Hip dysplasia
Hip dysplasia is an abnormality of the hip joint where the socket portion does not fully cover the ball portion, resulting in an increased risk for joint dislocation.[1] Hip dysplasia may occur at birth or develop in early life.[1] Regardless, it does not typically produce symptoms in babies less than a year old.[3] Occasionally one leg may be shorter than the other.[1] The left hip is more often affected than the right.[3] Complications without treatment can include arthritis, limping, and low back pain.[3] Females are affected more often than males.[1] Risk factors for hip dysplasia include female sex, family history, certain swaddling practices, and breech presentation whether an infant is delivered vaginally or by cesarean section.[3] If one identical twin is affected, there is a 40% risk the other will also be affected.[3] Screening all babies for the condition by physical examination is recommended.[3] Ultrasonography may also be useful.[3]
| Hip dysplasia | |
|---|---|
| Other names | Developmental dysplasia of the hip (DDH),[1] developmental dislocation of the hip,[1] congenital dysplasia of the hip (CDH)[2] |
 | |
| Congenital dislocation of the left hip in an elderly person. Closed arrow marks the acetabulum, open arrow the femoral head. | |
| Specialty | Pediatrics, orthopedics |
| Symptoms | None, hip aches, one leg shorter, limping[1] |
| Complications | Arthritis[3] |
| Risk factors | Family history, swaddling, breech birth[3] |
| Diagnostic method | Physical exam, ultrasound[3] |
| Treatment | Bracing, casting, surgery[3] |
| Prognosis | Good (if detected early)[1] |
| Frequency | 1 in 1,000 (term babies)[3] |
Many of those with mild instability resolve without specific treatment.[3] In more significant cases, if detected early, bracing may be all that is required.[3] In cases that are detected later, surgery and casting may be needed.[3] About 7.5% of hip replacements are done to treat problems which have arisen from hip dysplasia.[3]
About 1 in 1,000 babies have hip dysplasia.[3] Hip instability of meaningful importance occurs in one to two percent of babies born at term.[3] Females are affected more often than males.[1] Hip dysplasia was described at least as early as the 300s BC by Hippocrates.[4]
Signs and symptoms
Hip dysplasia can range from barely detectable to severely malformed or dislocated. The congenital form, teratologic or non-reducible dislocation occurs as part of more complex conditions.
The condition can be bilateral or unilateral:
- If both hip joints are affected, one speaks of "bilateral" dysplasia. In this case, some diagnostic indicators like asymmetric folds and leg-length inequality do not apply.
- In unilateral dysplasia only one joint shows deformity, the opposite side may show resulting effects.[5] In the majority of unilateral cases, the left hip has the dysplasia.
If the joint is fully dislocated a false acetabulum often forms (often higher up on the pelvis) opposite the dislocated femoral head position.
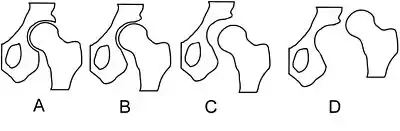
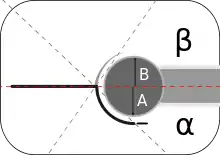
In acetabular dysplasia, the acetabulum (socket) is too shallow or deformed. The center-edge angle is measured as described by Wiberg.[6] Two forms of femoral dysplasia are coxa vara, in which the femur head grows at too narrow an angle to the shaft, and coxa valga, in which the angle is too wide.
A rare type, the "Beukes familial hip dysplasia" is found among Afrikaners that are members of the Beukes family. The femur head is flat and irregular. People develop osteoarthritis at an early age.[7]
Causes
Hip dysplasia is considered to be a multifactorial condition. That means that several factors are involved in causing the condition to manifest.[8]
The cause of the condition is unknown; however, some factors of congenital hip dislocation are through heredity and racial background. It is also thought that the higher rates in some ethnic groups (such as some Native American groups) is due to the practice of swaddling of infants, which is known to be a potential risk factor for developing dysplasia. It also has a low risk in African Americans and southern Chinese.
