Ankle fracture
An ankle fracture is a break of one or more of the bones that make up the ankle joint.[1] Symptoms may include pain, swelling, bruising, and an inability to walk on the injured leg.[1] Complications may include an associated high ankle sprain, compartment syndrome, stiffness, malunion, and post-traumatic arthritis.[1][2]
| Ankle fracture | |
|---|---|
| Other names | Broken ankle[1] |
 | |
| Fracture of both sides of the ankle with dislocation as seen on anteroposterior X-ray. (1) fibula, (2) tibia, (arrow) medial malleolus, (arrowhead) lateral malleolus | |
| Specialty | Orthopedics |
| Symptoms | Pain, swelling, bruising, inability to walk[1] |
| Complications | High ankle sprain, compartment syndrome, decreased range of motion, malunion[1][2] |
| Usual onset | Young males, older females[2] |
| Types | Lateral malleolus, medial malleolus, posterior malleolus, bimalleolar, trimalleolar[1] |
| Causes | Rolling the ankle, blunt trauma[2] |
| Diagnostic method | X-rays based on the Ottawa ankle rule[2] |
| Differential diagnosis | Rheumatoid arthritis, gout, septic arthritis, Achilles tendon rupture[2] |
| Treatment | Splinting, casting, surgery[1] |
| Frequency | ~1 per 1000/year[2] |
Ankle fractures may result from excessive stress on the joint such as from rolling an ankle or from blunt trauma.[1][2] Types of ankle fractures include lateral malleolus, medial malleolus, posterior malleolus, bimalleolar, and trimalleolar fractures.[1] The Ottawa ankle rule can help determine the need for X-rays.[2] Special X-ray views called stress views help determine whether an ankle fracture is unstable.
Treatment depends on the fracture type. Ankle stability largely dictates non-operative vs. operative treatment. Non-operative treatment includes splinting or casting while operative treatment includes fixing the fracture with metal implants through an open reduction internal fixation (ORIF).[1] Significant recovery generally occurs within four months while completely recovery usually takes up to one year.[1]
Ankle fractures are common, occurring in over 1.8 per 1000 adults and 1 per 1000 children per year.[2][3] They occur most commonly in young males and older females.[2]
Functional anatomy
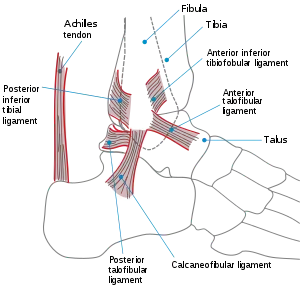
The ankle region refers to where the leg meets the foot (talocrural region).[4] The ankle joint is a highly constrained, complex hinge joint composed of three bones: the tibia, the fibula, and the talus.[5][6] The weight-bearing aspect of the tibia closest to the foot (known as the plafond) connects with the talus. This articulation (where two bones meet) is primarily responsible for plantarflexion (moving your foot down) and dorsiflexion (moving your foot up).[6] Together the tibia and fibula form a bracket-shaped socket known as the mortise, into which the dome-shaped talus fits.[7] The talus and the fibula are connected by a strong group of ligaments, which provide support for the lateral aspect of the ankle. These ligaments include the anterior talofibular ligament (ATFL) and the posterior talofibular ligament (PTFL).[8] The calcaneofibular ligament (CFL), which connects the fibula to the calcaneus, or heel bone, also provides lateral support. The deltoid ligament provides support to the medial part of the ankle (closest to the midline). It prevents the foot from excessively everting, or turning outwards while also preventing the talus from externally rotating.[8] The distal parts of the tibia and fibula are connected by a connective tissue network referred to as the syndesmosis, which consists of four ligaments and the interosseous membrane.[8]
Signs and symptoms
Symptoms of an ankle fracture can be similar to those of ankle sprains (pain, swelling, limited range of motion), though typically they are often more severe by comparison. It is exceedingly rare for the ankle joint to dislocate in the presence of ligamentous injury alone. However, in the setting of an ankle fracture, the talus can become unstable and subluxate or dislocate. Patients may notice ecchymosis ("black and blue" coloration from bleeding under the skin), or there may be an abnormal position, alignment, gross instability, or lack of normal motion secondary to pain. In a displaced, fracture the skin is sometimes tented over a sharp edge of broken bone. The sharp fragments of broken bone sometimes tear the skin and form a laceration that communicates with the broken bone or joint space. This is known as an open fracture and has a high incidence of infection if not promptly treated.[8]
Diagnosis
Physical Examination
Patients with ankle fractures may have variable findings on physical examination. Generally, the injured side should be compared to the non-injured side. The skin should be carefully examined, paying particular attention to any openings or breaks in the skin that could be due to an open fracture.[9] It is important to evaluate the exact location of the pain, the range of motion of the ankle, and the condition of the nerves and blood vessels. It is also important to palpate the calf proximally (near the knee) because there may be an associated high fibula fracture (Maisonneuve fracture).
