Gastric bypass surgery
| Gastric bypass surgery | |
|---|---|
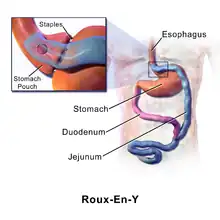
A diagram of a gastric bypass (Roux-en-Y). | |
| ICD-9-CM | 44.31-44.39 |
| MeSH | D015390 |
| MedlinePlus | 007199 |
Gastric bypass surgery refers to a technique in which the stomach is divided into a small upper pouch and a much larger lower "remnant" pouch and then the small intestine is rearranged to connect to both. Surgeons have developed several different ways to reconnect the intestine, thus leading to several different gastric bypass procedures (GBP). Any GBP leads to a marked reduction in the functional volume of the stomach, accompanied by an altered physiological and physical response to food.
The operation is prescribed to treat morbid obesity (defined as a body mass index greater than 40), type 2 diabetes, hypertension, sleep apnea, and other comorbid conditions. Bariatric surgery is the term encompassing all of the surgical treatments for morbid obesity, not just gastric bypasses, which make up only one class of such operations. The resulting weight loss, typically dramatic, markedly reduces comorbidities. The long-term mortality rate of gastric bypass patients has been shown to be reduced by up to 40%.[journal 1][journal 2] As with all surgery, complications may occur. A study from 2005 to 2006 revealed that 15% of patients experience complications as a result of gastric bypass, and 0.5% of patients died within six months of surgery due to complications.[press release 1] A meta-analysis of 174,772 participants published in The Lancet in 2021 found that bariatric surgery was associated with 59% and 30% reduction in all-cause mortality among obese adults with or without type 2 diabetes respectively.[1] This meta-analysis also found that median life-expectancy was 9.3 years longer for obese adults with diabetes who received bariatric surgery as compared to routine (non-surgical) care, whereas the life expectancy gain was 5.1 years longer for obese adults without diabetes.[1]
Uses
Gastric bypass is indicated for the surgical treatment of morbid obesity, a diagnosis which is made when the patient is seriously obese, has been unable to achieve satisfactory and sustained weight loss by dietary efforts, and suffers from comorbid conditions which are either life-threatening or a serious impairment to the quality of life.
Prior to 1991, clinicians interpreted serious obesity as weighing at least 100 pounds (45 kg) more than the "ideal body weight", an actuarially-determined body-weight at which one was estimated to be likely to live the longest, as determined by the life-insurance industry. This criterion failed for persons of short stature.
In 1991, the National Institutes of Health (NIH) sponsored a consensus panel whose recommendations have set the current standard for consideration of surgical treatment, the body mass index (BMI). The BMI is defined as the body weight (in kilograms), divided by the square of the height (in meters). The result is expressed as a number in units of kilograms per square meter. In healthy adults, BMI ranges from 18.5 to 24.9, with a BMI above 30 being considered obese, and a BMI less than 18.5 considered underweight.[web 1]
The Consensus Panel of the National Institutes of Health (NIH) recommended the following criteria for consideration of bariatric surgery, including gastric bypass procedures:
- people who have a BMI of 40 or higher[journal 3]
- people with a BMI of 35 or higher with one or more related comorbid conditions[journal 3]
The Consensus Panel also emphasized the necessity of multidisciplinary care of the bariatric surgical patient by a team of physicians and therapists to manage associated comorbidities and nutrition, physical activity, behavior, and psychological needs. The surgical procedure is best regarded as a tool which enables the patient to alter lifestyle and eating habits, and to achieve effective and permanent management of obesity and eating behavior.
Since 1991, major developments in the field of bariatric surgery, particularly laparoscopy, have outdated some of the conclusions of the NIH panel. In 2004 the American Society for Bariatric Surgery (ASBS) sponsored a consensus conference which updated the evidence and the conclusions of the NIH panel. This conference, composed of physicians and scientists of both surgical and non-surgical disciplines, reached several conclusions, including:
- bariatric surgery is the most effective treatment for morbid obesity
- gastric bypass is one of four types of operations for morbid obesity
- laparoscopic surgery is equally effective and as safe as open surgery
- patients should undergo comprehensive preoperative evaluation and have multi-disciplinary support for optimum outcome
Surgical techniques
The gastric bypass, in its various forms, accounts for a large majority of the bariatric surgical procedures performed. It is estimated that 200,000 such operations were performed in the United States in 2008.[journal 4]
Laparoscopic surgery is performed using several small incisions, or ports: one to insert a surgical telescope connected to a video camera, and others to permit access of specialized operating instruments. The surgeon views the operation on a video screen. Laparoscopy is also called limited access surgery, reflecting the limitation on handling and feeling tissues and also the limited resolution and two-dimensionality of the video image. With experience, a skilled laparoscopic surgeon can perform most procedures as expeditiously as with an open incision—with the option of using an incision should the need arise.[journal 5]
The Roux-en-Y laparoscopic gastric bypass, first performed in 1993, is regarded as one of the most difficult procedures to perform by limited access techniques, but use of this method has greatly popularized the operation due to associated benefits such as a shortened hospital stay, reduced discomfort, shorter recovery time, less scarring, and minimal risk of incisional hernia.[journal 5]
Essential features
The gastric bypass procedure consists of:
- Creation of a small, (15–30 ml/1–2 tbsp) thumb-sized pouch from the upper stomach, accompanied by bypass of the remaining stomach (about 400 ml and variable). This restricts the volume of food which can be eaten. The stomach may simply be partitioned (like a wall between two rooms in a house or two office cubicles next to each other with a partition wall in between them—and typically by the use of surgical staples), or it may be totally divided into two separate/separated parts (also with staples). Total division (separate/separated parts) is usually advocated to reduce the possibility that the two parts of the stomach will heal back together ("fistulize") and negate the operation.
- Re-construction of the GI tract to enable drainage of both segments of the stomach. The particular technique used for this reconstruction produces several variants of the operation, differing in the lengths of small intestine used, the degree to which food absorption is affected, and the likelihood of adverse nutritional effects. Usually, a segment of the small bowel (called the alimentary limb) is brought up to the proximal remains of the stomach.
Variations
Gastric bypass, Roux-en-Y (RYGB, proximal)

This variant is the most commonly employed gastric bypass technique, and is by far the most commonly performed bariatric procedure in the United States. The small intestine is divided approximately 45 cm (18 in) below the lower stomach outlet and is re-arranged into a Y-configuration, enabling outflow of food from the small upper stomach pouch via a "Roux limb". In the proximal version, the Y-intersection is formed near the upper (proximal) end of the small intestine. The Roux limb is constructed using 80–150 cm (31–59 in) of the small intestine, preserving the rest (and the majority) of it from absorbing nutrients. The patient will experience very rapid onset of the stomach feeling full, followed by a growing satiety (or "indifference" to food) shortly after the start of a meal.