Congenital
Some studies suggest a hormonal link.[9] Specifically, the hormone relaxin has been indicated.[10]
Female sex, alone without other known risk factors, accounts for 75%.[11] A genetic factor is indicated since the trait runs in families and there is an increased occurrence in some ethnic populations (e.g., Native Americans,[12] Lapps[13] / Sami people[14]). A locus has been described on chromosome 13.[15] Beukes familial dysplasia, on the other hand, was found to map to an 11-cM region on chromosome 4q35, with nonpenetrant carriers not affected.[16] Further risk factors include , gender, genetics (family history),[17][18] and firstborns.[19]
Acquired
In the breech position the femoral head tends to get pushed out of the socket and the breech position is probably the most important single risk factor, whether an infant is delivered vaginally or by cesarean section.[3]
As an acquired condition it has been linked to traditions of swaddling infants,[20] use of overly restrictive baby seats, carriers and other methods of transporting babies,[21] or use of a cradle board which locks the hip joint in an "adducted" position (pulling the knees together tends to pull the heads of the femur bone out of the sockets or acetabulae) for extended periods. Modern swaddling techniques, such as the 'hip healthy swaddle' have been developed to relieve stress on hip joints caused by traditional swaddling methods.[22]
A narrow uterus also facilitates hip joint dislocation during fetal development and birth.
Screening and diagnosis


All newborns should be screened for congenital hip dysplasia. The screening examination techniques to detect hip dysplasia in newborns include observation for
- asymmetry of legs and asymmetrical gluteal folds ,[23]
- limb length discrepancy (evaluated by placing the child in a supine position with the hips and knees flexed [unequal knee heights might be noticed – the Galeazzi sign]), and
- restricted hip abduction.
Sometimes during an exam a "click" or more precisely "clunk" in the hip may be detected[24] (although not all clicks indicate hip dysplasia).[25] When a hip click (also known as "clicky hips" in the UK) is detected, the child's hips are tracked with additional screenings[26] to determine if developmental dysplasia of the hip is caused.[27]
Two maneuvers commonly employed for diagnosis in neonatal exams are the Ortolani maneuver and the Barlow maneuver.[28][29]
In order to do the Ortolani maneuver it is recommended that the examiner put the newborn baby in a position in which the opposite hip is held still while the thigh of the hip being tested is abducted and gently pulled anteriorly. If a "clunk" is heard (the sound of the femoral head moving over the acetabulum), the joint is normal, but absence of the "clunk" sound indicates that the acetabulum is not fully developed. The next method that can be used is called the Barlow maneuver. It is done by adducting the hip while pushing the thigh posteriorly. If the hip goes out of the socket it means it is dislocated, and the newborn has a congenital hip dislocation. The baby is laid on its back for examination by separation of its legs. If a clicking sound can be heard, it indicates that the baby may have a dislocated hip. It is highly recommended that these maneuvers be done when the baby is not fussing, because the baby may inhibit hip movement.
There is some evidence suggesting that hip examinations in newborns are painful and pain relief in the form of oral glucose has been suggested but is not yet widely accepted.[30][31]
Most vexingly, many newborn hips show a certain ligamentous laxity, on the other hand severely malformed joints can appear stable. That is one reason why follow-up exams and developmental monitoring are important. Physical examination of newborns followed by appropriate use of hip ultrasound is widely accepted.[32]
The Harris hip score[33] (developed by William H. Harris MD, an orthopedist from Massachusetts) is one way to evaluate hip function following surgery. Other scoring methods are based on patients' evaluation like e.g. the Oxford hip score, HOOS and WOMAC score.[34] Children's Hospital Oakland Hip Evaluation Scale (CHOHES) is a modification of the Harris hip score that is currently being evaluated.[35]
Hip dysplasia can develop in older age. Adolescents and adults with hip dysplasia may present with a waddling gait, Trendelenburg's sign, decreased hip abduction, hip pain and in some cases hip labral tears. X-rays are used to confirm a diagnosis of hip dysplasia. CT scans and MRI scans are occasionally used too.[36][37]
Terminology
Some sources prefer "developmental dysplasia of the hip" (DDH) to "congenital dislocation of the hip" (CDH), finding the latter term insufficiently flexible in describing the diversity of potential complications.[38]
The use of the word congenital can also imply that the condition already exists at birth. This terminology introduces challenges, because the joint in a newborn is formed from cartilage and is still malleable, making the onset difficult to ascertain. The newer term DDH also encompasses occult dysplasia (e.g. an underdeveloped joint) without dislocation and a dislocation developing after the "newborn" phase.
