Hallermann–Streiff syndrome
Hallermann–Streiff syndrome is a congenital disorder that affects growth, cranial development, hair-growth, and dental development. There are fewer than 200 people with the syndrome worldwide. One notable organization that is supporting people with Hallermann–Streiff syndrome is the Germany-based "Schattenkinder e.V".[1]
| Hallermann–Streiff syndrome | |
|---|---|
| Other names | Oculomandibulofacial syndrome, François dyscephalic syndrome, Hallermann–Streiff–François syndrome, oculomandibulodyscephaly with hypotrichosis, Aubry syndrome, Ullrich–Fremery-Dohna syndrome |
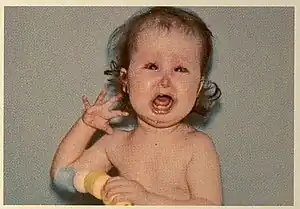 | |
| Girl with Hallermann-Streiff syndrome | |
| Specialty | Medical genetics |
Presentation
Patients with this syndrome are shorter than the average person and may not develop hair in many places, including in the facial, leg and pubic areas. Patients also have eye problems including reduced eye size, bilateral cataracts[2] and glaucoma. The syndrome can be associated with sleep apnea.[3] The physical characteristics of the syndrome can result in difficult intubation by medical professionals.[4] Intelligence is usually normal.[5]
Cause
The genetic cause of Hallermann–Streiff syndrome has not been conclusively determined. It is most likely due to a de novo mutation,[6] and it may be associated with the GJA1 gene.[7]
Diagnosis
Diagnosis is based on the physical characteristics and symptoms.[5] There is no established clinical genetic testing for Hallermann–Streiff syndrome, however some laboratories offer research genetic testing for the condition.[6]
Treatment
There is no cure for Hallermann–Streiff syndrome. Treatments center around the particular symptoms in each individual. Early measures are based around ensuring proper breathing and intake of nutrients and may include a tracheostomy. Early surgery for cataracts may be recommended, however some studies have suggested that spontaneous resolution of cataracts occurs in up to 50% of untreated patients. Regular visits to an ophthalmologist to monitor and deal with other eye problems, some of which may require surgery, are strongly recommended.[6]
Management of the condition may also include surgical reconstruction of certain craniofacial malformations (particularly in the mandibular and nasal region) at an appropriate age. Additionally, management for certain heart defects, such as medication or surgery, may be needed.[6]
History
It is named after German ophthalmologist Wilhelm Hallermann (1909–2005) and Italian–Swiss ophthalmologist Enrico Bernardo Streiff (1908–1988),[8][9][10] who first described the syndrome in 1948 and 1950 respectively.[11]
References
- "Herzlich willkommen!". schattenkinder.info. Retrieved 2020-05-07.
- Ertekin V, Selimoğlu MA, Selimoğlu E (2004). "Non-lethal Hallermann-Streiff syndrome with bone fracture: report of a case". Ann. Genet. 47 (4): 387–91. doi:10.1016/j.anngen.2004.03.005. PMID 15581837.
- Shiomi T, Guilleminault C, Izumi H, Yamada S, Murata K, Kobayashi T (October 1999). "Obstructive sleep apnoea in a puerperal patient with Hallermann-Streiff syndrome". Eur. Respir. J. 14 (4): 974–7. doi:10.1034/j.1399-3003.1999.14d42.x. PMID 10573253.
- Malde AD, Jagtap SR, Pantvaidya SH (1994). "Hallermann-Streiff syndrome: airway problems during anaesthesia". J Postgrad Med. 40 (4): 216–8. PMID 9136243.
- "Hallermann-Streiff syndrome - Natural Living Center". www.naturallivingcenter.net. Archived from the original on 2018-03-06. Retrieved 2018-03-05.
- "Hallermann-Streiff syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Retrieved 2018-03-05.
- Pizzuti A, Flex E, Mingarelli R, Salpietro C, Zelante L, Dallapiccola B (March 2004). "A homozygous GJA1 gene mutation causes a Hallermann-Streiff/ODDD spectrum phenotype". Hum. Mutat. 23 (3): 286. doi:10.1002/humu.9220. PMID 14974090.
- synd/1767 at Who Named It?
- W. Hallermann. Vogelgesicht und Cataracta congenita. Klinische Monatsblätter für Augenheilkunde, Stuttgart, 1948, 113: 315–318.
- E. B. Streiff. Dysmorphie mandibulo-faciale (tête d’oiseau) et alterations oculaires. Ophthalmologica, Basel, 1950, 120: 79–83.
- Wynbrandt, James; Ludman, Mark D. (2010-05-12). The Encyclopedia of Genetic Disorders and Birth Defects. Infobase Publishing. p. 185. ISBN 9781438120959.
12. Shandilya VK, Parmar LD, Shandilya AV. Functional ambulation with bent knee prostheses for an adult with bilateral 90 degrees knee flexion contractures—A case report. J Family Med Prim Care [serial online] 2020 [cited 2020 Jun 2];9:2492-5. Available from: http://www.jfmpc.com/text.asp?2020/9/5/2492/285055