Vaginoplasty
| Vaginoplasty | |
|---|---|
 Vaginoplasty and labiaplasty example, shown pre- and post-op. The vaginoplasty has reduced the size of the vaginal opening. | |
| ICD-9-CM | 70.64, 70.62, 70.64, 70.94, 70.6, 70.95 |
| MeSH | D013509 |
Vaginoplasty is any surgical procedure that results in the construction or reconstruction of the vagina. It is a type of genitoplasty. Pelvic organ prolapse is often treated with one or more surgeries to repair the vagina. Sometimes a vaginoplasty is needed following the treatment or removal of malignant growths or abscesses in order to restore a normal vaginal structure and function. Surgery to the vagina is done to correct congenital defects to the vagina, urethra and rectum. It will correct protrusion of the urinary bladder into the vagina (cystocele) and protrusion of the rectum (rectocele) into the vagina.[1] Often, a vaginoplasty is performed to repair the vagina and its attached structures due to trauma or injury. Labiaplasty, which alters the appearance of the vulva, can be performed as a discrete surgery, or as a subordinate procedure within a vaginoplasty.[2][3]
Congenital disorders such as adrenal hyperplasia can affect the structure and function of the vagina and sometimes the vagina is absent; these can be reconstructed or formed, using a vaginoplasty.[4] Other candidates for the surgery include babies born with a microphallus, people with Müllerian agenesis resulting in vaginal hypoplasia, trans women, and women who have had a vaginectomy after malignancy or trauma.[5][6] Vaginoplasty can reduce the size of the entrance of the vagina or alter the appearance of the vulva.
Medical uses
Vaginoplasty is the description of the following surgical interventions:
- separation of congenitally fused urethra and vagina[7]
- repair of a urethra that is short[7]
- vaginal construction[5][8]
- vaginal reconstruction[5][8]
- vaginal vault prolapse[9]
- vaginal suspension and fixation[5][8]
- operations on cul-de-sac[5][8]
- repair of cystocele[5][8]and rectocele[5]
- retropubic paravaginal repair[10]
- the repair of a cystocele using a graft or prosthesis[5][8]
- the repair of a cystocele and a rectocele in the same procedure using a graft or prosthetic device[5][8]
- the repair of a rectocele using a graft or prosthetic material[5]
- the vaginal construction using a graft or prosthetic material[5][11]
- the vaginal reconstruction using a graft or prosthetic material[5]
- the vaginal suspension and stabilization using with graft or prosthetic material
- treatment of MRKH syndrome (vaginal agenesis)[11]
- hymenorrhaphy
In some instances, extra tissue is needed to reconstruct or construct the vagina. These grafts used in vaginoplasty can be an allogenic, a heterograph, an autograft, xenograft, or an autologous material.[11][12] A woman can use an autologous in vitro cultured tissue taken from her vaginal vestibule as transplanted tissue to form the lining of the reconstructed vagina.[11] A reconstructed or newly constructed vagina is called a neovagina.[13]
Vaginoplasties in children
Conditions such as congenital adrenal hyperplasia virilize genetic females due to a 21-hydroxylase deficiency. Specific procedures include: clitoral reduction, labiaplasty, normalizing appearance, vagina creation, initiating vaginal dilation.[14] Vaginal atresia, or congenital absence of the vagina can be another reason for surgery to construct a normal and functional vagina.[15] Vaginoplasty is used as part of the series of surgeries needed to treat those girls and women born with the bladder located outside of their abdomen. After the repairs, women have been able to give birth but are at risk of prolapse.[1]
There are human rights concerns about vaginoplasties and other genital surgeries in children who are not old enough to consent,[16][17] including concern with post-surgical sexual function,[18] and assumptions of cisnormativity.[19] There is no consensus attitude amongst clinicians about their necessity, timing, method or evaluation.[14] Vaginoplasties may be performed in children or adolescents with intersex conditions or disorders of sex development.[20]
Techniques
Non-surgical vagina creation was used in the past to treat the congenital absence of a vagina. The procedure involved the wearing of a saddle-like device and the use of increasing-diameter dilators. The procedure took several months and was sometimes painful. It was not effective in every instance.[4] Uncommon growths, cysts, septums in the vagina can also require vaginoplasty.[3]
Reconstructive surgery after cancer treatment
Radiological cancer treatment can result in the destruction or alteration of vaginal tissues. Vaginoplasty is often performed to reconstruct the vagina and other genital structures. In some cases, normal sexual function can be restored.[5]
McIndoe surgical technique
A canal is surgically constructed between the urinary bladder and urethra in the anterior portion of the pelvic region and the rectum. A skin graft is used from another area of the person's body. The graft is removed from the thigh, buttocks, or inguinal region. Other materials have been used to create the lining of the new vagina. These have been cutaneous skin flaps, amniotic membranes, and buccal mucosa.[5][11]
Sex reassignment surgery
Several techniques may be used in sex reassignment surgery to create a vagina.