The term is not used consistently. In pediatric/neonatal orthopedics it is used to describe unstable/dislocatable hips and poorly developed acetabula. For adults it describes hips showing abnormal femur head or acetabular x-rays.[39][40]
Some sources prefer the term "hip dysplasia" over DDH, considering it to be "simpler and more accurate", partly because of the redundancy created by the use of the terms developmental and dysplasia.[41] Types of DDH include subluxation, dysplasia, and dislocation. The main types are the result of either laxity of the supporting capsule or an abnormal acetabulum.
Imaging
Hip dysplasia can be diagnosed by ultrasound[42] and projectional radiography ("X-ray").[43] Ultrasound imaging is generally preferred at up to 4 months due to limited ossification of the femoral head up until then, and is the most accurate method for imaging of the hip during the first few months after birth. However, in most instances, ultrasound screening should not be performed before 3 to 4 weeks of age because of the normal physiologic laxity.[44][notes 1] When universal with targeted ultrasound screening was compared, the former results in an insignificant reduction in the late diagnosis of hip dysplasia, which is why universal ultrasonographic screening of newborn infants is not recommended by the American Academy of Pediatrics.[11]
Despite the widespread use of ultrasound, pelvis X-ray is still frequently used to diagnose or monitor hip dysplasia or for assessing other congenital conditions or bone tumors.[45]
| Age | Scenario | Usual appropriate initial imaging |
|---|---|---|
| <4 weeks | Equivocal physical examination or risk factors | No imaging |
| Physical findings of DDH | Ultrasonography | |
| 4 weeks - 4 months | Equivocal physical examination or risk factors | Ultrasonography |
| 4 – 6 months | Concern for DDH | X-ray. Ultrasonography may be appropriate[notes 1] |
| >6 months | X-ray |
The most useful lines and angles that can be drawn in the pediatric pelvis assessing hip dysplasia are as follows:[45] Different measurements are used in adults.[45]


Treatment
Hip dysplasia presents a nearly perfect equilibrium between the arthritis, movement/mobility problems and pain associated with the developmental malformation, and the arthritis, movement/mobility problems and pain that are, as often as not in moderate to severe cases, inflicted by the treatment itself.
However, given the very real possibility of a limp, constant and/or debilitating pain, complicated treatment and impaired mobility later in life, careful developmental monitoring is indicated and early intervention is often the best result. The worst possible consequence of non treatment is developing early arthritis, sometimes even during teenage years. All treatment aims to delay the onset of arthritis, but no treatment is fully successful in avoiding it; and, all available treatments bear the risk of inflicting equivalent damage. Most unfortunately, studies have as yet been unable to find a method of predicting outcomes in either the surgical/orthopedic treatment of the condition in infants and young children, or the surgical treatment of these early treatments' negative outcomes later in life (such as arthritis, avascular necrosis, trochanteric bursitis, and bone spurs of up to 3.5 cm just medial of the gluteus maximus insertion point on the greater trochanter due to excessive friction).
Harnesses, casts, and traction
Early hip dysplasia can often be treated using a Pavlik harness[46] (see photograph) or the Frejka pillow/splint[47] in the first year of life with usually normal results. Complications can occur when using the Pavlik harness. Cases of femoral nerve palsy[48] and avascular necrosis of the femoral head have been reported with the use of the Pavlik harness,[49] but whether these cases were due to improper application of the device or a complication encountered in the course of the disorder remains unresolved. Complications arise mainly because the sheet of the iliopsoas muscle pushes the circumflex artery against the neck of the femur and decreases blood flow to the femoral head, so the Frejka pillow is not indicated in all the forms of the developmental dysplasia of the hip.