Gastric bypass, Roux-en-Y (RYGB, distal)
The small intestine is normally 6–10 m (20–33 ft) in length. As the Y-connection is moved further down the gastrointestinal tract, the amount available to fully absorb nutrients is progressively reduced, traded for greater effectiveness of the operation. The Y-connection is formed much closer to the lower (distal) end of the small intestine, usually 100–150 cm (39–59 in) from the lower end, causing reduced absorption (malabsorption) of food: primarily of fats and starches, but also of various minerals and the fat-soluble vitamins. The unabsorbed fats and starches pass into the large intestine, where bacterial actions may act on them to produce irritants and malodorous gases. These larger effects on nutrition are traded for a relatively modest increase in total weight loss.
Mini-gastric bypass (MGB)
The mini-gastric bypass procedure was first developed by Robert Rutledge from the US in 1997, as a modification of the standard Billroth II procedure. A mini gastric bypass creates a long narrow tube of the stomach along its right border (the lesser curvature). A loop of the small gut is brought up and hooked to this tube at about 180 cm from the start of the intestine.
Numerous studies show that the loop reconstruction (Billroth II gastrojejunostomy) works more safely when placed low on the stomach, but can be a disaster when placed adjacent to the esophagus. Today thousands of "loops" are used for surgical procedures to treat gastric problems such as ulcers, stomach cancer, and injury to the stomach. The mini-gastric bypass uses the low set loop reconstruction and thus has rare chances of bile reflux.
The MGB has been suggested as an alternative to the Roux-en-Y procedure due to the simplicity of its construction and is becoming more and more popular because of low risk of complications and good sustained weight loss. It has been estimated that 15.4% of weight loss surgery in Asia is now performed via the MGB technique.[journal 6]
Endoscopic duodenal-jejunal bypass
This technique has been clinically researched since the mid-2000s. It involves the implantation of a duodenal-jejunal bypass liner between the beginning of the duodenum (first portion of the small intestine from the stomach) and the mid-jejunum (the secondary stage of the small intestine). This prevents the partially digested food from entering the first and initial part of the secondary stage of the small intestine, mimicking the effects of the biliopancreatic portion of Roux-en-Y gastric bypass (RYGB) surgery. Despite a handful of serious adverse events such as gastrointestinal bleeding, abdominal pain, and device migration – all resolved with device removal – initial clinical trials have produced promising results in the treatment's ability to improve weight loss and glucose homeostasis outcomes.[book 1][book 2][web 2]
Physiology
The gastric bypass reduces the size of the stomach by well over 90%.[2] A normal stomach can stretch, sometimes to over 1000 mL, while the pouch of the gastric bypass may be 15 mL in size. The gastric bypass pouch is usually formed from the part of the stomach which is least susceptible to stretching. That, and its small original size, prevents any significant long-term change in pouch volume. What does change, over time, is the size of the connection between the stomach and intestine and the ability of the small intestine to hold a greater volume of food. Over time, the functional capacity of the pouch increases; by that time, weight loss has occurred, and the increased capacity should serve to allow maintenance of a lower body weight.
When the patient ingests just a small amount of food, the first response is a stretching of the wall of the stomach pouch, stimulating nerves that tell the brain that the stomach is full. The patient feels a sensation of fullness, as if they had just eaten a large meal—but with just a thimble-full of food. Most people do not stop eating simply in response to a feeling of fullness, but the patient rapidly learns that subsequent bites must be eaten very slowly and carefully, to avoid increasing discomfort or vomiting.
Food is first churned in the stomach before passing into the small intestine. When the lumen of the small intestine comes into contact with nutrients, a number of hormones are released, including cholecystokinin from the duodenum and PYY and GLP-1 from the ileum. These hormones inhibit further food intake and have thus been dubbed "satiety factors". Ghrelin is a hormone that is released in the stomach that stimulates hunger and food intake. Changes in circulating hormone levels after gastric bypass have been hypothesized to produce reductions in food intake and body weight in obese patients. However, these findings remain controversial, and the exact mechanisms by which gastric bypass surgery reduces food intake and body weight have yet to be elucidated.
For example, it is still widely perceived that gastric bypass works by mechanical means, i.e. food restriction and/or malabsorption. Recent clinical and animal studies, however, have indicated that these long-held inferences about the mechanisms of Roux-en-Y gastric bypass (RYGB) may not be correct. A growing body of evidence suggests that profound changes in body weight and metabolism resulting from RYGB cannot be explained by simple mechanical restriction or malabsorption. One study in rats found that RYGB induced a 19% increase in total and a 31% increase in resting energy expenditure, an effect not exhibited in vertical sleeve gastrectomy rats. In addition, pair-fed rats lost only 47% as much weight as their RYGB counterparts. Changes in food intake after RYGB only partially account for the RYGB-induced weight loss, and there is no evidence of clinically significant malabsorption of calories contributing to weight loss. Thus, it appears RYGB affects weight loss by altering the physiology of weight regulation and eating behavior rather than by simple mechanical restriction or malabsorption.[journal 7]
To gain the maximum benefit from this physiology, it is important that the patient eat only at mealtimes, 5 to 6 small meals daily, and not graze between meals. Concentration on obtaining 80–100 g of daily protein is necessary. Meals after surgery are ¼–½ cup, slowly getting to 1 cup by one year. This requires a change in eating behavior and an alteration of long-acquired habits for finding food. In almost every case where weight gain occurs late after surgery, capacity for a meal has not greatly increased. Some assume the cause of regaining weight must be the patient's fault, e.g. eating between meals with high-caloric snack foods, though this has been debated. Others believe it is an unpredictable failure or limitation of the surgery for certain patients (e.g. reactive hypoglycemia).
Complications
Any major surgery involves the potential for complications—adverse events that increase risk, hospital stay, and mortality. Some complications are common to all abdominal operations, while some are specific to bariatric surgery.
Mortality and complication rates
The overall rate of complications during the 30 days following surgery ranges from 7% for laparoscopic procedures to 14.5% for operations through open incisions. One study on mortality revealed a 0% mortality rate out of 401 laparoscopic cases, and 0.6% out of 955 open procedures. Similar mortality rates—30-day mortality of 0.11%, and 90-day mortality of 0.3%—have been recorded in the U.S. Centers of Excellence program, the results being from 33,117 operations at 106 centers.[web 3]
Mortality and complications are affected by pre-existing risk factors such as degree of obesity, heart disease, obstructive sleep apnea, diabetes mellitus, and history of prior pulmonary embolism. It is also affected by the experience of the operating surgeon: the learning curve for laparoscopic bariatric surgery is estimated to be about 100 cases. Supervision and experience are important when selecting a surgeon, as the way a surgeon becomes experienced in dealing with problems is by encountering and solving them.