Penile inversion
Inversion of the penile skin is the method most often selected to create a neovagina by surgeons performing sex reassignment surgery. The inverted penile skin uses inferior pedicle skin or abdominal skin for the lining of the neovagina. The skin is cut to form an appropriate-sized flap. The skin flap is sometimes combined with a scrotal or urethral flap.[6]
The penile inversion technique was pioneered by Georges Burou in his Morocco clinic in the 1950s.[21] By the 1970s he had performed hundreds of them, and gave his first public presentation of his technique to a conference at Stanford University in 1973,[22] after which it gradually became the predominant technique worldwide.
Bowel vaginoplasty
Bowel vaginoplasty is another commonly used method to create a neovagina in sex reassignment surgery.[6] It is generally used in those with penoscrotal hypoplasia or those for whom a primary penile inversion vaginoplasty failed.
Compared to penile inversion, bowel vaginoplasty has the advantages of self-lubrication, depth, and reduced risk of stenosis. However, it carries the disadvantages of requiring abdominal surgery and the creation of a bowel anastomosis, excessive discharge and/or malodour, and prolapsed neovagina. Patients with a history of cancer, inflammatory bowel disease, or extensive intraabdominal adhesions are not candidates for this procedure.
Other methods
Penile-scrotal skin flaps are also used. Nongenital full-thickness graft (FTG) or split-thickness skin grafts from other parts of the body have been used.
The World Professional Association for Transgender Health
The World Professional Association for Transgender Health (WPATH) criteria for genital ("bottom") surgery (orchiectomy and vaginoplasty in male-to-female transgender individuals) include:[23]
- Two referral letters from qualified mental health professionals.
- Persistent, well-documented gender dysphoria.
- Capacity for informed decision making and consent.
- Age of majority.
- Well-controlled medical and mental health comorbidities.
- Twelve continuous months of hormone therapy, unless the individual is unwilling or unable secondary to a medical condition (recommended for orchiectomy and vaginoplasty).
- Twelve continuous months of living in the desired gender role congruent with the individual's gender identity (recommended for vaginoplasty).
- Regular visits with a mental health or other medical professional are also recommended but not explicitly required for surgery.
Elective vaginoplasty
Critics have labeled such surgery as the "designer vagina". The American College of Obstetricians and Gynecologists issued a warning against these procedures in 2007[24] as did the Royal Australian College of Gynaecologists,[25] and a commentary in the British Medical Journal strongly criticized the "designer vagina" in 2009.[25][26] The Society of Obstetricians and Gynaecologists of Canada published a policy statement against elective vaginoplasty based upon the risks associated with unnecessary cosmetic surgery in 2013.[27]
The World Health Organization describes any medically unnecessary surgery to the vaginal tissue and organs as female genital mutilation.[28]
Vaginal rejuvenation is a form of elective plastic surgery. Its purpose is to restore or enhance the vagina's cosmetic appearance.[26]
Hymen surgical procedures
An imperforate hymen is the presence of tissue that completely covers the vaginal opening. It is cut to allow menstrual flow to exit during a short surgical procedure.[1] A hymenorrhaphy is the surgical procedure that reconstructs the hymen.
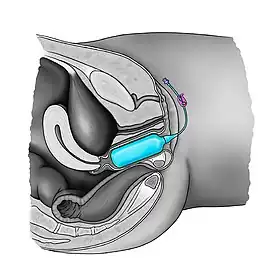
Balloon vaginoplasty
In this procedure, a Foley catheter is laparoscopically inserted to the rectouterine pouch whereupon gradual traction and distension are applied to create a neovagina.