 Baby wearing a Pavlik harness
Baby wearing a Pavlik harness Diagram of Pavlik harness
Diagram of Pavlik harness Diagram of Frejka pillow
Diagram of Frejka pillow Traction
Traction
Other devices employed include the spica cast,[50] particularly following surgical closed reduction, open reduction, or osteotomy in babies and young children. Traction is sometimes used in the weeks leading up to a surgery to help stretch ligaments in the hip joint, although its use is controversial and varies amongst physicians.[51]
Surgery
In older children the adductor and iliopsoas muscles may have to be treated surgically because they adapt to the dislocated joint position (contracture). Braces and splints are often used following either of these methods to continue treatment. Although some children "outgrow" untreated mild hip dysplasia[40] and some forms of untreated dysplasia cause little or no impairment of quality of life, studies have as yet been unable to find a method of predicting outcomes. On the other hand, it has often been documented that starting treatment late leads to complications and ends in poor results.
Hip replacement and osteotomy
Hip dysplasia is often cited as causing osteoarthritis of the hip at a comparatively young age. Dislocated load bearing surfaces lead to increased and unusual wear, although there are studies that contradict these findings (see[52][53]). Peri-acetabular osteotomy (PAO) surgery can be used to realign the hip joint in some adolescents and adults. Subsequent treatment with total hip arthroplasty (hip replacement) is complicated by a need for revision surgery (replacing the artificial joint) owing to skeletal changes as the body matures, loosening/wear or bone resorption. Hip resurfacing is another option for correcting hip dysplasia in adults. It is a type of hip replacement that preserves more bone, and may work for younger hip dysplasia patients.[54]
Osteotomies are either used in conjunction with arthroplasty or by themselves to correct misalignment.
Epidemiology
Determining the incidence can be difficult.[55][56] In addition there is a wide margin in diagnostic results. A German study comparing two methods resulted in twice the usual rate for one method. The condition is eight times more frequent in females than in males.[9]
Native Americans are more likely to have congenital hip dislocation than any of the other races. The risk for Native Americans is about 25–50 in 1000. The overall frequency of developmental dysplasia of the hip is approximately 1 case per 1000 individuals; however, Barlow believed that the incidence of hip instability in newborns can be as high as 1 case for every 60 newborns,[57] with the rate dropping to 1:240 at one week.[58]
History
The Frejka pillow splint was named after Dr. Bedrich Frejka (1890-1972), a Czech orthopedic surgeon. The Pavlik harness was named after Dr. Arnold Pavlik (1902-1962), also a Czech orthopedic surgeon.
Society and culture
In the television program ER, Kerry Weaver uses a crutch owing to congenital hip dysplasia. In season 12, she undergoes a hip replacement to cure her dysplasia when her previously untreated joint worsens.[59]
Research
One avenue of research is using stem cells. They are applied in grafting (bone grafting) or by seeding porous arthroplasty prosthesis with autologous fibroblasts or chondrocyte progenitor cells to assist in firmly anchoring the artificial material in the bone bed.
Other animals
In dogs, hip dysplasia is an abnormal formation of the hip socket that, in its more severe form, can eventually cause crippling lameness and painful arthritis of the joints. It is a genetic (polygenic) trait that is affected by environmental factors. It is common in many dog breeds, particularly the larger breeds.
Hip dysplasia is one of the most studied veterinary conditions in dogs, and the most common single cause of arthritis of the hips. Cats are also known to have this condition, especially Siamese.[60]
Notes
- Ultrasonography is the imaging method of choice up to 6 months for the nonoperative surveillance imaging in harness of known diagnosis of DDH.
- "ACR Appropriateness Criteria - Developmental Dysplasia of the Hip (DDH)–Child". American College of Radiology. Revised 2018
References
- "Your Orthopaedic Connection: Developmental Dysplasia of the Hip". American Academy of Orthopaedic Surgeons. October 2013.
- "Definition: congenital dysplasia of the hip from Online Medical Dictionary".
- Shaw, BA; Segal, LS; SECTION ON, ORTHOPAEDICS. (December 2016). "Evaluation and Referral for Developmental Dysplasia of the Hip in Infants". Pediatrics. 138 (6): e20163107. doi:10.1542/peds.2016-3107. PMID 27940740.