Complications of abdominal surgery
Infection
Infection of the incisions or of the inside of the abdomen (peritonitis, abscess) may occur due to the release of bacteria from the bowel during the operation. Nosocomial infections, such as pneumonia, bladder or kidney infections, and sepsis (blood-borne infection) are also possible. Effective short-term use of antibiotics, diligent respiratory therapy, and encouragement of activity within a few hours after surgery can reduce the risks of infections.
Venous thromboembolism
Any injury, such as a surgical operation, causes the body to increase the coagulation of the blood. Simultaneously, activity may be reduced. There is an increased probability of formation of clots in the veins of the legs, or sometimes the pelvis, particularly in the morbidly obese patient. A clot that breaks free and floats to the lungs is called a pulmonary embolus, a very dangerous occurrence. Blood thinners are commonly administered before surgery to reduce the probability of this type of complication.
Hemorrhage
Many blood vessels must be cut in order to divide the stomach and to move the bowel. Any of these may later begin bleeding, either into the abdomen (intra-abdominal hemorrhage) or into the bowel itself (gastrointestinal hemorrhage). Transfusions may be needed, and re-operation is sometimes necessary. The use of blood thinners to prevent venous thromboembolic disease may actually increase the risk of hemorrhage slightly.
Hernia
A hernia is an abnormal opening, either within the abdomen or through the abdominal wall muscles. An internal hernia may result from surgery and re-arrangement of the bowel and is a cause of bowel obstruction. Antecolic antegastric Roux-en-Y gastric bypass surgery has been estimated to result in internal hernia in 0.2% of cases, mainly through Petersen's defect.[journal 8] An incisional hernia occurs when a surgical incision does not heal well; the muscles of the abdomen separate and allow protrusion of a sac-like membrane, which may contain bowel or other abdominal contents, and which can be painful and unsightly. The risk of abdominal-wall hernia is markedly decreased in laparoscopic surgery.
Bowel obstruction
Abdominal surgery always results in some scarring of the bowel, called adhesions. A hernia, either internal or through the abdominal wall, may also result. When the bowel becomes trapped by adhesions or a hernia, it may become kinked and obstructed, sometimes many years after the original procedure. An operation is usually necessary to correct this problem.
Complications of gastric bypass
Anastomotic leakage
An anastomosis is a surgical connection between the stomach and bowel, or between two parts of the bowel. The surgeon attempts to create a water-tight connection by connecting the two organs with either staples or sutures, either of which actually makes a hole in the bowel wall. The surgeon will rely on the body's natural healing abilities and its ability to create a seal, like a self-sealing tire, to succeed with the surgery. If that seal fails to form for any reason, fluid from within the gastrointestinal tract can leak into the sterile abdominal cavity and give rise to infection and abscess formation. Leakage of an anastomosis can occur in about 2% of Roux-en-Y gastric bypass and less than 1% in mini gastric bypass. Leaks usually occur at the stomach-intestine connection (gastro-jejunostomy).
Anastomotic stricture
As the anastomosis heals, it forms scar tissue, which naturally tends to shrink ("contract") over time, making the opening smaller. This is called a "stricture". Usually, the passage of food through an anastomosis will keep it stretched open, but if the inflammation and healing process outpaces the stretching process, scarring may make the opening so small that even liquids can no longer pass through it. The solution is a procedure called gastro endoscopy, and stretching of the connection by inflating a balloon inside it. Sometimes this manipulation may have to be performed more than once to achieve lasting correction.
Anastomotic ulcer
Ulceration of the anastomosis occurs in 1–16% of patients.[journal 9] Possible causes of such ulcers are:
- Restricted blood supply to the anastomosis (compared to the blood supply available to the original stomach)
- Anastomosis tension
- Gastric acid
- The bacteria Helicobacter pylori
- Smoking
- Use of non-steroidal anti-inflammatory drugs
This condition can be treated with:
- Proton pump inhibitors, e.g. esomeprazole
- A cytoprotectant and acid buffering agent, e.g. sucralfate
- Temporary restriction of the consumption of solid foods
Dumping syndrome
Normally, the pyloric valve at the lower end of the stomach regulates the release of food into the bowel. When the gastric bypass patient eats a sugary food, the sugar passes rapidly into the intestine, where it gives rise to a physiological reaction called dumping syndrome. The body will flood the intestines with gastric content in an attempt to dilute the sugars. An affected person may feel their heart beating rapidly and forcefully, break into a cold sweat, get a feeling of butterflies in the stomach, and may have an anxiety attack. The person usually has to lie down and could be very uncomfortable for 30–45 minutes. Diarrhea may then follow.
Nutritional deficiencies
Nutritional deficiencies are common after gastric bypass surgery, and are often not recognized. They include:[journal 10]
- Secondary hyperparathyroidism due to inadequate absorption of calcium may occur for GBP patients. Calcium is primarily absorbed in the duodenum, which is bypassed by the surgery. Most patients can achieve adequate calcium absorption by supplementation with vitamin D and calcium citrate (carbonate may not be absorbed—it requires an acidic stomach, which is bypassed).
- Iron frequently is seriously deficient, particularly in menstruating females, and must be supplemented. Again, it is normally absorbed in the duodenum. Ferrous sulfate can cause considerable GI distress in normal doses; alternatives include ferrous fumarate, or a chelated form of iron. Occasionally, a female patient develops severe anemia, even with supplements, and must be treated with parenteral iron. The signs of iron deficiency include: brittle nails, an inflamed tongue, constipation, depression, headaches, fatigue, and mouth lesions.[journal 11]
- Signs and symptoms of zinc deficiency may also occur such as: acne, eczema, white spots on the nails, hair loss, depression, amnesia, and lethargy.[journal 12]
- Deficiency of thiamine (also known as vitamin B1) brings the risk of permanent neurological damage (i.e. Wernicke's encephalopathy or polyneuropathy). Signs of thiamin deficiency are heart failure, memory loss, numbness of the hands, constipation, and loss of appetite.[journal 11]
- Vitamin B12 requires intrinsic factor from the gastric mucosa to be absorbed. In patients with a small gastric pouch, it may not be absorbed, even if supplemented orally, and deficiencies can result in pernicious anemia and neuropathies. Vitamin B12 deficiency is quite common after gastric bypass surgery with reported rates of 30% in some clinical trials.[journal 13] Sublingual B12 (cyanocobalamin) appears to be adequately absorbed. In cases where sublingual B12 does not provide sufficient amounts, injections may be needed.
- Protein malnutrition is a real risk. Some patients suffer troublesome vomiting after surgery, until their GI tract adjusts to the changes, and cannot eat adequate amounts even with 6 meals a day. Many patients require protein supplementation during the early phases of rapid weight loss to prevent excessive loss of muscle mass. Hair loss is also a risk of protein malnutrition.
