction refractory to oral medications and injectable therapy.[22][9] Additionally, penile implants can be a relevant option for those with erectile dysfunction who wants to proceed with a permanent solution without medical therapy. Penile implants have been used for the treatment of erectile dysfunction with various etiologies, including vascular, cavernosal, neurogenic, psychological and post-surgical (e.g. prostatectomy). The American Urological Association recommends informing all men with erectile dysfunction about penile implants as a choice of treatment and discussing the potential outcomes with them.[23]
Penile deformity
Penile implants can help recover the natural shape of the penis in various conditions that have led to penile deformity. These can be traumatic injuries, penile surgeries, disfiguring and fibrosing diseases of the penis, such as Peyronie's disease.[9] In Peyronie's disease, the change in penile curvature affects normal sexual intercourse as well as causing erectile dysfunction due to disruption of blood flow in the cavernous bodies of the penis.[24] Therefore, implantation of penile prosthesis in Peyronie's disease addresses several mechanisms involved in the pathophysiology of the disease.
Female-to-male sex reassignment
Although different models of penile prostheses have been reported to be implanted after phalloplasty procedures,[25] with the first case described in 1978 by Pucket and Montie,[26] the first penile implants designed and produced specifically for female-to-male gender reassignment surgery for trans men were introduced in 2015 by Zephyr Surgical Implants.[27] Both malleable and inflatable models are available. These implants have more realistic shape with an ergonomic glans at the tip of the prosthesis. The inflatable model has an attached pump resembling a testicle. The prosthesis is implanted with a sturdy fixation on pubic bone. Another, thinner malleable implant is intended for metoidioplasty.
Outcomes
Satisfaction
The overall satisfaction rate with penile implants reaches over 90%.[9] Both self and partner-reported satisfaction rates are evaluated to assess the outcomes. It has been shown that implantation of inflatable penile prosthesis brings more patient and partner satisfaction than medication therapy with PDE5 inhibitors or intracavernosal injections.[22] Satisfaction rates are reported to be higher with inflatable rather than malleable implants, but there are no difference between two-piece and three-piece devices.[28][29] The most frequent reasons for dissatisfaction are reduced penis length and girth, failed expectations and difficulties with device use.[22][28] Thus, it is vital to provide patients and their partners with detailed preoperative counselling and instructions.
Curvature correction
33% to 90% of cases of patients with Peyronie's disease that have had an inflatable PI procedure have successfully corrected their penile deformity.[24] The residual curvature after penile implant placement usually requires intraoperative surgical intervention.
Complications
The most common complication associated with penile implant placement appears to be infections with reported rates of 1-3%.[28] Both surgical site and device infections are reported. When the infection involves the penile implant itself, implant removal is required and irrigation of the cavities with antiseptic solutions. In this scenario, placement of a new implant is needed to avoid further tissue fibrosis and shortening of the penis. The rate of repeat surgeries or device replacements ranges from 6% to 13%.[24] Other reported complications include perforation of the corpus cavernosum and urethra (0.1-3%), commonly occurring in patients with previous fibrosis, prosthesis erosion or extrusion, change in glans shape, hematoma, shortening of penis length, and device malfunction. Due to continuous improvement of surgical techniques and modifications of implants, complication rates have dramatically decreased over time.
To overcome post-operative penile shortening and to increase the perceived length of the penis and patient satisfaction, ventral and dorsal phalloplasty procedures in combination with penile implants have been described.[22] Modified glanulopexy has been proposed to prevent supersonic transporter deformity and glandular hypermobility which are possible complications of penile implants.[30] Sliding techniques in which the penis is cut and elongated with penile implants have been performed in cases of severe penile shortening. However, these techniques had higher rates of complications and are currently avoided.
References
- ↑ Littara, Alessandro; Melone, Roberto; Morales-Medina, Julio Cesar; Iannitti, Tommaso; Palmieri, Beniamino (2019-04-19). "Cosmetic penile enhancement surgery: a 3-year single-centre retrospective clinical evaluation of 355 cases". Scientific Reports. 9 (1): 6323. Bibcode:2019NatSR...9.6323L. doi:10.1038/s41598-019-41652-w. ISSN 2045-2322. PMC 6474863. PMID 31004096.
- 1 2 Perito, Paul. "Penile Implants". PeritoUrology.com. Perito Urology. Retrieved 12 November 2019.
- 1 2 Veale, David; Miles, Sarah; Bramley, Sally; Muir, Gordon; Hodsoll, John (2015). "Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15 521 men". BJU International. 115 (6): 978–986. doi:10.1111/bju.13010. ISSN 1464-410X. PMID 25487360. S2CID 36836535.
