Aggressive fibromatosis
Aggressive fibromatosis or desmoid tumor is a rare condition. Desmoid tumors are a type of fibromatosis and related to sarcoma, though without the ability to spread throughout the body (metastasize). The tumors arise from cells called fibroblasts, which are found throughout the body and provide structural support, protection to the vital organs, and play a critical role in wound healing. These tumors tend to occur in women in their thirties, but can occur in anyone at any age. They can be either relatively slow-growing or malignant. However, aggressive fibromatosis is locally aggressive and can cause life-threatening problems or even death when the tumors compress vital organs such as intestines, kidneys, lungs, blood vessels, or nerves. The condition is rarely fatal. Most cases are sporadic, but some are associated with familial adenomatous polyposis (FAP). Approximately 10% of individuals with Gardner's syndrome, a type of FAP with extracolonic features, have desmoid tumors.[3]
| Aggressive fibromatosis | |
|---|---|
| Other names | Desmoid tumor, deep fibromatosis, desmoid fibromatosis |
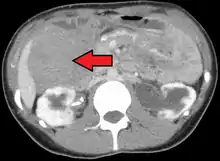
 | |
| Desmoid tumor as seen on CT scan | |
| Specialty | Oncology, surgery, radiology |
| Complications | Pain, loss of function, restricted movement |
| Usual onset | 30–40 years[1] |
| Risk factors | CTNNB1 and APC gene mutations, familial adenomatous polyposis, estrogen levels, pregnancy, physical trauma or surgery |
| Diagnostic method | Biopsy |
| Differential diagnosis | Broad, including fibroblastic sarcomas, superficial fibromatosis, nodular fasciitis, gastrointestinal stromal tumor, and scar tissue |
| Treatment | Watchful waiting; surgery; radiation therapy‚ chemotherapy; antiestrogen medication; NSAIDs; ablation with cold, heat, or ultrasound |
| Incidence | 5–6 per million per year[2] |
The World Health Organization reclassified desmoid tumors (termed desmoid-type fibromatosis) as a specific type of tumor in the category of intermediate (locally aggressive) fibroblastic and myofibroblastic tumors.[4]
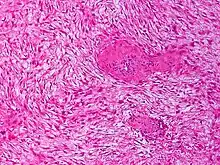
Histologically they resemble very low-grade fibrosarcomas,[5] but they are very locally aggressive and tend to recur even after complete resection. The condition is "characterized by a variable and often unpredictable clinical course."[2] There is a tendency for recurrence in the setting of prior surgery; in one study, two-thirds of patients with desmoid tumors had a history of prior abdominal surgery.[6] The condition can be chronic and may be debilitating.[7]
History and etymology

The condition was first described in 1832 by John MacFarlane. Desmoid, used by Johannes Peter Müller in 1838, comes from the Greek desmos 'band or tendon-like', describing the tumors' consistency.[8][9] The term found broad acceptance in the 1880s.[10] Over the next several decades, Georg Ledderhose and C. Pfeiffer compiled and reported a number of cases, reaching 400 by the early 1900s.[10] In 1923, Ralph W. Nichols first described the correlation between familial adenomatous polyposis (FAP) and desmoid tumors.[11] Arthur Purdy Stout coined the term fibromatosis (in the name congenital generalized fibromatosis, describing myofibromatosis) in 1954.[12]
Causes and risk factors
Wnt signaling pathway alterations are the likely cause of desmoid tumor formation.[13] Mutations have been discovered in both the beta-catenin encoding CTNNB1 gene and the tumor-suppressing APC gene, which affect the Wnt pathway. A 2015 study on desmoid tumors lacking these mutations found that almost all, 95%, "may have mutations that affect the Wnt/β-catenin pathway, suggesting a near universal relationship between desmoid tumors and Wnt signaling."[13]
The majority of cases are sporadic, most of which – 85% – involve a CTNNB1 mutation.[14] Of these, "the three distinct mutations identified are 41A, 45F, and 45. Mutation 45F is associated with a high risk of recurrence."[1] APC mutations affect FAP patients and make up a smaller percentage, 10–15%, of sporadic cases.[14]
The disease has a tendency to occur during and after pregnancy and in exposure to higher estrogen levels, suggesting a hormonal link.[15] One study noted the formation of desmoid tumors in guinea pigs after prolonged estrogen exposure.[16] Other factors include trauma and surgery.[13]
Risk factors for desmoid disease amongst FAP patients include female sex, a 3' APC mutation, a positive family history, and a history of previous abdominal surgery.[17]
Occurrence
The incidence of desmoid tumors is 5–6 per million per year;[2] they constitute 0.03% of tumors and less than 3% of soft-tissue tumors. The primary age range is 15–60, with a peak between 30 and 40 years old; more females than males are affected.[1][8] A 2012 retrospective multi-institutional analysis of 211 patients found a median age of 36 and a 68% female prevalence.[18] Children do not have the same sex disparity and are most commonly affected around 15 or 16 years old.[19]