Imaging
Imaging for evaluation of ankle fractures can include x-rays, CT scans, and MRIs. Typically evaluation begins with x-rays, which can provide information about the mechanism of injury, severity of injury, and stability of fracture. The Ottawa ankle rules determine the necessity of obtaining x-rays in patients with acute ankle injuries. These guidelines were created to minimize the expense of unnecessary x-rays.[8]
X-ray
Views
There are three x-ray views in a complete ankle series: anteroposterior (AP), lateral, and oblique (or "mortise view"). The mortise view is an AP x-ray taken with the ankle internally rotated 15-20 degrees since the foot is naturally externally rotated relative to the ankle.[8] In addition to these views, a full-length view of the tibia and fibula may be necessary to evaluate for injuries to the proximal fibula associated with Maisonneuve fractures.
A specialized AP stress view of the ankle is performed when there is concern for an unstable ankle injury. There are two types of stress views: gravity and mechanical.[10] In the gravity stress view, the patient lies in the lateral decubitus position with the ankle dangling over the edge of the table to mimic the mechanical stress view.
Findings
On X-rays, there can be a fracture of the medial malleolus, the lateral malleolus, and/or of the anterior/posterior margin of the distal tibia. The posterior margin (known as the posterior malleolus) is much more frequently injured than the anterior aspect of the distal tibia. If both the lateral and medial malleoli are broken, this is called a bimalleolar fracture (some of them are called Pott's fractures). If the posterior malleolus is also fractured, this is called a trimalleolar fracture.

 A triplane fracture of the ankle as seen on plain X-ray
A triplane fracture of the ankle as seen on plain X-ray A triplane fracture of the ankle as seen on CT
A triplane fracture of the ankle as seen on CT A triplane fracture of the ankle as seen on CT
A triplane fracture of the ankle as seen on CT
CT
CT scans may be indicated when there is concern for a highly comminuted fracture or a fracture involving the joint surface.[9] This imaging may be used for surgical planning.
MRI
MRI is less commonly used to diagnose ankle fractures but may be used to show problems involving the soft tissues (ligaments and tendons) and articular cartilage.[11]
Classification
There are several classification schemes for ankle fractures. Out of the following, the Lauge-Hansen and Danis-Weber classification systems are most commonly used.[8]
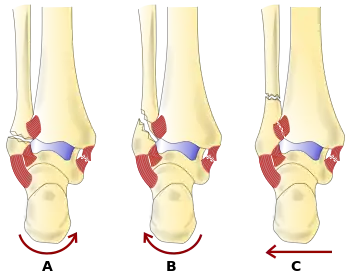
- The Lauge-Hansen classification categorizes fractures based on the mechanism of the injury as it relates to the position of the foot and the deforming force (the most common type is supination-external rotation)
- The Danis-Weber classification categorizes ankle fractures by the level of the fracture of the distal fibula (type A = below the syndesmotic ligament, type B = at its level, type C = above the ligament), with use in assessing injury to the syndesmosis and the interosseous membrane
Other classification schemes:
- The Herscovici classification categorizes medial malleolus fractures of the distal tibia based on level.
- The Ruedi-Allgower classification categorizes pilon fractures of the distal tibia.
Pediatric fracture types
- Wagstaffe-Le Fort avulsion fracture¨, a vertical fracture of the antero-medial part of the distal fibula with avulsion of the anterior tibiofibular ligament.[12]
- Tillaux fracture, a Salter–Harris type III fracture through the anterolateral aspect of the distal tibial epiphysis.[13]
- Triplane fractures are a special type of fracture that involves the immature skeleton. It has a coronal plane in the metaphysis, an axial plane in the physis, and a sagittal plane in the epiphysis.[14]

Treatment
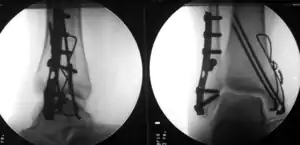
The broad goals of treating ankle fractures are restoring the ankle joint to normal alignment, healing the fracture, and preventing arthritis.[8] The stability of the ankle joint often dictates treatment. Certain fracture patterns are stable and are thus treated without surgery similarly to ankle sprains. Unstable fractures require surgery, most often an open reduction and internal fixation (ORIF), which is usually performed with permanently implanted metal hardware that holds the bones in place while the natural healing process occurs. A cast or splint will be required to immobilize the ankle following surgery.[11] Stable ankle fractures with preserved joint alignment may be treated with non-operative measures (splinting, casting, and/or walking boot).[11]
Complications
General complications associated with surgical treatment include infection, bleeding, blood clots, wound healing problems, and damage to surrounding nerves and blood vessels.[1] Specific complications associated with surgical treatment of ankle fractures include fracture healing in an abnormal position (malunion), post-traumatic arthritis, failed fracture healing after a prolonged period of time (nonunion), and decreased range of motion (post-operative stiffness).[8] If post-operative x-rays are concerning for malunion, then patients may need an additional procedure to restore proper ankle anatomy. The ultimate goal is to prevent or delay the development of post-traumatic arthritis.[8] Post-traumatic arthritis can initially be managed with conservative options like activity modification, non-steroidal anti-inflammatory medication (NSAIDs), specialized footwear, and cortisone injections.[15] If patients still have pain and impaired ankle function after these measures, then other procedures such as ankle arthrodesis and ankle arthroplasty can be considered.[16] Nonunion is rare following surgical fixation of ankle fractures but can be managed with bone grafts and stable internal fixation.[16] Patients can also experience pain or discomfort from the metal hardware used to fix the fracture. As a result, some patients decide to have the hardware removed after the fracture has healed through an additional procedure.[1]
Epidemiology
Several large studies have suggested that the incidence of ankle fractures has increased since the 1960s.[17][18][19] The incidence is highest in elderly women over the age of 65, but importantly ankle fractures are not considered as fragility fractures.[19] In terms of fracture type, isolated malleolar fractures are most common (two-thirds of fractures); bimalleolar fractures occur in roughly 25% of patients while trimalleolar fractures occur in 5-10%.[9] Open fractures are rare, compromising 2% of all ankle fractures.[20] In children, ankle fractures occur in about 1 per 1000 per year.[3]
See also
References
- "Ankle Fractures (Broken Ankle) - OrthoInfo - AAOS". www.orthoinfo.org. Retrieved 20 June 2019.