Pull through or Vecchietti procedure
In treating Müllerian agenesis, the Vecchietti procedure is a laparoscopic surgical technique that produces a vagina of dimensions (depth and width) comparable to those of a normal vagina (ca. 8.0 cm. deep).[29][30] A small, plastic sphere (“olive”) is threaded (sutured) against the vaginal area; the threads are drawn though the vaginal skin, up through the abdomen, and through the navel. There, the threads are attached to a traction device, and then daily are drawn tight so that the “olive” is pulled inwards and stretches the vagina, by approximately 1.0 cm. per day, thereby creating a vagina, approximately 7.0 cm. deep by 7.0 cm. wide, in 7 days. The mean operating room (OR) time for the Vecchietti vaginoplasty is approximately 45 minutes; yet, depending upon the patient and her indications, the procedure might require more time.[31] The outcomes of Vecchietti technique via the laparoscopic approach are found to be comparable to the procedure using laparotomy.[32] In vaginal hypoplasia, traction vaginoplasty such as the Vecchietti technique seems to have the highest success rates both anatomically (99%) and functionally (96%) among available treatments.[33][3]
Other surgical techniques that have been developed include ileal neovagina (Monti's technique), the Creatsas vaginoplasty, the Wharton–Sheares–George neovaginoplasty, or the Davydov procedure. The most widely used is the Vecchietti laparoscopic procedure. Sometimes sexual intercourse can result in the dilation of a newly constructed vagina.[11]
Vaginal dilators and expanders

The most techniques of vaginoplasty are using inflatable vaginal expanders or vaginal stents to design the vaginal diameter and length.[34][35] At the end of the procedure the device stays in place to maintain the neovagina against the pelvic wall which also favors the process of microscopic neovascularization and reduces the risks of hematoma. In post-operative setting the expander can be used regularly to prevent post-operative vaginal retraction.[36] Solid vaginal dilators can also be used immediately after surgery to keep the passage from attachments, and regularly thereafter to maintain the viability of the neovagina. The frequency required to use decreases over time, however remains obligatory lifelong.[37][38]
Risks and complications
Reconstructive vaginoplasty in children and adolescents carries the risk of "superinfection".[3]
In adults, rates and types of complications varied with sex reassignment vaginoplasty. Necrosis of the clitoral region was 1-3%. Necrosis of the surgically created vagina was 3.7-4.2%. Vaginal shrinkage occurred was documented in 2-10% of those treated. Stricture, or narrowing of the vaginal orifice was reported in 12-15% of the cases. Of those reporting stricture, 41% underwent a second operation to correct the condition. Necrosis of two scrotal flaps has been described. Posterior vaginal wall is rare complication. Genital pain was reported in 4-9%. Rectovaginal fistula is also rare with only 1% documented. Vaginal prolapse was seen in 1-2% of people assigned male at birth undergoing this procedure.[6]
The ability of emptying the bladder was affected after this procedure with 13% reporting improvement, 68% said that there was no change and 19% reported that voiding got worse. Those reporting a negative outcome experienced in which loss of bladder control and urinary incontinence were 19%. Urinary tract infections occurred in 32% of those treated.[6]
See also
- Intersex medical interventions
- Sex reassignment surgery (male-to-female)
- List of transgender-related topics
- Enterocele
- Sigmoidocele
References
- 1 2 3 Baggish, p. 779-798.
- ↑ Mirzabeigi MN, Moore JH, Mericli AF, et al. (February 2012). "Current trends in vaginal labioplasty: a survey of plastic surgeons". Ann Plast Surg. 68 (2): 125–34. doi:10.1097/SAP.0b013e31820d6867. PMID 21346521. S2CID 36163955.
- 1 2 3 4 Emans.
- 1 2 Gundeti, Mohan (2012). Pediatric Robotic and Reconstructive Urology a Comprehensive Guide. City: Wiley-Blackwell. ISBN 9781444335538; Access provided by the University of Pittsburgh
{{cite book}}: CS1 maint: postscript (link) - 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Hoffman, Barbara (2012). Williams gynecology. New York: McGraw-Hill Medical. ISBN 9780071716727.
- 1 2 3 4 5 Horbach, Sophie E.R.; Bouman, Mark-Bram; Smit, Jan Maerten; Özer, Müjde; Buncamper, Marlon E.; Mullender, Margriet G. (2015). "Outcome of Vaginoplasty in Male-to-Female Transgenders: A Systematic Review of Surgical Techniques". The Journal of Sexual Medicine. 12 (6): 1499–1512. doi:10.1111/jsm.12868. ISSN 1743-6095. PMID 25817066.