Diagnosis
Diagnosis
A biopsy is always indicated as the definitive method to determine the nature of the tumor.[1] Diagnosis may be difficult in part due to the use of core needle biopsy over open biopsy.[20]
Similarities among bland spindle-cell lesions lead to a large number of possibilities in diagnosis, including fibroblastic sarcomas, Gardner fibroma, scar tissue or keloids, superficial fibromatosis, nodular fasciitis, myofibroma, collagenous fibroma, gastrointestinal stromal tumor, solitary fibrous tumor, and other conditions. Such conditions may therefore also be incorrectly diagnosed as desmoid tumors (29% of cases in one review).[21][15][22] Some 30–40% of desmoid tumors may be misdiagnosed.[23]
Classification
Desmoid tumors can occur almost anywhere in the body.[18] They are classified as extra-abdominal, abdominal wall, or intra-abdominal; the last is more common in patients with FAP.[24] Most cases occur in the mesentery, abdominal wall, and extremities.[25] One study has shown extra-abdominal tumors making up 43% of cases, abdominal tumors 49%, and mesenteric 8%, though statistics vary.[16] Pregnancy-related tumors typically arise in the abdominal wall.[26] Tumors located intra-abdominally or in the head and neck have the highest risk of mortality due to the proximity to vital structures.[19]
One analysis has shown a median tumor size of 7.5 cm (3.0 in).[18] Though metastasis cannot occur, the tumors may in some cases be multifocal, with several located in the same body part.[27]
A 3' APC mutation is the most significant risk factor for intra-abdominal desmoid development amongst FAP patients.[28] FAP patients presenting with an abdominal wall desmoid pre-operatively are at an increased risk of developing an intra-abdominal desmoid post-operatively.[29]
Desmoid tumors of the breast are rare, constituting 4% of extra-abdominal cases and 0.2% of breast tumors.[25] Although benign, they can mimic breast cancer on physical examination, mammography and breast ultrasound and can also be locally invasive. Even though they occur sporadically, they can also be seen as a part of Gardner's syndrome. Some cases – up to 44% – occur in patients who have previously had breast surgery.[30] A high index of suspicion and a thorough triple examination protocol is necessary to detect rare lesions like a desmoid tumor which can masquerade as breast carcinoma. Desmoid tumor of the breast may present a difficulty in the diagnosis especially where imaging studies are not conclusive and suggest a more ominous diagnosis.[31] They may arise in the chest wall or the breast itself.[16]
Desmoid tumors may occur in the head and neck, more commonly among children, and tend to be more aggressive than in other extra-abdominal locations. These tumors constitute up to 23% of extra-abdominal cases.[16]
Staging
There is no standard staging system; desmoid tumors do not fall under cancer staging systems as they do not metastasize.[30]
Disease course, treatment, and impacts
Disease course
The condition is "characterized by a variable and often unpredictable clinical course",[2] often considered chronic,[13] and with the potential to be debilitating.[7] Death, however, is uncommon.[19] Tumors may grow, regress, or remain stable:[23]
- Resolution without treatment (10–28%)
- Progression and resolution (30%)
- Stable (50%)
- Rapid progression (10%)
Management of these lesions is complex, the main problem being the high rates of recurrence particularly in FAP-associated disease. Recurrence rates in general vary from 19 to 77 percent.[16] Conversely, for intra-abdominal fibromatosis without evidence of FAP, although extensive surgery may still be required for local symptoms, the risk of recurrence appears to be lower.[32]
Treatment, trials, and management
Patients with desmoid tumors should be evaluated by a multi-disciplinary team of surgeons, medical oncologists, radiation oncologists, and geneticists. They should be treated by desmoid tumor experts, typically soft-tissue sarcoma specialists.[33][34][35] The 2020 global consensus paper on desmoid treatment notes, in a summary, that "Clearly, patients need to be referred to centers with experience in [desmoid tumors (DT)] to minimize the risk of active surveillance and avoid unnecessarily debilitating or mutilating surgery when possibly needed. Surgery by surgeons without significant experience in the management of DT is strongly discouraged."[36]