- ↑ Shah, J.; Christopher, N. (October 2002). "Can shoe size predict penile length?". BJU International. 90 (6): 586–587. doi:10.1046/j.1464-410x.2002.02974.x. ISSN 1464-4096. PMID 12230622. S2CID 20887458.
- ↑ Prause, Nicole; Park, Jaymie; Leung, Shannon; Miller, Geoffrey (2015-09-02). "Women's Preferences for Penis Size: A New Research Method Using Selection among 3D Models". PLOS ONE. 10 (9): e0133079. Bibcode:2015PLoSO..1033079P. doi:10.1371/journal.pone.0133079. ISSN 1932-6203. PMC 4558040. PMID 26332467.
- 1 2 Carrion, Hernan; Martinez, Daniel; Parker, Justin; Hakky, Tariq; Bickell, Michael; Boyle, Alexander; Weigand, Luke; Carrion, Rafael (July 2016). "A History of the Penile Implant to 1974". Sexual Medicine Reviews. 4 (3): 285–293. doi:10.1016/j.sxmr.2016.05.003. PMID 27871961.
- ↑ Goodwin, Willard E.; Scott, William Wallace (December 1952). "Phalloplasty". Journal of Urology. 68 (6): 903–908. doi:10.1016/S0022-5347(17)68301-0. PMID 13000938.
- ↑ Lash, Harvey; Zimmerman, Donald C.; Loeffler, Robert A. (July 1964). "Silicone Implantation". Plastic and Reconstructive Surgery. 34 (1): 75–80. doi:10.1097/00006534-196407000-00011. PMID 14200523. S2CID 43779571.
- 1 2 3 4 5 6 7 Rodriguez, Katherine M.; Pastuszak, Alexander W. (November 2017). "A history of penile implants". Translational Andrology and Urology. 6 (S5): S851–S857. doi:10.21037/tau.2017.04.02. PMC 5715175. PMID 29238664.
- 1 2 Brantley Scott, F.; Bradley, William E.; Timm, Gerald W. (July 1973). "Management of erectile impotence Use of implantable inflatable prosthesis". Urology. 2 (1): 80–82. doi:10.1016/0090-4295(73)90224-0. PMID 4766860.
- ↑ Small, Michael P.; Carrion, Hernan M.; Gordon, Julian A. (April 1975). "Small-Carrion penile prosthesis". Urology. 5 (4): 479–486. doi:10.1016/0090-4295(75)90071-0. PMID 1093303.
- ↑ Carson, Culley C (May 2018). "F. Brantley Scott: a visionary in the world of urology". Trends in Urology & Men's Health. 9 (3): 32–33. doi:10.1002/tre.639.
- 1 2 3 4 Chung, Eric (February 2017). "Penile prosthesis implant: scientific advances and technological innovations over the last four decades". Translational Andrology and Urology. 6 (1): 37–45. doi:10.21037/tau.2016.12.06. PMC 5313299. PMID 28217449.
- ↑ Mulcahy, John J.; Köhler, Tobias S.; Wen, Lexiaochuan; Wilson, Steven K. (7 August 2020). "Penile implant infection prevention part II: device coatings have changed the game". International Journal of Impotence Research. 33 (8): 801–807. doi:10.1038/s41443-020-0338-1. PMC 8776559. PMID 32770140. S2CID 221019610.
- ↑ Trost, Landon (2020). "Future considerations in prosthetic urology". Asian Journal of Andrology. 22 (1): 70–75. doi:10.4103/aja.aja_103_19. PMC 6958985. PMID 31571642.
- ↑ Lee, Daniel J.; Najari, Bobby B.; Davison, Wesley L.; Al Awamlh, Bashir Al Hussein; Zhao, Fujun; Paduch, Darius A.; Mulhall, John P.; Chughtai, Bilal; Lee, Richard K. (July 2015). "Trends in the Utilization of Penile Prostheses in the Treatment of Erectile Dysfunction in the United States". The Journal of Sexual Medicine. 12 (7): 1638–1645. doi:10.1111/jsm.12921. PMID 26096365.
- ↑ Darouiche, Rabih O.; Bella, Anthony J.; Boone, Timothy B.; Brock, Gerry; Broderick, Gregory A.; Burnett, Arthur L.; Carrion, Raphael; Carson, Culley; Christine, Brian; Dhabuwala, Chipriya B.; Hakim, Lawrence S.; Henry, Gerard; Jones, LeRoy A.; Khera, Mohit; Montague, Drogo K.; Nehra, Ajay (October 2013). "North American Consensus Document on Infection of Penile Prostheses". Urology. 82 (4): 937–942. doi:10.1016/j.urology.2013.05.048. PMID 23958508.