- Bentley, George (2009). European Instructional Lectures: Volume 9, 2009; 10th EFORT Congress, Vienna, Austria. Springer Science & Business Media. p. 40. ISBN 9783642009662.
- Jacobsen S, Rømer L, Søballe K (2006). "The other hip in unilateral hip dysplasia". Clin. Orthop. Relat. Res. 446: 239–46. doi:10.1097/01.blo.0000201151.91206.50. PMID 16721954. S2CID 11709860.
- Wiberg G. Studies of acetabular and congenital subluxation of the hip joint with special reference to complication of osteoarthritis Acta Chir Scand 1939, 83(Suppl. 58)
- Cilliers HJ, Beighton P (1990). "Beukes familial hip dysplasia: an autosomal dominant entity". Am. J. Med. Genet. 36 (4): 386–90. doi:10.1002/ajmg.1320360403. PMID 2389793.
- Lynn T Staheli, Fundamentals of Pediatric Orthopedics, p 13
- "Clinical Practice Guideline: Early Detection of Developmental Dysplasia of the Hip -- Committee on Quality Improvement and Subcommittee on Developmental Dysplasia of the Hip 105 (4): 896 -- AAP Policy". 29 January 2005. Archived from the original on 29 January 2005.
- Forst J, Forst C, Forst R, Heller KD (1997). "Pathogenetic relevance of the pregnancy hormone relaxin to inborn hip instability". Arch Orthop Trauma Surg. 116 (4): 209–12. doi:10.1007/BF00393711. PMID 9128773. S2CID 32322656.
- Shaw, Brian A.; Segal, Lee S.; SECTION ON ORTHOPAEDICS; et al. (1 December 2016). "Evaluation and Referral for Developmental Dysplasia of the Hip in Infants". Pediatrics. 138 (6): e20163107. doi:10.1542/peds.2016-3107. ISSN 0031-4005. PMID 27940740. S2CID 32575088.
- Morcuende, Jose A.; Weinstein, Stuart L. "Developmental dysplasia of the hip: natural history, results of treatment, and controversies. In: Bourne R, ed. Controversies in Hip Surgery" (PDF). Oxford University Press. Archived from the original (PDF) on 26 July 2011.
- The occurrence of hip joint dislocation in early Lappic populations of Norway, Per Holck, Anthropological Department, Anatomical Institute, Box 1105 Blindern, N-0317 Oslo 3, Norway
- Forsdahl A (2000). "[A physician from Finnmark who pointed out the significance of heredity in congenital hip dysplasia]". Tidsskr. Nor. Legeforen. (in Norwegian). 120 (22): 2672–3. PMID 11077514.
- Mabuchi A, Nakamura S, Takatori Y, Ikegawa S (2006). "Familial osteoarthritis of the hip joint associated with acetabular dysplasia maps to chromosome 13q". Am. J. Hum. Genet. 79 (1): 163–8. doi:10.1086/505088. PMC 1474113. PMID 16773577.
- "AJHG - Autosomal Dominant (Beukes) Premature Degenerative Osteoarthropathy of the Hip Joint Maps to an 11-cM Region on Chromosome 4q35". 6 May 2008. Archived from the original on 6 May 2008.
- Hashmi, Jamil; Basit, Sulman; Khoshhal, Khalid (August 2019). "Genetics of developmental dysplasia of the hip: Recent progress and future perspectives". Journal of Musculoskeletal Surgery and Research. 3 (3): 245. doi:10.4103/jmsr.jmsr_46_19. S2CID 199547368.
- "Causes of Developmental Dysplasia of the Hip - International Hip Dysplasia Institute". 13 April 2020.
- "Developmental Dislocation of the Hip - Wheeless' Textbook of Orthopaedics". 22 July 2020.
- Mahan ST, Kasser JR (2008). "Does swaddling influence developmental dysplasia of the hip?". Pediatrics. 121 (1): 177–8. doi:10.1542/peds.2007-1618. PMID 18166571. S2CID 37598276.
- "Baby Carriers, Seats, & Other Equipment - International Hip Dysplasia Institute". Archived from the original on 18 November 2020. Retrieved 25 June 2012.