There is no definitive cure; patients are encouraged to enlist in clinical trials when possible.[37] Trials on selective gamma secretase inhibitors are underway as of 2023, with a Phase 2/3 trial on AL102 having begun in 2021 and a Phase 3 trial on nirogacestat having begun in 2019.[38][39] No treatments have yet received approval by the US Food and Drug Administration as of 2023.[23] Since there are "no established, evidence-based treatments",[40] individualized treatment and follow-up by specialists is necessary: "Due to the rarity of the disease, the level of evidence available for common types of cancer is unlikely ever to be available for [desmoid fibromatosis]."[2] Prediction of tumor response to specific forms of treatment is currently not possible.[15]
Surgery was the standard treatment for desmoid tumors up to the early 2000s.[2][41] Due to the condition's unpredictability, more conservative management such as watchful waiting has since become common due to the potential impacts of surgical interventions. As of the 2010s, there is a "clear consensus"[2] from medical groups, including the European Organization for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group and the European Society for Medical Oncology: immediate surgical resection is no longer the first-line treatment, particularly in asymptomatic patients.[13][25][2] Complete removal is not always possible due to the tumors' infiltrative nature and tendril-like growth.[15]
In more advanced, recurring, or rapidly progressing cases, treatment may consist of complete surgical removal, radiation therapy, antiestrogens (e.g. tamoxifen), nonsteroidal anti-inflammatory drugs (NSAIDs), chemotherapy, or ablation (cold, heat, ultrasound). Treatment with oral tyrosine kinase inhibitor drugs (e.g. imatinib, sorafenib, pazopanib) shows promising success rates.[42][27][43] Radiation therapy after surgery may improve outcomes.[15] Despite the condition's hormonal link, anti-hormonal therapies only appear to work in a small subset of patients.[15]
Intestinal transplant is a treatment option for those patients with complicated desmoid tumor, such as those involving the mesenteric root, or those with intestinal failure resulting from the tumor or prior interventions.[44]
MRI or CT imaging scans are commonly used for monitoring.[45][1]
Impacts
Though desmoid tumors do not metastasize, their invasiveness may lead to pain and loss of function or restricted movement. Chronic pain is an issue for as many as 63% of patients and may be debilitating.[23] Pressure on vital organs or deformity may occur.[46] The economic burden of treatment may be significant, with surgery costs estimated at $50,000 in 2022 US dollars.[41] Tumors may be misdiagnosed (30–40%)[23] due to their rarity and a lack of knowledge; patients may initially be given poor prognoses due to misdiagnosis with conditions such as malignant sarcoma.[40] Patients may need to visit multiple healthcare providers to receive a diagnosis, causing delay in care. Patients may experience issues including anxiety, fatigue, or trouble sleeping; their level of emotional distress has been "compared with that of patients with sarcoma, also a malignant connective tissue disorder".[23] A lack of knowledge by healthcare providers and of information available to patients and others have also been cited as issues.[40]
Specific instruments to determine health-related quality of life impacts for desmoid patients, the Gounder/Desmoid Tumor Research Foundation (DTRF) Desmoid Symptom/Impact Scale (GODDESS) and the Desmoid-type fibromatosis Quality of Life Questionnaire (DTF-QOL) have been developed and validated.[23]
ICD-10-CM diagnosis codes
Few rare diseases have a specific code in the International Classification of Diseases.[47] As of October 2023, specific codes for desmoid tumors will be included in the ICD-10-CM, the United States' diagnosis code system, after a request from the Desmoid Tumor Research Foundation.[48] A subcategory of D48.1, Neoplasm of uncertain behavior of connective and other soft tissue, has been created with more specific codes:[47]
- D48.11: Desmoid tumor
- D48.110: Desmoid tumor of head and neck
- D48.111: Desmoid tumor of chest wall
- D48.112: Desmoid tumor, intrathoracic
- D48.113: Desmoid tumor of abdominal wall
- D48.114: Desmoid tumor, intraabdominal
- Desmoid tumor of pelvic cavity
- Desmoid tumor, peritoneal, retroperitoneal
- D48.115: Desmoid tumor of upper extremity and shoulder girdle
- D48.116: Desmoid tumor of lower extremity and pelvic girdle
- Desmoid tumor of buttock
- D48.117: Desmoid tumor of back
- D48.118: Desmoid tumor of other site
- D48.119: Desmoid tumor of unspecified site
Notable patients
- Dave Dravecky, American baseball pitcher and motivational speaker[49][50]
- Kevin Reilly, American football player[51]
In animals
Desmoid tumors occur in dogs, primarily on the head, and more infrequently in horses and cats.[52] A case has also been observed in a goat.[53]
References
- Master SR, Mangla A, Puckett Y, Shah C (January 2023). "Desmoid Tumor". StatPearls. Treasure Island: StatPearls Publishing. PMID 29083753. Retrieved 2023-08-14 – via National Institutes of Health.