- ↑ "Enforcement Reports". www.accessdata.fda.gov.
- ↑ Perito, Paul. "Malleable Penile Implant Prosthesis". PeritoUrology.com. Perito Urology. Retrieved 12 November 2019.
- ↑ Le, Brian; Burnett, Arthur L. (2015). "Evolution of penile prosthetic devices". Korean Journal of Urology. 56 (3): 179–86. doi:10.4111/kju.2015.56.3.179. PMC 4355428. PMID 25763121.
- ↑ Eid, J. Francois (July 2016). "Penile Implant: Review of a "No-Touch" Technique". Sexual Medicine Reviews. 4 (3): 294–300. doi:10.1016/j.sxmr.2016.01.002. PMID 27871962.
- 1 2 3 4 Fakhoury, Mathew Q; Halpern, Joshua; Bennett, Nelson (18 February 2019). "Recent advancements in penile prosthetics". F1000Research. 8: 193. doi:10.12688/f1000research.17407.1. PMC 6381800. PMID 30828431.
- ↑ Burnett, Arthur L.; Nehra, Ajay; Breau, Rodney H.; Culkin, Daniel J.; Faraday, Martha M.; Hakim, Lawrence S.; Heidelbaugh, Joel; Khera, Mohit; McVary, Kevin T.; Miner, Martin M.; Nelson, Christian J.; Sadeghi-Nejad, Hossein; Seftel, Allen D.; Shindel, Alan W. (September 2018). "Erectile Dysfunction: AUA Guideline". Journal of Urology. 200 (3): 633–641. doi:10.1016/j.juro.2018.05.004. PMID 29746858.
- 1 2 3 Anaissie, James; Yafi, Faysal A. (June 2016). "A review of surgical strategies for penile prosthesis implantation in patients with Peyronie's disease". Translational Andrology and Urology. 5 (3): 342–350. doi:10.21037/tau.2016.04.04. PMC 4893506. PMID 27298781.
- ↑ Falcone, Marco; Garaffa, Giulio; Gillo, Arianna; Dente, Dino; Christopher, Andrew N.; Ralph, David J. (January 2018). "Outcomes of inflatable penile prosthesis insertion in 247 patients completing female to male gender reassignment surgery". BJU International. 121 (1): 139–144. doi:10.1111/bju.14027. PMID 28940910.
- ↑ Puckett, Charles L.; Montie, Joseph E. (April 1978). "Construction of Male Genitalia in the Transsexual, Using a Tubed Groin Flap for the Penis and a Hydraulic Inflation Device". Plastic and Reconstructive Surgery. 61 (4): 523–530. doi:10.1097/00006534-197804000-00005. PMID 345304. S2CID 42344243.
- ↑ Neuville, Paul; Morel-Journel, Nicolas; Cabelguenne, Delphine; Ruffion, Alain; Paparel, Philippe; Terrier, Jean-Etienne (February 2019). "First Outcomes of the ZSI 475 FtM, a Specific Prosthesis Designed for Phalloplasty". The Journal of Sexual Medicine. 16 (2): 316–322. doi:10.1016/j.jsxm.2018.11.013. PMID 30638882.
- 1 2 3 Krzastek, Sarah C.; Smith, Ryan (8 January 2019). "An update on the best approaches to prevent complications in penile prosthesis recipients". Therapeutic Advances in Urology. 11: 175628721881807. doi:10.1177/1756287218818076. PMC 6329024. PMID 30671142.
- ↑ Çayan, Selahittin; Aşcı, Ramazan; Efesoy, Ozan; Bolat, Mustafa Suat; Akbay, Erdem; Yaman, Önder (July 2019). "Comparison of Long-Term Results and Couples' Satisfaction with Penile Implant Types and Brands: Lessons Learned From 883 Patients With Erectile Dysfunction Who Underwent Penile Prosthesis Implantation". The Journal of Sexual Medicine. 16 (7): 1092–1099. doi:10.1016/j.jsxm.2019.04.013. PMID 31155387. S2CID 173992578.
- ↑ Ziegelmann, Matthew J.; Alom, Manaf; Bole, Raevti; Kohler, Tobias; Trost, Landon (June 2018). "Modified Glanulopexy Technique for Supersonic Transporter Deformity and Glanular Hypermobility in Men With Penile Prostheses". The Journal of Sexual Medicine. 15 (6): 914–919. doi:10.1016/j.jsxm.2018.04.633. PMID 29731427. S2CID 24785737.