- 1 2 Hiort, O (2014). Understanding differences and disorders of sex development (DSD). Basel: Karger. ISBN 9783318025590; Access provided by the University of Pittsburgh
{{cite book}}: CS1 maint: postscript (link) - 1 2 3 4 5 6 7 "2016 ICD-10-PCS Procedure Code 0UQG0ZZ : Repair Vagina, Open Approach". ICD10Data.com. Retrieved 2016-03-03.
- ↑ Baggish, p. 467-474.
- ↑ Baggish, p. 409-412.
- 1 2 3 4 5 6 Acién, Pedro; Acién, Maribel (2016-01-01). "The presentation and management of complex female genital malformations". Human Reproduction Update. 22 (1): 48–69. doi:10.1093/humupd/dmv048. ISSN 1355-4786. PMID 26537987.
- ↑ "Online ICD9/ICD9CM codes". World Health Organization. Retrieved 2016-03-01.
- ↑ Unger, Cecile A.; Paraiso, Marie Fidela R. (16 October 2014). "18. Construction of the Neovagina". In Farzeen Firoozi (ed.). Female Pelvic Surgery. New York: Springer. pp. 267–. ISBN 978-1-4939-1504-0. OCLC 941369411. Retrieved 31 May 2018.
- 1 2 Lee PA, Nordenström A, Houk CP, Ahmed SF, Auchus R, Baratz A, et al. (2016). "Global Disorders of Sex Development Update since 2006: Perceptions, Approach and Care". Horm Res Paediatr. 85 (3): 158–80. doi:10.1159/000442975. ISSN 1663-2818. PMID 26820577.
- ↑ "Müllerian Agenesis: Diagnosis, Management, and Treatment - ACOG". www.acog.org. Retrieved 2017-12-26.
- ↑ Office of the High Commissioner for Human Rights (October 24, 2016), End violence and harmful medical practices on intersex children and adults, UN and regional experts urge
- ↑ "The Social Construction of Female Circumcision: Gender, Equality, and Culture". femalecircumcision. 2018-02-02. Retrieved 2018-02-11.
- ↑ Liao LM, Wood D, Creighton SM (September 2015). "Parental choice on normalising cosmetic genital surgery". BMJ. 351: h5124. doi:10.1136/bmj.h5124. ISSN 1756-1833. PMID 26416098. S2CID 20580500.
- ↑ Report of the UN Special Rapporteur on Torture, Office of the UN High Commissioner for Human Rights, February 2013.
- ↑ Lee, P. A.; Houk, C. P.; Ahmed, S. F.; Hughes, I. A. (2006). "Consensus statement on management of intersex disorders". Pediatrics. 118 (2): e488–500. doi:10.1542/peds.2006-0738. PMC 2082839. PMID 16882788.
- ↑ Hage, J Joris; Karim, Refaat B.; Laub, Donald R. Sr (December 2007). "On the Origin of Pedicled Skin Inversion Vaginoplasty: Life and Work of Dr Georges Burou of Casablanca". Annals of Plastic Surgery. Wolters Kluwer. 59 (6): 723–729. doi:10.1097/01.sap.0000258974.41516.bc. ISSN 0148-7043. PMID 18046160. S2CID 25373951.
In 1956, the gynecologist Dr Georges Burou (1910–1987) independently developed the anteriorly pedicled penile skin flap inversion vaginoplasty in his Clinique du Parc in Casablanca. This technique was to become the gold standard of skin-lined vaginoplasty in transsexuals.
- ↑ Goddard, Jonathan Charles; Vickery, Richard M.; Terry, Tim R. (2007). "Development of Feminizing Genitoplasty for Gender Dysphoria". The Journal of Sexual Medicine. 4 (4, Part 1): 981–989. doi:10.1111/j.1743-6109.2007.00480.x. ISSN 1743-6095. PMID 17451484.
- ↑ Coleman, Eli (2017), "Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People" (PDF), Principles of Gender-Specific Medicine, Elsevier, pp. 69–75, doi:10.1016/b978-0-12-803506-1.00058-9, ISBN 978-0-12-803506-1
- ↑ Zimmerman, Rachel (31 August 2007). "Genital Procedure Draws Warning". Wall Street Journal.
- 1 2 Bourke, Emily (2009-11-12). "Designer vagina craze worries doctors". Australian Broadcasting Corporation. Retrieved 5 March 2016.
