Scimitar syndrome
| Scimitar syndrome | |
|---|---|
 | |
| Scimitar syndrome chest CT | |
Scimitar syndrome, or congenital pulmonary venolobar syndrome, is a rare congenital heart defect characterized by anomalous venous return from the right lung (to the systemic venous drainage, rather than directly to the left atrium).[1] This anomalous pulmonary venous return can be either partial (PAPVR) or total (TAPVR). The syndrome associated with PAPVR is more commonly known as Scimitar syndrome after the curvilinear pattern created on a chest radiograph by the pulmonary veins that drain to the inferior vena cava.[2] This radiographic density often has the shape of a scimitar, a type of curved sword.[2] The syndrome was first described by Catherine Neill in 1960.[3]
Signs and symptoms
The anomalous venous return forms a curved shadow on chest x-ray such that it resembles a scimitar. This is called the Scimitar Sign. Associated abnormalities include right lung hypoplasia with associated dextroposition of the heart, pulmonary artery hypoplasia and pulmonary sequestration. Incidence is around 1 per 100,000 births.[4]
Cause
The etiology of Scimitar syndrome is not known[5]
Diagnosis
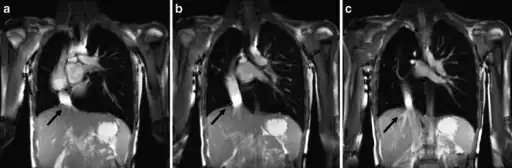 a-c) Scimitar syndrome in a young male- Breath-hold coronal 2-D steady-state free precession demonstrates the anomalous partial pulmonary venous return
a-c) Scimitar syndrome in a young male- Breath-hold coronal 2-D steady-state free precession demonstrates the anomalous partial pulmonary venous return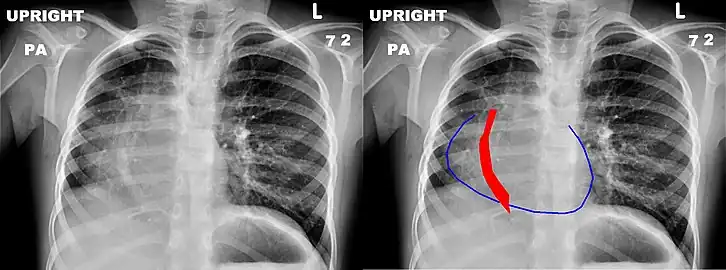 Chest x-ray of a five-year-old girl with Scimitar syndrome. The heart (blue outline) is shifted into the right half of the chest, and the anomalous pulmonary venous return (red) has a shape reminiscent of a Scimitar.
Chest x-ray of a five-year-old girl with Scimitar syndrome. The heart (blue outline) is shifted into the right half of the chest, and the anomalous pulmonary venous return (red) has a shape reminiscent of a Scimitar.
The diagnosis is made by transthoracic or transesophageal echocardiography and selective pulmonary angiography.[6] More recently by CT angiography or MR Angiography.
Pulmonary angiography demonstrates anomalous arterial supply to right lower lobe.[6]
Treatment
Surgical correction should be considered in the presence of significant left to right shunting (Qp:Qs ≥ 2:1) and pulmonary hypertension. This involves creation of an inter-atrial baffle to redirect the pulmonary venous return into the left atrium. Alternatively, the anomalous vein can be re-implanted directly into the left atrium.
History
Scimitar syndrome was first described by George Cooper and Raoul Chassinat in 1836 regarding a rare syndrome that has an abnormal pulmonary vein that drains into inferior vena cava below the diaphgram instead of draining into the left atrium.[7]
References
- ↑ Sehgal, Arvind; Loughran-Fowlds, Allison, Clinical Brief: Scimitar Syndrome (PDF), medIND — Biomedical journals from India, archived from the original (PDF) on 2009-05-30, retrieved 2008-02-28
- 1 2 Scimitar Syndrome, Children's Hospital Boston, archived from the original on 2010-12-04, retrieved 2008-02-28
- ↑ Oransky, Ivan (2006). "Catherine Neill" (PDF). The Lancet. 367 (9519): 1312. doi:10.1016/s0140-6736(06)68565-6. Archived (PDF) from the original on 2019-12-21. Retrieved 2022-06-19.
- ↑ M.Hasan, A.Varshney. A case of scimitar syndrome: anesthetic considerations regarding non cardiac surgery. Pediatric Anesthesia and Critical Care Journal 2016;4(2):89-90 doi:10.14587/paccj.2016.18 .
- ↑ Diaz-Frias, Josue; Widrich, Jason (2022). "Scimitar Syndrome". StatPearls. StatPearls Publishing. Archived from the original on 15 August 2022. Retrieved 20 October 2022.
- 1 2 Roehm, John O. F.; Jue, Kenneth L.; Amplatz, Kurt (May 1966). "Radiographic Features of the Scimitar Syndrome". Radiology. 86 (5): 856–859. doi:10.1148/86.5.856. ISSN 0033-8419. Archived from the original on 2022-06-14. Retrieved 2022-06-19.
- ↑ Mulligan, Michael E. (January 1999). "History of Scimitar Syndrome". Radiology. 210 (1): 288–290. doi:10.1148/radiology.210.1.r99ja59288. ISSN 0033-8419. Archived from the original on 2022-10-21. Retrieved 2022-06-19.
Further reading
- Holt, PD; Berdon, WE; Marans, Z; Griffiths, S; Hsu, D (February 2004). "Scimitar vein draining to the left atrium and a historical review of the scimitar syndrome". Pediatric Radiology. 34 (5): 409–13. doi:10.1007/s00247-004-1149-0. PMID 14872299.
- A case of Scimitar Syndrome Archived 2016-03-03 at the Wayback Machine
- Halasz NA, Halloran KH, Liebow AA (November 1956). "Bronchial and arterial anomalies with drainage of the right lung into the inferior vena cava". Circulation. 14 (5): 826–46. doi:10.1161/01.cir.14.5.826. PMID 13374858. Archived from the original on 2013-02-23. Retrieved 2022-06-19.
- Kramer U, Dörnberger V, Fenchel M, Stauder N, Claussen CD, Miller S (December 2003). "Scimitar syndrome: morphological diagnosis and assessment of hemodynamic significance by magnetic resonance imaging". Eur Radiol. 13 (Suppl 4): L147–50. doi:10.1007/s00330-003-2061-y. PMID 15018181.
- Brown JW, Ruzmetov M, Minnich DJ, et al. (February 2003). "Surgical management of scimitar syndrome: an alternative approach". J. Thorac. Cardiovasc. Surg. 125 (2): 238–45. doi:10.1067/mtc.2003.113. PMID 12579091.
- Hasan M, Varshney A, Agarwal P (2016). "A case of scimitar syndrome: anesthetic considerations regarding non cardiac surgery" (PDF). Pediatric Anesthesia and Critical Care Journal. 4 (2): 89–90. Archived (PDF) from the original on 2017-04-21. Retrieved 2022-06-19.
External links
| Classification |
|---|