- Kasper B, Baumgarten C, Garcia J, Bonvalot S, Haas R, Haller F, et al. (October 2017). "An update on the management of sporadic desmoid-type fibromatosis: a European Consensus Initiative between Sarcoma PAtients EuroNet (SPAEN) and European Organization for Research and Treatment of Cancer (EORTC)/Soft Tissue and Bone Sarcoma Group (STBSG)". Annals of Oncology. 28 (10): 2399–2408. doi:10.1093/annonc/mdx323. PMC 5834048. PMID 28961825.
- Nieuwenhuis MH, De Vos Tot Nederveen Cappel W, Botma A, Nagengast FM, Kleibeuker JH, Mathus-Vliegen EM, et al. (February 2008). "Desmoid tumors in a dutch cohort of patients with familial adenomatous polyposis". Clinical Gastroenterology and Hepatology. 6 (2): 215–219. doi:10.1016/j.cgh.2007.11.011. PMID 18237870. S2CID 26052046.
- Sbaraglia M, Bellan E, Dei Tos AP (April 2021). "The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives". Pathologica. 113 (2): 70–84. doi:10.32074/1591-951X-213. PMC 8167394. PMID 33179614.
- "desmoid" at Dorland's Medical Dictionary
- Lynch HT, Fitzgibbons R (December 1996). "Surgery, desmoid tumors, and familial adenomatous polyposis: case report and literature review". The American Journal of Gastroenterology. 91 (12): 2598–2601. PMID 8946994.
- Valesano JC, Schmitz JJ, Jensen NM, Schultz GR, Callstrom MR (December 2017). "Desmoid Tumors: A Review of Their Natural History, Imaging, and Treatment". Journal of Radiology Nursing. 36 (4): 211–217. doi:10.1016/j.jradnu.2017.09.003.
- Ravi V, Patel SR, Raut CP, Baldini EH, Berman RS, Pollock RE (January 2022). "Desmoid tumors: Epidemiology, molecular pathogenesis, clinical presentation, diagnosis, and local therapy". UpToDate. Retrieved 2023-08-14.
- Hajdu SI (May 2007). "Soft tissue sarcomas". Cancer. 109 (9): 1697–1704. doi:10.1002/cncr.22608. PMID 17366588. S2CID 39827598.
- Nichols RW (1923-07-01). "Desmoid tumors: a report of thirty-one cases". Archives of Surgery. 7 (1): 227. doi:10.1001/archsurg.1923.01120010230013. ISSN 0004-0010.
- "Gardner Syndrome: Practice Essentials, Anatomy, Pathophysiology". eMedicine. 2022-04-29.
- Beck JC, Devaney KO, Weatherly RA, Koopmann CF, Lesperance MM (January 1999). "Pediatric myofibromatosis of the head and neck". Archives of Otolaryngology–Head & Neck Surgery. 125 (1): 39–44. doi:10.1001/archotol.125.1.39. PMID 9932585. S2CID 19440724.
- Howard JH, Pollock RE (June 2016). "Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis". Oncology and Therapy. 4 (1): 57–72. doi:10.1007/s40487-016-0017-z. PMC 5315078. PMID 28261640.
- "Desmoid tumor: MedlinePlus Genetics". National Library of Medicine MedlinePlus. Retrieved 2023-08-14.
- Kasper B, Ströbel P, Hohenberger P (2011-05-01). "Desmoid tumors: clinical features and treatment options for advanced disease". The Oncologist. 16 (5): 682–693. doi:10.1634/theoncologist.2010-0281. PMC 3228186. PMID 21478276.
- Weiss SW, Goldblum JR, Folpe AL (2007). "Deep Fibromatosis". Enzinger and Weiss's Soft Tissue Tumors (5th ed.). Elsevier Health Sciences. ISBN 9780323076159.