- "Hip-Healthy Swaddling - International Hip Dysplasia Institute". 28 May 2020.
- "Asymmetry Symptoms of DDH". Archived from the original on 25 October 2020. Retrieved 31 August 2012.
- "HipDysplasia - Newborn Nursery at LPCH - Stanford University School of Medicine". 5 July 2023.
- Kamath S, Bramley D (2005). "Is 'clicky hip' a risk factor in developmental dysplasia of the hip?". Scott Med J. 50 (2): 56–8. doi:10.1177/003693300505000205. PMID 15977515. S2CID 23000620.
- "Newborn Screening and Prevention - International Hip Dysplasia Institute". Archived from the original on 12 November 2020. Retrieved 31 August 2012.
- "Hip Clicks and Hip Dysplasia - International Hip Dysplasia Institute". Archived from the original on 4 December 2020. Retrieved 31 August 2012.
- "Physical Examination of Infants - International Hip Dysplasia Institute". Archived from the original on 20 October 2020. Retrieved 31 August 2012.
- French LM, Dietz FR; Dietz (July 1999). "Screening for developmental dysplasia of the hip". American Family Physician. 60 (1): 177–84, 187–8. PMID 10414637.
- Olsson, Emma; Pettersson, Miriam; Eriksson, Mats; Ohlin, Andreas (April 2019). "Oral sweet solution to prevent pain during neonatal hip examination: a randomised controlled trial". Acta Paediatrica. 108 (4): 626–629. doi:10.1111/apa.14588. PMC 6585692. PMID 30246505.
- Pettersson, Miriam; Olsson, Emma; Ohlin, Andreas; Eriksson, Mats (September 2019). "Neurophysiological and behavioral measures of pain during neonatal hip examination". Paediatric and Neonatal Pain. 1 (1): 15–20. doi:10.1002/pne2.12006. ISSN 2637-3807. PMC 8974883. PMID 35546870.
- "Physician Newborn Screening and Prevention - International Hip Dysplasia Institute". Archived from the original on 12 November 2020. Retrieved 31 August 2012.
- "Harris Hip Score - Orthopaedic Scores". www.orthopaedicscore.com.
- Wylde V, Learmonth ID, Cavendish VJ (2005). "The Oxford hip score: the patient's perspective". Health Qual Life Outcomes. 3: 66. doi:10.1186/1477-7525-3-66. PMC 1283979. PMID 16259627.
- Aguilar CM, Neumayr LD, Eggleston BE, et al. (2005). "Clinical evaluation of avascular necrosis in patients with sickle cell disease: Children's Hospital Oakland Hip Evaluation Scale--a modification of the Harris Hip Score". Arch Phys Med Rehabil. 86 (7): 1369–75. doi:10.1016/j.apmr.2005.01.008. PMID 16003666.
- Betsy Miller, The Parents' Guide to Hip Dysplasia, p 19.
- Sutherland, Denise; West, Sophie (2011). A Guide for Adults with Hip Dysplasia. Lulu.com. pp. 7, 21–23. ISBN 978-0-9872152-0-8. Archived from the original on 10 April 2013. Retrieved 2 April 2013.
- Skaggs, David L.; Storer, Stephen K. (15 October 2006). "Developmental Dysplasia of the Hip". American Family Physician. 74 (8): 1310–1316. PMID 17087424. Archived from the original on 16 October 2008. Retrieved 19 April 2008.
- "Dr. Rose's Peripheral Brain--DEVELOPMENTAL DYSPLASIA OF THE HIP". faculty.washington.edu. Archived from the original on 10 June 2017. Retrieved 22 April 2008.
- Dietz, Frederick R.; Speer, Linda (1 July 1999). "Screening for Developmental Dysplasia of the Hip". American Family Physician. 60 (1): 177–84, 187–8. PMID 10414637. Archived from the original on 6 July 2008. Retrieved 14 April 2008.
- "eMedicine - Developmental Dysplasia of the Hip : Article by James McCarthy, MD, FAAOS". 20 October 2019.