- Vitamin A deficiencies generally occur as a result of fat-soluble vitamins deficiencies. This often comes after intestinal bypass procedures such as jejunoileal bypass (no longer performed) or biliopancreatic diversion/duodenal switch procedures. In these procedures, fat absorption is markedly impaired. There is also the possibility of a vitamin A deficiency with use of the weight-loss medication orlistat (marketed as Xenical and Alli).
- Folate deficiency is also a common occurrence in gastric bypass surgery patients.
Nutritional effects
After surgery, patients feel fullness after ingesting only a small volume of food, followed soon thereafter by a sense of satiety and loss of appetite. Total food intake is markedly reduced. Due to the reduced size of the newly created stomach pouch, and reduced food intake, adequate nutrition demands that the patient follow the surgeon's instructions for food consumption, including the number of meals to be taken daily, adequate protein intake, and the use of vitamin and mineral supplements. Calcium supplements, iron supplements, protein supplements, multi-vitamins (sometimes pre-natal vitamins are best), and vitamin B12 (cyanocobalamin) supplements are all very important to the post-operative bypass patient.
Total food intake and absorbance rate of food will rapidly decline after gastric bypass surgery, and the number of acid-producing cells lining the stomach increases. Doctors often prescribe acid-lowering medications to counteract the high acidity levels. Many patients then experience a condition known as achlorhydria, where there is not enough acid in the stomach. As a result of the low acidity levels, patients can develop an overgrowth of bacteria. A study conducted on 43 post-operative patients revealed that almost all of the patients tested positive for a hydrogen breath test, which indicated an overgrowth of bacteria in the small intestine.[journal 14] Bacterial overgrowth causes the gut ecology to change and induces nausea and vomiting. Recurring nausea and vomiting eventually change the absorbance rate of food, contributing to the vitamin and nutrition deficiencies common in post-operative gastric bypass patients.
Protein nutrition
Proteins are essential food substances, contained in foods such as meat, fish, poultry, dairy products, eggs, vegetables, fruits, legumes and nuts. With reduced ability to eat a large volume of food, gastric bypass patients must focus on eating their protein requirements first, and with each meal. In some cases, surgeons may recommend use of a liquid protein supplement. Powdered protein supplements added to smoothies or any food can be an important part of the post-op diet.
Calorie nutrition
The profound weight loss which occurs after bariatric surgery is due to taking in much less energy (calories) than the body needs to use every day. Fat tissue must be burned to offset the deficit, and weight loss results. Eventually, as the body becomes smaller, its energy requirements are decreased, while the patient simultaneously finds it possible to eat somewhat more food. When the energy consumed is equal to the calories eaten, weight loss will stop. Proximal GBP typically results in loss of 60–80% of excess body weight, and very rarely leads to excessive weight loss. The risk of excessive weight loss is slightly greater with distal GBP.
Vitamins
Vitamins are normally contained in foods and supplements. The amount of food eaten after GBP is severely reduced, and vitamin content is correspondingly lowered. Supplements should therefore be taken to complete minimum daily requirements of all vitamins and minerals. Pre-natal vitamins are sometimes suggested by doctors, as they contain more of certain vitamins than most multi-vitamins. Absorption of most vitamins is not seriously affected after proximal GBP, although vitamin B12 may not be well-absorbed in some persons: sublingual preparations of B12 provide adequate absorption. Some studies suggest that GBP patients who took probiotics after surgery are able to absorb and retain higher amounts of B12 than patients who did not take probiotics after surgery. After a distal GBP, fat-soluble vitamins A, D, and E may not be well-absorbed, particularly if fat intake is large. Water-dispersed forms of these vitamins may be indicated on specific physician recommendation. For some patients, sublingual B12 is not enough, and patients may require B12 injections.
Minerals
All versions of the GBP bypass the duodenum, which is the primary site of absorption of both iron and calcium. Iron replacement is essential in menstruating females, and supplementation of iron and calcium is preferable in all patients. Ferrous sulfate is poorly tolerated. Alternative forms of iron (fumarate, gluconate, chelates) are less irritating and probably better absorbed. Calcium carbonate preparations should also be avoided; calcium as citrate or gluconate (with 1200 mg as calcium) has greater bioavailability independent of acid in the stomach, and will likely be better absorbed. Chewable calcium supplements that include vitamin K are sometimes recommended by doctors as a good way to get calcium.
Alcohol metabolism
Post-operative gastric bypass patients develop a lowered tolerance for alcoholic beverages because their altered digestive tract absorbs alcohol at a faster rate than people who have not undergone the surgery. It also takes a post-operative patient longer to reach sober levels after consuming alcohol. In a study conducted on 36 post-operative patients and a control group of 36 subjects (who had not undergone surgery), each subject drank a 5 oz. glass of red wine and had the alcohol in their breath measured to evaluate alcohol metabolism. The gastric bypass group had an average peak alcohol breath level at 0.08%, whereas the control group had an average peak alcohol breath level of 0.05%. It took on average 108 minutes for the gastric bypass patients group to return to an alcohol breath of zero, while it took the control group an average of 72 minutes.[journal 15]
Pica
There have been reported cases in which pica recurs after gastric bypass in patients with a pre-operative history of the disorder, which are possibly due to iron deficiency. Pica is a compulsive tendency to eat substances other than normal food. Some examples would be people eating paper, clay, plaster, ashes, or ice. Low levels of iron and hemoglobin are common in patients who have undergone gastric bypass.[web 4] One study reported on a female post-operative gastric bypass patient who was consuming eight to ten 32 oz. glasses of ice a day. The patient's blood test revealed iron levels of 2.3 mmol/L and hemoglobin level of 5.83 mmol/L. Normal iron blood levels of adult women are 30 to 126 µg/dL and normal hemoglobin levels are 12.1 to 15.1 g/dl. This deficiency in the patient's iron levels may have led to the increase Pica activity. The patient was then given iron supplements that brought her hemoglobin and iron blood levels to normal levels. After one month, the patient's eating diminished to two to three glasses of ice per day. After one year of taking iron supplements the patient's iron and hemoglobin levels remained in a normal range and the patient reported that she did not have any further cravings for ice.[journal 16]
Results and health benefits of gastric bypass
Weight loss of 65–80% of excess body weight is typical of most large series of gastric bypass operations reported. The medically more significant effects include a dramatic reduction in comorbid conditions:
- Hyperlipidemia is corrected in over 70% of patients.
- Essential hypertension is relieved in over 70% of patients, and medication requirements are usually reduced in the remainder.
- Obstructive sleep apnea improves markedly with weight loss and bariatric surgery may be curative for sleep apnea. Snoring also reduces in most patients.
- Type 2 diabetes is reversed in up to 90% of patients[news 1] usually leading to a normal blood-sugar level without medication, sometimes within days of surgery.