- Sinha A, Tekkis PP, Gibbons DC, Phillips RK, Clark SK (November 2011). "Risk factors predicting desmoid occurrence in patients with familial adenomatous polyposis: a meta-analysis". Colorectal Disease. 13 (11): 1222–1229. doi:10.1111/j.1463-1318.2010.02345.x. PMID 20528895. S2CID 26117431.
- Peng PD, Hyder O, Mavros MN, Turley R, Groeschl R, Firoozmand A, et al. (December 2012). "Management and recurrence patterns of desmoids tumors: a multi-institutional analysis of 211 patients". Annals of Surgical Oncology. 19 (13): 4036–4042. doi:10.1245/s10434-012-2634-6. PMC 3568525. PMID 22972507.
- "Desmoid Tumor - Statistics". Cancer.Net. American Society of Clinical Oncology. 2020-09-02. Retrieved 2023-08-14.
- Le Guellec S, Soubeyran I, Rochaix P, Filleron T, Neuville A, Hostein I, Coindre JM (December 2012). "CTNNB1 mutation analysis is a useful tool for the diagnosis of desmoid tumors: a study of 260 desmoid tumors and 191 potential morphologic mimics". Modern Pathology. 25 (12): 1551–1558. doi:10.1038/modpathol.2012.115. PMID 22766794. S2CID 24471719.
- Goldstein JA, Cates JM (July 2015). "Differential diagnostic considerations of desmoid-type fibromatosis". Advances in Anatomic Pathology. 22 (4): 260–266. doi:10.1097/PAP.0000000000000077. PMID 26050263.
- "Differential Diagnosis - Abdominal Desmoid Fibromatosis - Surgical Pathology Criteria". Stanford University School of Medicine. Retrieved 2023-08-19.
- Bektas M, Bell T, Khan S, Tumminello B, Fernandez MM, Heyes C, Oton AB (September 2023). "Desmoid Tumors: A Comprehensive Review". Advances in Therapy. 40 (9): 3697–3722. doi:10.1007/s12325-023-02592-0. PMC 10427533. PMID 37436594.
- "Desmoid Tumor - Symptoms, Causes, Treatment". National Organization for Rare Disorders. Retrieved 2023-05-07.
- Lorenzen J, Cramer M, Buck N, Friedrichs K, Graubner K, Lühr CS, et al. (February 2021). "Desmoid Type Fibromatosis of the Breast: Ten-Year Institutional Results of Imaging, Histopathology, and Surgery". Breast Care. 16 (1): 77–84. doi:10.1159/000507842. PMC 7923936. PMID 33708054.
- "Desmoid Tumor - Risk Factors". Cancer.Net. American Society of Clinical Oncology. 2020-09-02. Retrieved 2023-08-19.
- Alman B, Attia S, Baumgarten C, Benson C, Blay JY, Bonvalot S, et al. (Desmoid Tumor Working Group) (March 2020). "The management of desmoid tumours: A joint global consensus-based guideline approach for adult and paediatric patients". European Journal of Cancer. 127: 96–107. doi:10.1016/j.ejca.2019.11.013. PMID 32004793. S2CID 210998595.
- Sinha A, Tekkis PP, Neale KF, Phillips RK, Clark SK (June 2010). "Risk factors predicting intra-abdominal desmoids in familial adenomatous polyposis: a single centre experience". Techniques in Coloproctology. 14 (2): 141–146. doi:10.1007/s10151-010-0573-4. PMID 20352275. S2CID 24922322.
- Sinha A, Gibbons DC, Phillips RK, Clark S (September 2010). "Surgical prophylaxis in familial adenomatous polyposis: do pre-existing desmoids outside the abdominal cavity matter?". Familial Cancer. 9 (3): 407–411. doi:10.1007/s10689-010-9342-9. PMID 20428953. S2CID 20685381.
- Li GZ, Raut CP, Hunt KK, Feng M, Chugh R (March 2021). "Breast Sarcomas, Phyllodes Tumors, and Desmoid Tumors: Epidemiology, Diagnosis, Staging, and Histology-Specific Management Considerations". American Society of Clinical Oncology Educational Book. American Society of Clinical Oncology. Annual Meeting. 41 (41): 390–404. doi:10.1200/EDBK_321341. PMID 34010054.
- Rammohan A, Wood JJ (2012). "Desmoid tumour of the breast as a manifestation of Gardner's syndrome". International Journal of Surgery Case Reports. 3 (5): 139–142. doi:10.1016/j.ijscr.2012.01.004. PMC 3312056. PMID 22370045.