- 1 2 Liao, Lih Mei; Sarah M Creighton (24 May 2007). "Requests for cosmetic genitoplasty: how should healthcare providers respond?". BMJ. British Medical Journal. 334 (7603): 1090–1092. doi:10.1136/bmj.39206.422269.BE. PMC 1877941. PMID 17525451.
- ↑ Shaw MBChB, Dorothy; Lefebvre MD, Guylaine; Bouchard MD, Celine; Shapiro MD, MHSc, Jodi; Blake MD, Jennifer; Allen MD, Lisa; Cassell MD, Krista (December 2013). "Female Genital Cosmetic Surgery" (PDF). Journal of Obstetrics and Gynaecology Canada. Society of Obstetricians and Gynaecologists of Canada. 35 (12): 1108–1112. doi:10.1016/S1701-2163(15)30762-3. PMID 24405879. Retrieved 2016-03-07.
- ↑ "Female genital mutilation". World Health Organization. 2016. Retrieved 2016-03-07.
- ↑ Vecchietti G (1965). "[Creation of an artificial vagina in Rokitansky-Küster-Hauser syndrome]". Attual Ostet Ginecol (in Italian). 11 (2): 131–47. PMID 5319813.
- ↑ Fedele L, Bianchi S, Tozzi L, Borruto F, Vignali M (November 1996). "A new laparoscopic procedure for creation of a neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome". Fertil. Steril. 66 (5): 854–7. doi:10.1016/S0015-0282(16)58653-1. PMID 8893702.
- ↑ Fedele, Luigi; Bianchi, Stefano; Zanconato, Giovanni; Raffaelli, Ricciarda; Zatti, Nicoletta (March 2000). "Laparoscopic creation of a neovagina in a woman with a kidney transplant: Case Report". Human Reproduction. 15 (3): 692–693. doi:10.1093/humrep/15.3.692. PMID 10686221. Retrieved 28 May 2018.
- ↑ Borruto, F; Chasen, ST; Chervenak, FA; Fedele, L (Feb 1999). "The Vecchietti procedure for surgical treatment of vaginal agenesis: comparison of laparoscopy and laparotomy". International Journal of Gynaecology and Obstetrics. 64 (2): 153–8. doi:10.1016/s0020-7292(98)00244-6. PMID 10189024. S2CID 2851401.
- ↑ Callens, N.; De Cuypere, G.; De Sutter, P.; Monstrey, S.; Weyers, S.; Hoebeke, P.; Cools, M. (2014). "An update on surgical and non-surgical treatments for vaginal hypoplasia". Human Reproduction Update. 20 (5): 775–801. doi:10.1093/humupd/dmu024. ISSN 1355-4786. PMID 24899229.
- ↑ Coskun, Ayhan; Coban, Yusuf Kenan; Vardar, Mehmet Ali; Dalay, Ahmet Cemil (10 July 2007). "The use of a silicone-coated acrylic vaginal stent in McIndoe vaginoplasty and review of the literature concerning silicone-based vaginal stents: a case report". BMC Surgery. 7 (1): 13. doi:10.1186/1471-2482-7-13. PMC 1947946. PMID 17623058.
- ↑ Barutçu, Ali; Akgüner, Muharrem (November 1998). "McIndoe Vaginoplasty with the Inflatable Vaginal Stent". Annals of Plastic Surgery. 41 (5): 568–9. doi:10.1097/00000637-199811000-00020. PMID 9827964.
- ↑ Antoniadis, N; Charles, G; Mejías, I; Pabón, R (March 2011). "Vaginoplasty: modification to McIndoe techique using hemostatic gel sponge". Cirugía Plástica Ibero-Latinoamericana. 37 (1): 73–77. doi:10.4321/S0376-78922011000100010.
- ↑ The encyclopedia of cosmetic and plastic surgery. New York: Facts On File. 12 May 2010. p. 195. ISBN 978-1-4381-2702-6.
- ↑ Textbook of plastic, maxillofacial, and reconstructive surgery (2nd ed.). Baltimore, Maryland: Williams & Wilkins. 1992. ISBN 978-0-683-03454-7.
Bibliography
- Baggish, Michael (2016). Atlas of pelvic anatomy and gynecologic surgery. Philadelphia, PA: Elsevier. ISBN 9780323225526.
- Emans, Herriot (2011). Emans, Laufer, Goldstein's pediatric & adolescent gynecology. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins Health. ISBN 9781608316489.electronic book, no page numbers.