[journal 17][journal 18] Furthermore, Type 2 diabetes is prevented by more than 30-fold in patients with pre-diabetes. All these findings were first reported by Walter Pories and Jose F. Caro.[journal 19]
- Gastroesophageal reflux disease is relieved in almost all patients.
- Venous thromboembolic disease signs such as leg swelling are typically alleviated.
- Lower-back pain and joint pain are typically relieved or improved in nearly all patients.
A study in a large prospective study of 2010 obese patients showed a 29% reduction in mortality up to 15 years following surgery (hazard ratio 0.71 when adjusted for sex, age, and risk factors), compared to a non-surgically treated group of 2037 patients.[journal 2] A meta-analysis of 174772 participants published in The Lancet in 2021 found that bariatric surgery was associated with 59% and 30% reduction in all-cause mortality among obese adults with or without type 2 diabetes respectively.[1] This meta-analysis also found that median life-expectancy was 9.3 years longer for obese adults with diabetes who received bariatric surgery as compared to routine (non-surgical) care, whereas the life expectancy gain was 5.1 years longer for obese adults without diabetes.[1]
Concurrently, most patients are able to enjoy greater participation in family and social activities.
Cost of gastric bypass
The patient's out-of-pocket cost for Roux-en-Y gastric bypass surgery varies widely depending on method of payment, region, surgical practice and hospital in which the procedure is performed.
Methods of payment in the United States include private insurance (Individual & Family coverage, Small Group coverage through an employer (Under 50 full-time employees) and Large Group coverage through an employer (50 or more full-time employees), public insurance (Medicare and Medicaid) and self-pay. Out of pocket costs for a patient with private or public insurance that specifically list bariatric surgery as a covered benefit include several insurance-policy-specific parameters such as deductible levels, coinsurance percentages, copay amounts and out of pocket limits.
Patients without insurance must pay for surgery directly (or through a third party lender), and total out of pocket costs will depend on the surgical practice they choose and the hospital in which the surgical practice performs the procedure. On average, the total cost of gastric bypass surgery is about $24,000 in the United States, although on a state-specific level it ranges from an average of $15,000 (Arkansas) to an average of $57,000 (Alaska).[web 5]
In Germany a gastric bypass operation, if not covered by health insurance and therefore paid privately, costs up to €15,000;[web 6] in Switzerland CHF 20,000–25,000,[news 2] in Poland gastric bypass costs around £4,000, whereas in Turkey it costs £3200.[3]
Living with gastric bypass
Gastric bypass surgery has an emotional and physiological impact on the individual. Many who have undergone the surgery suffer from depression in the following months as a result of a change in the role food plays in their emotional well-being.[journal 20] Strict limitations on the diet can place great emotional strain on the patient. Energy levels in the period following the surgery can be low, both due to the restriction of food intake and negative changes in emotional state.[journal 21] It may take as long as three months for emotional levels to rebound.
Muscular weakness in the months following surgery is also common. This is caused by a number of factors, including a restriction on protein intake, a resulting loss in muscle mass and decline in energy levels. Muscle weakness may result in balance problems, difficulty climbing stairs or lifting heavy objects, and increased fatigue following simple physical tasks. Many of these issues pass over time as food intake gradually increases. However, the first months following the surgery can be very difficult, an issue not often mentioned by physicians suggesting the surgery. The benefits and risks of this surgery are well established; however, the psychological effects are not well understood.
Even if physical activity is increased, patients may still harbor long term psychological effects due to excess skin and fat. Often bypass surgery is followed up with "body lifts" of skin and liposuction of fatty deposits. These extra surgeries have their own inherent risks but are even more dangerous when coupled with the typical nutritional deficiences that accompany convalescing gastric bypass patients.
Surgeon accreditation
The American Society for Metabolic & Bariatric Surgery lists bariatric programs and surgeons in its "Centers of Excellence" network,[web 7] while the American College of Surgeons accredits providers through its Bariatric Surgery Center Network.[web 8] For listings of surgeons and centers in other countries, the International Federation for the Surgery of Obesity and Metabolic Disorders lists medical associations by country.[web 9]
See also
- Adjustable gastric band
- Duodenal switch surgery
- StomaphyX—Revisional, natural orifice procedure for patients that have regained weight after gastric bypass
- Vagotomy—Cutting of the vagus nerve to reduce the feeling of hunger
References
- 1 2 3 4 Syn, Nicholas L.; Cummings, David E.; Wang, Louis Z.; Lin, Daryl J.; Zhao, Joseph J.; Loh, Marie; Koh, Zong Jie; Chew, Claire Alexandra; Loo, Ying Ern; Tai, Bee Choo; Kim, Guowei (15 May 2021). "Association of metabolic-bariatric surgery with long-term survival in adults with and without diabetes: a one-stage meta-analysis of matched cohort and prospective controlled studies with 174 772 participants". Lancet. 397 (10287): 1830–1841. doi:10.1016/S0140-6736(21)00591-2. ISSN 1474-547X. PMID 33965067. S2CID 234345414.
- ↑ Chen M, Krishnamurthy A, Mohamed AR, Green R (July 2013). "Hematological Disorders following Gastric Bypass Surgery: Emerging Concepts of the Interplay between Nutritional Deficiency and Inflammation". BioMed Research International. Biomed Res Int. 2013: 205467. doi:10.1155/2013/205467. PMC 3741944. PMID 23984326.
- ↑ "Gastric Bypass Weight Loss Surgery: cost UK, diet, side effects, pre-op diet". Clinic Hunter - Find a clinic and get a treatment abroad. Retrieved 1 April 2021.
Books
- ↑ Shelby S (2015). "Endoscopic Treatment of Obesity". In Jonnalagadda SS (ed.). Gastrointestinal Endoscopy: New Technologies and Changing Paradigms (2015 ed.). Springer Publishing (published 26 February 2015). pp. 61–82. doi:10.1007/978-1-4939-20317 (inactive 31 October 2021). ISBN 978-1493920310. OCLC 945669699. Retrieved 18 March 2016.
{{cite book}}: CS1 maint: DOI inactive as of October 2021 (link) - ↑ Muñoz R, Escalona A (2015). "Chapter 51: Endoscopic Duodenal-Jejunal Bypass Sleeve Treatment for Obesity". In Agrawal S (ed.). Obesity, Bariatric and Metabolic Surgery: A Practical Guide (2015 ed.). Springer Publishing (published 15 September 2015). pp. 493–498. doi:10.1007/978-3-319-04343-2. ISBN 978-3319043425. OCLC 930041021. Retrieved 18 March 2016.
Journal sources
- ↑ Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, Rosamond WD, et al. (August 2007). "Long-term mortality after gastric bypass surgery". The New England Journal of Medicine (Journal Article). Massachusetts Medical Society (published 23 August 2007). 357 (8): 753–61. doi:10.1056/NEJMoa066603. eISSN 1533-4406. LCCN 20020456. OCLC 231027780. PMID 17715409. S2CID 8710295.