- Wire J, Slane VH (9 May 2019). "Ankle Fractures". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 31194464.
- Yeung DE, Jia X, Miller CA, Barker SL (April 2016). "Interventions for treating ankle fractures in children". The Cochrane Database of Systematic Reviews. 4: CD010836. doi:10.1002/14651858.CD010836.pub2. PMC 7111433. PMID 27033333.
- Moore KL. Clinically oriented anatomy. ISBN 978-1-9751-5086-0. OCLC 1112382966.
- Brockett CL, Chapman GJ (June 2016). "Biomechanics of the ankle". Orthopaedics and Trauma. 30 (3): 232–238. doi:10.1016/j.mporth.2016.04.015. PMC 4994968. PMID 27594929.
- Thompson CJ (2015). Netter's concise orthopaedic anatomy, updated edition. Elsevier. ISBN 978-0-323-42970-2. OCLC 946457800.
- "The Ankle Joint - Articulations - Movements - TeachMeAnatomy". Retrieved 2021-03-09.
- Coughlin MJ, Saltzman CL, Mann RA (2014). Mann's surgery of the foot and ankle. Saunders/Elsevier. ISBN 978-0-323-07242-7. OCLC 883562707.
- Koval KJ (28 March 2012). Handbook of fractures. ISBN 978-1-4511-4837-4. OCLC 1233314470.
- Murphy, Andrew. "Ankle (stress view) | Radiology Reference Article | Radiopaedia.org". Radiopaedia. Retrieved 2021-03-23.
- Carr, James B. (2009), "Malleolar Fractures and Soft Tissue Injuries of the Ankle", Skeletal Trauma, Elsevier, pp. 2515–2584, doi:10.1016/b978-1-4160-2220-6.10060-x, ISBN 978-1-4160-2220-6, retrieved 2021-03-24
- Hunter TB, Peltier LF, Lund PJ (2000). "Radiologic history exhibit. Musculoskeletal eponyms: who are those guys?" (PDF). Radiographics. 20 (3): 819–36. doi:10.1148/radiographics.20.3.g00ma20819. PMID 10835130.
- "Wheeless Online". Retrieved 30 October 2014.
- Hirsch M, et al. Understanding triplane distal tibia fractures. http://dx.doi.org/10.1016/j.rchira.2016.09.002
- Ewalefo SO, Dombrowski M, Hirase T, Rocha JL, Weaver M, Kline A, et al. (December 2018). "Management of Posttraumatic Ankle Arthritis: Literature Review". Current Reviews in Musculoskeletal Medicine. 11 (4): 546–557. doi:10.1007/s12178-018-9525-9. PMC 6220012. PMID 30327933.
- Carr JB (2009). "Malleolar Fractures and Soft Tissue Injuries of the Ankle". Skeletal Trauma. Elsevier. pp. 2515–2584. doi:10.1016/b978-1-4160-2220-6.10060-x. ISBN 978-1-4160-2220-6.
- Kannus P, Parkkari J, Niemi S, Palvanen M (December 1996). "Epidemiology of osteoporotic ankle fractures in elderly persons in Finland". Annals of Internal Medicine. 125 (12): 975–8. doi:10.7326/0003-4819-125-12-199612150-00007. PMID 8967708. S2CID 20553362.
- Daly PJ, Fitzgerald RH, Melton LJ, Ilstrup DM (October 1987). "Epidemiology of ankle fractures in Rochester, Minnesota". Acta Orthopaedica Scandinavica. 58 (5): 539–44. doi:10.3109/17453678709146395. PMID 3425285.
- Bengnér U, Johnell O, Redlund-Johnell I (February 1986). "Epidemiology of ankle fracture 1950 and 1980. Increasing incidence in elderly women". Acta Orthopaedica Scandinavica. 57 (1): 35–7. doi:10.3109/17453678608993211. PMID 3083643.
- Court-Brown CM, McBirnie J, Wilson G (February 1998). "Adult ankle fractures--an increasing problem?". Acta Orthopaedica Scandinavica. 69 (1): 43–7. doi:10.3109/17453679809002355. PMID 9524517.