{{cite journal}}: Cite journal requires|journal=(help) - "Ultrasound Detection of DDH - International Hip Dysplasia Institute". Archived from the original on 4 December 2020. Retrieved 31 August 2012.
- "X-Ray Screening for Developmental Dysplasia of the Hip - International Hip Dysplasia Institute". Archived from the original on 4 December 2020. Retrieved 31 August 2012.
- "ACR Appropriateness Criteria - Developmental Dysplasia of the Hip (DDH)–Child". American College of Radiology. Revised 2018
- Initially largely copied from: Ruiz Santiago, Fernando; Santiago Chinchilla, Alicia; Ansari, Afshin; Guzmán Álvarez, Luis; Castellano García, Maria del Mar; Martínez Martínez, Alberto; Tercedor Sánchez, Juan (2016). "Imaging of Hip Pain: From Radiography to Cross-Sectional Imaging Techniques". Radiology Research and Practice. 2016: 1–15. doi:10.1155/2016/6369237. ISSN 2090-1941. PMC 4738697. PMID 26885391. Attribution 4.0 International (CC BY 4.0) license
- "Pavlik Harness". Archived from the original on 22 October 2020. Retrieved 31 August 2012.
- Czubak J, Piontek T, Niciejewski K, Magnowski P, Majek M, Płończak M (2004). "Retrospective analysis of the non-surgical treatment of developmental dysplasia of the hip using Pavlik harness and Fredjka pillow: comparison of both methods". Ortop Traumatol Rehabil. 6 (1): 9–13. PMID 17676003.
- Fleischman, Andrew N.; Rothman, Richard H.; Parvizi, Javad (April 2018). "Femoral Nerve Palsy". The Journal of Arthroplasty. 33 (4): 1194–1199. doi:10.1016/j.arth.2017.10.050. PMID 29239773.
- Nakamura J, Kamegaya M, Saisu T, Someya M, Koizumi W, Moriya H (2007). "Treatment for developmental dysplasia of the hip using the Pavlik harness: long-term results". J Bone Joint Surg Br. 89 (2): 230–5. doi:10.1302/0301-620X.89B2.18057. PMID 17322441. Archived from the original on 24 December 2012.
- "Hip Spica Cast for Developmental Dysplasia of the Hip". Archived from the original on 4 December 2020. Retrieved 31 August 2012.
- "Traction with DDH Treatment". Archived from the original on 4 December 2020. Retrieved 31 August 2012.
- Lau EM, Lin F, Lam D, Silman A, Croft P (1995). "Hip osteoarthritis and dysplasia in Chinese men". Ann. Rheum. Dis. 54 (12): 965–9. doi:10.1136/ard.54.12.965. PMC 1010061. PMID 8546528.
- Lievense AM, Bierma-Zeinstra SM, Verhagen AP, Verhaar JA, Koes BW (2004). "Influence of hip dysplasia on the development of osteoarthritis of the hip". Ann. Rheum. Dis. 63 (6): 621–6. doi:10.1136/ard.2003.009860. PMC 1755018. PMID 15140766.
- Sutherland, Denise; West, Sophie (2011). A Guide for Adults with Hip Dysplasia. Lulu.com. pp. 56–59. ISBN 978-0-9872152-0-8.
- Bialik V, Bialik GM, Blazer S, Sujov P, Wiener F, Berant M (1999). "Developmental dysplasia of the hip: a new approach to incidence". Pediatrics. 103 (1): 93–9. doi:10.1542/peds.103.1.93. PMID 9917445. S2CID 1595498.
- Kokavec M, Bialik V (2007). "Developmental dysplasia of the hip. Prevention and real incidence". Bratisl Lek Listy. 108 (6): 251–4. PMID 17972535.
- Developmental Dysplasia of the Hip at eMedicine
- "UNSW Embryology- Musculoskeletal System - Abnormalities". Archived from the original on 9 April 2008. Retrieved 19 April 2008.
- "ER - Out on a Limb (2006)". IMDb. Retrieved 31 August 2012.
- Ettinger, Stephen J.; Feldman, Edward C. (1995). Textbook of Veterinary Internal Medicine (4th ed.). W. B. Saunders Company. ISBN 0-7216-6795-3.