During a mean follow-up of 7.1 years, adjusted long-term mortality from any cause in the surgery group decreased by 40%, as compared with that in the control group (37.6 vs. 57.1 deaths per 10,000 person-years, P<0.001); cause-specific mortality in the surgery group decreased by 56% for coronary artery disease (2.6 vs. 5.9 per 10,000 person-years, P=0.006), by 92% for diabetes (0.4 vs. 3.4 per 10,000 person-years, P=0.005), and by 60% for cancer (5.5 vs. 13.3 per 10,000 person-years, P<0.001).
- 1 2 Sjöström L, Narbro K, Sjöström CD, Karason K, Larsson B, Wedel H, et al. (August 2007). "Effects of bariatric surgery on mortality in Swedish obese subjects". The New England Journal of Medicine (Journal Article). Massachusetts Medical Society (published 23 August 2007). 357 (8): 741–52. doi:10.1056/NEJMoa066254. eISSN 1533-4406. LCCN 20020456. OCLC 231027780. PMID 17715408. S2CID 20533869.
Bariatric surgery for severe obesity is associated with long-term weight loss and decreased overall mortality.
- 1 2 Cummings DE, Cohen RV (February 2014). "Beyond BMI: the need for new guidelines governing the use of bariatric and metabolic surgery". The Lancet. Diabetes & Endocrinology. Bariatric Surgery. 2 (2): 175–81. doi:10.1016/S2213-8587(13)70198-0. eISSN 1474-547X. LCCN sf82002015. OCLC 1755507. PMC 4160116. PMID 24622721.
... the National Institutes of Health recommendations had important limitations from the outset and are now gravely outdated. They do not account for remarkable advances in minimally invasive surgical techniques or the development of entirely new procedures. In the two decades since they were crafted, we have gained far greater understanding of the dramatic, weight-independent benefits of some operations on metabolic diseases, especially type 2 diabetes, and of the inadequacy of BMI as a primary criterion for surgical selection.
- ↑ McTigue KM, Wellman R, Nauman E, Anau J, Coley RY, Odor A, et al. (March 2020). "Comparing the 5-Year Diabetes Outcomes of Sleeve Gastrectomy and Gastric Bypass: The National Patient-Centered Clinical Research Network (PCORNet) Bariatric Study". JAMA Surgery. 155 (5): e200087. doi:10.1001/jamasurg.2020.0087. PMC 7057171. PMID 32129809.
- 1 2 Wittgrove AC, Clark GW (June 2000). "Laparoscopic gastric bypass, Roux-en-Y- 500 patients: technique and results, with 3-60 month follow-up". Obesity Surgery (Journal Article). Springer-Verlag (published 1 June 2000). 10 (3): 233–9. doi:10.1381/096089200321643511. eISSN 1708-0428. LCCN 2001301458. OCLC 23835796. PMID 10929154. S2CID 33015279.
We began to explore techniques for laparoscopic performance of the gastric bypass in 1993, adhering to the fundamental principle that essential features of the open operation must not be modified or compromised, to achieve the limited access technique. After laboratory verification of the instrument techniques, we performed our first procedure in late 1993.
- ↑ Lomanto D, Lee WJ, Goel R, Lee JJ, Shabbir A, So JB, et al. (March 2012). "Bariatric surgery in Asia in the last 5years (2005-2009)". Obesity Surgery (Journal Article). Springer-Verlag (published 1 March 2012). 22 (3): 502–6. doi:10.1007/s11695-011-0547-2. eISSN 1708-0428. LCCN 2001301458. OCLC 23835796. PMID 22033767. S2CID 207304196.
For combined years 2005-2009, the four most commonly performed procedures were laparoscopic adjustable gastric banding (LAGB, 35.9%), laparoscopic standard Roux-en-Y gastric bypass (LRYGB, 24.3%), laparoscopic sleeve gastrectomy (LSG, 19.5%), and laparoscopic mini gastric bypass (15.4%).
- ↑ Stylopoulos N, Hoppin AG, Kaplan LM (October 2009). "Roux-en-Y gastric bypass enhances energy expenditure and extends lifespan in diet-induced obese rats". Obesity (Journal Article). The Obesity Society (published 6 September 2012). 17 (10): 1839–47. doi:10.1038/oby.2009.207. eISSN 1930-739X. PMC 4157127. PMID 19556976.
Despite its widespread clinical use, the mechanisms by which RYGB induces its profound weight loss remain largely unknown. This procedure effects weight loss by altering the physiology of weight regulation and eating behavior rather than by simple mechanical restriction and/or malabsorption as previously thought.
- ↑ Cho M, Pinto D, Carrodeguas L, Lascano C, Soto F, Whipple O, et al. (13 April 2005). "Frequency and management of internal hernias after laparoscopic antecolic antegastric Roux-en-Y gastric bypass without division of the small bowel mesentery or closure of mesenteric defects: review of 1400 consecutive cases". Surgery for Obesity and Related Diseases (Journal Article). Elsevier (published 7 March 2006). 2 (2): 87–91. doi:10.1016/j.soard.2005.11.004. eISSN 1878-7533. OCLC 723554412. PMID 16925328. Retrieved 5 October 2019.
Three patients (0.2%) developed a symptomatic internal hernia. Two of these patients had a 200—cm—long Roux limb, and the other had a 100—cm—long Roux limb. All three patients exhibited mild symptoms of partial small bowel obstruction. In all three cases the internal hernia was clinically manifested more than 10 months after the original AA—LRYGBP.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Sacks BC, Mattar SG, Qureshi FG, Eid GM, Collins JL, Barinas-Mitchell EJ, et al. (2006). "Incidence of marginal ulcers and the use of absorbable anastomotic sutures in laparoscopic Roux-en-Y gastric bypass". Surgery for Obesity and Related Diseases (Journal Article). Elsevier. 2 (1): 11–6. doi:10.1016/j.soard.2005.10.013. eISSN 1878-7533. OCLC 723554412. PMID 16925306.
Marginal ulceration is a known complication of both open and laparoscopic Roux-en-Y gastric bypass, with an incidence of approximately 1% to 16%; most recent studies cite an incidence of approximately 2%. Although relatively uncommon, these ulcers cause significant morbidity, including severe pain, bleeding, and dysphagia, which may result in multiple readmissions.
{{cite journal}}: CS1 maint: url-status (link) - ↑ John S, Hoegerl C (November 2009). "Nutritional deficiencies after gastric bypass surgery". The Journal of the American Osteopathic Association (Journal Article). American Osteopathic Association (published 1 November 2009). 109 (11): 601–4. doi:10.7556/jaoa.2009.109.11.601 (inactive 31 October 2021). eISSN 1945-1997. LCCN 90641783. OCLC 1081714. PMID 19948694.