- Wilkinson MJ, Fitzgerald JE, Thomas JM, Hayes AJ, Strauss DC (May 2012). "Surgical resection for non-familial adenomatous polyposis-related intra-abdominal fibromatosis". The British Journal of Surgery. 99 (5): 706–713. doi:10.1002/bjs.8703. PMID 22359346. S2CID 205512855.
- "Newly-Diagnosed?". Desmoid Tumor Research Foundation. Retrieved 2023-08-15.
- "Desmoid-type fibromatosis". Sarcoma UK. Retrieved 2023-08-15.
- "Soft Tissue Sarcoma: Desmoid Tumors: What They Are, Causes, Symptoms, and Treatment". Memorial Sloan Kettering Cancer Center. Retrieved 2023-08-15.
- "The Management of Desmoid Tumors: A joint global evidence-based consensus guideline approach for adult and pediatric patients" (PDF). Desmoid Tumor Research Foundation (Booklet). The Desmoid Tumor Working Group. 2020.
- "About Desmoid Tumors". Desmoid Tumor Research Foundation. Archived from the original on 2015-07-27. Retrieved 2015-08-04.
- "A Study of AL102 in Patients With Progressing Desmoid Tumors (RINGSIDE)". ClinicalTrials.gov. Retrieved 2023-08-19.
- "Nirogacestat for Adults With Desmoid Tumor/Aggressive Fibromatosis (DT/AF) (DeFi)". ClinicalTrials.gov. Retrieved 2023-08-19.
- Husson O, Younger E, Dunlop A, Dean L, Strauss DC, Benson C, et al. (March 2019). "Desmoid fibromatosis through the patients' eyes: time to change the focus and organisation of care?". Supportive Care in Cancer. 27 (3): 965–980. doi:10.1007/s00520-018-4386-8. PMC 6373240. PMID 30155568.
- Fernandez, Maria M.; Bell, Timothy; Tumminello, Brad; Khan, Shahnaz; Zhou, Shengfan; Oton, Ana B. (2023-07-03). "Disease and economic burden of surgery in desmoid tumors: a review". Expert Review of Pharmacoeconomics & Outcomes Research. 23 (6): 607–618. doi:10.1080/14737167.2023.2203915. ISSN 1473-7167.
- Ganeshan D, Amini B, Nikolaidis P, Assing M, Vikram R (2019). "Current Update on Desmoid Fibromatosis". Journal of Computer Assisted Tomography. 43 (1): 29–38. doi:10.1097/RCT.0000000000000790. PMC 6331223. PMID 30211798.
- "Diagnosis and Treatment". Desmoid Tumor Research Foundation. Retrieved 22 October 2021.
- Chatzipetrou MA, Tzakis AG, Pinna AD, Kato T, Misiakos EP, Tsaroucha AK, et al. (March 2001). "Intestinal transplantation for the treatment of desmoid tumors associated with familial adenomatous polyposis". Surgery. 129 (3): 277–281. doi:10.1067/msy.2001.110770. PMID 11231455.
- Schwartz RA, Lambert PC, Shear N (2023-06-22). Butler DF, Elston DM (eds.). "Desmoid Tumor: Practice Essentials, Pathophysiology, Etiology". eMedicine. Retrieved 2023-08-14.
- J (ed.). "Desmoid Tumor - an overview". ScienceDirect. Retrieved 2023-08-19.
- "Diagnosis Codes & Desmoid Tumors". Desmoid Tumor Research Foundation. Retrieved August 12, 2023.
- "ICD-10 Coordination and Maintenance Committee Meeting" (PDF). Centers for Disease Control and Prevention. March 8–9, 2022. Retrieved August 12, 2023.
- Nack W (July 22, 1991). "'Let's Make the Best of It'". Sports Illustrated Vault.
- "Former MLB player Dave Dravecky to Headline Cancer Survivorship Conference Sept. 16-17". MD Anderson Cancer Center. 2011-06-14. Retrieved 2023-08-14.
- "Kevin Reilly - Sarcoma Cancer Research & Treatment". Sarcoma Foundation of America. Retrieved 2023-08-16.
- "Connective Tissue Tumors in Animals - Integumentary System". MSD Veterinary Manual. Retrieved 2023-08-14.
- Tontis A, Rossi GL (August 1993). "[First description of a desmoid tumor in a goat and comparative observations to human fibromatosis. Case report]". Tierarztliche Praxis (in German). 21 (4): 306–311. PMID 8211956.