Nutritional deficiencies are unrecognized in approximately 50% of patients who undergo gastric bypass surgery. The authors present some of the more common nutritional deficiencies and related complications that can occur in this patient population.
{{cite journal}}: CS1 maint: DOI inactive as of October 2021 (link) - 1 2 Poitou Bernert C, Ciangura C, Coupaye M, Czernichow S, Bouillot JL, Basdevant A (February 2007). "Nutritional deficiency after gastric bypass: diagnosis, prevention and treatment". Diabetes & Metabolism (Journal Article) (in English and French). French Society for the study of Diabetes (published 6 March 2007). 33 (1): 13–24. doi:10.1016/j.diabet.2006.11.004. eISSN 1878-1780. OCLC 715912772. PMID 17258928.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Madan AK, Orth WS, Tichansky DS, Ternovits CA (May 2006). "Vitamin and trace mineral levels after laparoscopic gastric bypass". Obesity Surgery. Springer-Verlag (published 1 May 2006). 16 (5): 603–6. doi:10.1381/096089206776945057. eISSN 1708-0428. LCCN 2001301458. OCLC 23835796. PMID 16687029. S2CID 31410788.
Nutritional deficiencies are a concern after any bariatric surgery procedure. Restriction of oral intake and/or decreased absorption may cause vitamin abnormalities. Prevention of these vitamin deficiencies includes both supplementation and routine measuring of serum values.
- ↑ Paluszkiewicz R, Kalinowski P, Wróblewski T, Bartoszewicz Z, Białobrzeska-Paluszkiewicz J, Ziarkiewicz-Wróblewska B, et al. (December 2012). "Prospective randomized clinical trial of laparoscopic sleeve gastrectomy versus open Roux-en-Y gastric bypass for the management of patients with morbid obesity". Wideochirurgia I Inne Techniki Maloinwazyjne = Videosurgery and Other Miniinvasive Techniques (Journal Article). Termedia Publishing (published 20 December 2012). 7 (4): 225–32. doi:10.5114/wiitm.2012.32384. eISSN 2299-0054. OCLC 761331890. PMC 3557743. PMID 23362420.
Vitamin and mineral supplementation was prescribed to both RYGB and LSG patients in a uniform manner to avoid confounding factors related to differences in nutrient supplementation. Postoperatively, one tablet of multivitamin and mineral supplements and sublingual iron at a dose of 0.1 g daily were prescribed. Vitamin B12 supplementation was given sublingually every month at a dose of 1000 µg.
- ↑ Adams TD, Avelar E, Cloward T, Crosby RD, Farney RJ, Gress R, et al. (October 2005). "Design and rationale of the Utah obesity study. A study to assess morbidity following gastric bypass surgery". Contemporary Clinical Trials (Journal Article). Elsevier (published 1 October 2005). 26 (5): 534–51. doi:10.1016/j.cct.2005.05.003. eISSN 1559-2030. LCCN 80645055. OCLC 569090329. PMID 16046191. Retrieved 4 October 2019.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Hagedorn JC, Encarnacion B, Brat GA, Morton JM (2007). "Does gastric bypass alter alcohol metabolism?". Surgery for Obesity and Related Diseases (Journal Article). Elsevier (published 1 September 2007). 3 (5): 543–8, discussion 548. doi:10.1016/j.soard.2007.07.003. eISSN 1878-7533. OCLC 723554412. PMID 17903777. Retrieved 5 October 2019.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Kushner RF, Gleason B, Shanta-Retelny V (September 2004). "Reemergence of pica following gastric bypass surgery for obesity: a new presentation of an old problem". Journal of the American Dietetic Association (Journal Article). Elsevier (published 1 September 2004). 104 (9): 1393–7. doi:10.1016/j.jada.2004.06.026. OCLC 1113369764. PMID 15354156. Retrieved 6 October 2019.
Pica, the compulsive ingestion of nonnutritive substances, has been a fascinating and poorly understood phenomenon for centuries. Pagophagia, or ice eating, is one of the most common forms of pica and is closely associated with the development of iron-deficiency anemia. Although this condition has been well described among pregnant women and malnourished children, particularly in developing countries, it has not been previously reported to occur following gastric bypass surgery for treatment of severe obesity. This article presents two cases of women who experienced a recurrence of pagophagia following gastric bypass surgery, along with an updated review of the literature.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Pories WJ, Caro JF, Flickinger EG, Meelheim HD, Swanson MS (September 1987). "The control of diabetes mellitus (NIDDM) in the morbidly obese with the Greenville Gastric Bypass". Annals of Surgery (Journal Article). Lippincott Williams & Wilkins (published 1 September 1987). 206 (3): 316–23. doi:10.1097/00000658-198709000-00009. eISSN 1528-1140. OCLC 676989143. PMC 1493167. PMID 3632094.
Abnormal glucose metabolism was present in 141 (36%) of 397 patients before surgery: NIDDM was present in 88 patients (22%) and 53 patients (14%) were glucose impaired. Of these, all but two became euglycemic within 4 months after surgery without any diabetic medication or special diets.
- ↑ Pories WJ, Swanson MS, MacDonald KG, Long SB, Morris PG, Brown BM, et al. (September 1995). "Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus". Annals of Surgery (Journal Article). Lippincott Williams & Wilkins (published 1 September 1995). 222 (3): 339–50, discussion 350–2. doi:10.1097/00000658-199509000-00011. eISSN 1528-1140. OCLC 866946233. PMC 1234815. PMID 7677463.
- ↑ Long SD, O'Brien K, MacDonald KG, Leggett-Frazier N, Swanson MS, Pories WJ, Caro JF (May 1994). "Weight loss in severely obese subjects prevents the progression of impaired glucose tolerance to type II diabetes. A longitudinal interventional study". Diabetes Care (Journal Article). American Diabetes Association. 17 (5): 372–5. doi:10.2337/diacare.17.5.372. eISSN 1935-5548. OCLC 60638990. PMID 8062602. S2CID 39466355. Retrieved 8 October 2019.
{{cite journal}}: CS1 maint: url-status (link) - ↑ Elkins G, Whitfield P, Marcus J, Symmonds R, Rodriguez J, Cook T (April 2005). "Noncompliance with behavioral recommendations following bariatric surgery". Obesity Surgery (Journal Article). Springer-Verlag (published 1 April 2005). 15 (4): 546–51. doi:10.1381/0960892053723385. eISSN 1708-0428. LCCN 2001301458. OCLC 23835796. PMID 15946436. S2CID 12924412.
- ↑ Delin CR, Watts JM, Saebel JL, Anderson PG (October 1997). "Eating behavior and the experience of hunger following gastric bypass surgery for morbid obesity". Obesity Surgery (Journal Article). Springer-Verlag (published 1 October 1997). 7 (5): 405–13. doi:10.1381/096089297765555386. eISSN 1708-0428. LCCN 2001301458. OCLC 23835796. PMID 9730494. S2CID 43501262.
News sources
- ↑ Templeton D (3 March 2010). "Magee pilot study probes further into weight-loss methods". Pittsburgh Post-Gazette. PG Publishing. ISSN 1068-624X. Retrieved 6 January 2014.
- ↑ Straumann F (29 March 2017). "Schwere Vorwürfe – Zürcher Spital trennt sich von Chirurg" [Serious allegations – Zurich hospital separates from surgeon]. Medizin & Psychologie. Tages-Anzeiger (article) (in German). Zürich, CH. Retrieved 8 September 2017.
"Eine Magenoperation kostet üblicherweise 20,000 bis 25,000 Franken inklusive Voruntersuchungen und Nachbetreuung", sagt Saps-Präsident Heinrich von Grünigen.
Press releases
- ↑ "Complications and Costs for Obesity Surgery Declining" (Press release). Rockville, MD: Agency for Healthcare Research and Quality. 29 April 2009. Archived from the original on 18 August 2011. Retrieved 24 August 2011.
The study, "Recent Improvements in Bariatric Surgery Outcomes," to be published in the May 2009 Medical Care, found that the complication rate among patients initially hospitalized for bariatric surgery dropped from approximately 24 percent to roughly 15 percent.
Web sources
- ↑ Dansinger M (18 February 2019). "Weight Loss and Body Mass Index (BMI)". WebMD.com. WebMD, LLC. Retrieved 5 October 2019.
- ↑ "Story of Obesity Surgery". asmbs.org. American Society for Metabolic and Bariatric Surgery. 1 January 2004. Retrieved 18 March 2016.
- ↑ "Know the possible risks of bariatric surgery". munroeregional.com. Ocala, Florida: Munroe Regional Medical Center. Archived from the original on 18 December 2013. Retrieved 6 January 2014 – via archive.org.
Bariatric surgery is major surgery. Any major surgery involves the potential for complications—adverse events which increase risk, hospital stay, and mortality. Some complications are common to all abdominal operations, while some are specific to bariatric surgery. A person who chooses to undergo bariatric surgery should know about these risks.
- ↑ Mandal A (24 April 2019). Robertson S (ed.). "Gastric Bypass Complications". news-medical.net. AZoNetwork.
Like most other surgeries, gastric bypass surgery is associated with a degree of risk. The surgery is associated with various complications, some of which are more serious than others such as internal bleeding or blood clots.
- ↑ Quinlan JA (5 March 2019). "Gastric Bypass Surgery Cost – As Low as $0, But Average Is $3,500". bariatric-surgery-source.com. Bariatric Surgery Source. Retrieved 7 October 2019.
The average cost of gastric bypass surgery is $24,300. That drops to around $3,500 with insurance but could be as low as $0 depending on your specific insurance pan and how much of your deductible and out-of-pocket maximum you’ve already paid this year.
- ↑ Bittner P (6 July 2011). "Der Mann, der die Pfunde purzeln lässt: Dr. Thomas Horbach operiert in Schwabach stark übergewichtige Menschen" [The man who lets the pounds tumble: Dr. Thomas Horbach operates in Schwabach heavily overweight people]. nordbayern.de (in German). Verlag Nürnberger Presse. Retrieved 8 September 2017.
- ↑ "Surgical Review Corporation". surgicalreview.org/. Raleigh, North Carolina: Surgical Review Corporation. Retrieved 7 October 2019.
Surgical Review Corporation provides accreditation, consulting, education, and data for surgeons and facilities to advance the safety and quality of care for their patients.
- ↑ "Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program". facs.org. Chicago, Illinois: American College of Surgeons.
The American College of Surgeons (ACS) and the American Society for Metabolic and Bariatric Surgery (ASMBS) combined their respective national bariatric surgery accreditation programs into a single unified program to achieve one national accreditation standard for bariatric surgery centers, the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBSAQIP®).
- ↑ "IFSO Chapters: International Federation for the Surgery of Obesity and Metabolic Disorders". ifso.com. Naples, Italy: International Federation for the Surgery of Obesity and Metabolic Disorders.
IFSO Regional chapters represent Adhering and Affiliated bodies of IFSO and Individual members from a defined geographical region
Further reading
- Buchwald H, Cowan GS, Pories WJ (13 October 2006). Surgical Management of Obesity (1st ed.). Saunders. doi:10.1016/B978-1-4160-0089-1.X5001-8. ISBN 978-1416000891. LCCN 2006041808. OCLC 954791137. OL 17156851M.
- Buchwald H (April 2005). "Bariatric surgery for morbid obesity: health implications for patients, health professionals, and third-party payers". Journal of the American College of Surgeons (Journal Article) (published 1 April 2004). 200 (4): 593–604. doi:10.1016/j.jamcollsurg.2004.10.039. OCLC 813726901. PMID 15804474.
- Christou NV, Sampalis JS, Liberman M, Look D, Auger S, McLean AP, MacLean LD (September 2004). "Surgery decreases long-term mortality, morbidity, and health care use in morbidly obese patients". Annals of Surgery (Journal Article). Lippincott Williams & Wilkins. 240 (3): 416–23, discussion 423–4. doi:10.1097/01.sla.0000137343.63376.19. eISSN 1528-1140. PMC 1356432. PMID 15319713.
- Fontaine KR, Redden DT, Wang C, Westfall AO, Allison DB (January 2003). "Years of life lost due to obesity". JAMA (Journal Article) (published 8 January 2003). 289 (2): 187–93. doi:10.1001/jama.289.2.187. eISSN 1538-3598. LCCN 82643544. OCLC 1124917. PMID 12517229.
- Peeters A, Barendregt JJ, Willekens F, Mackenbach JP, Al Mamun A, Bonneux L (January 2003). NEDCOM, the Netherlands Epidemiology and Demography Compression of Morbidity Research Group. "Obesity in adulthood and its consequences for life expectancy: a life-table analysis" (PDF). Annals of Internal Medicine (Journal Article). American College of Physicians (published 1 January 2003). 138 (1): 24–32. doi:10.7326/0003-4819-138-1-200301070-00008. eISSN 1539-3704. hdl:1765/10043. LCCN 43032966. OCLC 1481385. PMID 12513041. S2CID 8120329.
- Hutter MM, Randall S, Khuri SF, Henderson WG, Abbott WM, Warshaw AL (May 2006). "Laparoscopic versus open gastric bypass for morbid obesity: a multicenter, prospective, risk-adjusted analysis from the National Surgical Quality Improvement Program". Annals of Surgery (Journal Article). Lippincott Williams & Wilkins (published 1 May 2006). 243 (5): 657–62, discussion 662–6. doi:10.1097/01.sla.0000216784.05951.0b. eISSN 1528-1140. PMC 1570562. PMID 16633001.
External links
| Wikimedia Commons has media related to Gastric bypass surgery. |