Granulomatous amoebic encephalitis
Granulomatous amoebic encephalitis (GAE)[2] is a rare, usually fatal, subacute-to-chronic central nervous system disease caused by certain species of free-living amoebae[3] of the genera Acanthamoeba, Balamuthia and Sappinia.[4][5] The term is most commonly used with Acanthamoeba. In more modern references, the term "balamuthia amoebic encephalitis" (BAE) is commonly used when Balamuthia mandrillaris is the cause.[6][7][8][9]
| Granulomatous amoebic encephalitis | |
|---|---|
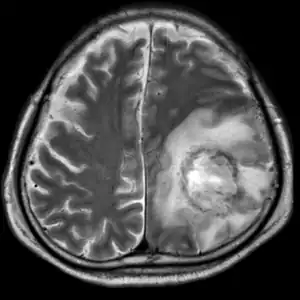 | |
| T2-weighted MRI showing liquefied, necrotic brain tissue as a result of GAE caused by an infection of Acanthamoeba, genotype T18 | |
| Specialty | Infectious diseases |
| Symptoms | Fever, headaches, personality changes[1] |
| Complications | seizures, coma |
| Causes | Acanthamoeba, Balamuthia mandrillaris, and Sappinia pedata |
.png.webp)
B: T1-weighted MRI showing expansion and addition of necrotic areas 4 days later
Symptoms and signs
GAE starts slowly, with symptoms like headache, nausea, dizziness, irritability and a low-grade fever. The CNS symptoms depend on the part of the brain that is infected. Changes in behavior are an important sign. Other CNS signs may include seizures, focal neurologic signs, diplopia (double vision), cranial nerve palsies, ataxia, confusion, and personality changes.[1]
Some of the symptoms may mimic glioma (especially brainstem glioma), or other brain diseases, which may hamper timely diagnosis. The symptoms are caused by inflammatory necrosis of brain tissue brought on by compounds released from the organisms.
Diagnosis
The condition can be difficult for doctors to diagnose, because it is a rare disease.[10] A brain biopsy will reveal the presence of infection by pathogenic amoebas. In GAE, these present as general inflammation and sparse granules. On microscopic examination, infiltrates of amoebic cysts and/or trophozoites will be visible.[11]
Treatment
Acanthamoeba
Antifungal drugs including ketoconazole, miconazole, 5-flucytosine and pentamidine have been shown to be effective against Acanthamoeba in vitro.[12]
Balamuthia
Like with Acanthamoeba, infection of the brain with this organism rapidly turns fatal in most cases.[13] However some survivors have been reported:
Two patients survived after being successfully treated with a therapy consisting of flucytosine, pentamidine, fluconazole, sulfadiazine, and azithromycin. Thioridazine or trifluoperazine was also given. Successful treatment in these cases was credited to "awareness of Balamuthia as the causative agent of encephalitis and early initiation of antimicrobial therapy."[14]
In one case, cloxacillin, ceftriaxone, and amphotericin B were tried, but this treatment protocol did not prove effective.[15]
In 2018 a metagenomic sequencing analysis identified Nitroxoline as amoebicidal agent against the Balamuthia mandrillaris.[16]
In 2021 a patient recovered after treatment with nitroxoline.[17][18] The man had been given a recommended drug therapy (pentamidine, sulfadiazine, azithromycin/clarithromycin, fluconazole, flucytosine, and miltefosine) but progressed negatively. Therefore with the permission of the FDA the regime was complemented with the unapproved drug. Nitroxoline had previously been identified via a clinical metagenomic next-generation sequencing analysis to be a compound that could be repurposed as an amoebicidal agent against Balamuthia mandrillaris.[16] The cerebral lesion shrank only one week later and the man later recovered.
Prognosis
Even with treatment, CNS infection with Acanthamoeba is often fatal, and there are very few recorded survivors, almost all of whom had permanent neurocognitive deficits.[12] The prognosis is largely influenced by the time of diagnosis, how virulent and sensitive the Acanthamoeba strain is, and, most crucially, the immune status of the affected person. Due to it commonly being an opportunistic infection, the prognosis is generally poor, with a mortality rate approaching 90%.[1]
Sappinia pedata can cause GAE, however only one case of GAE due to S. pedata infection has ever been reported, and the patient survived without any long-term consequences.[19]
See also
- Naegleriasis, an almost invariably fatal infection of the brain by the percolozoan Naegleria fowleri
References
- Duggal SD, Rongpharpi SR, Duggal AK, Kumar A, Biswal I (2018-01-22). "Role of Acanthamoeba in Granulomatous Encephalitis: A Review". Journal of Infectious Diseases & Immune Therapies. 2017.
- Sarica FB, Tufan K, Cekinmez M, Erdoğan B, Altinörs MN (July 2009). "A rare but fatal case of granulomatous amebic encephalitis with brain abscess: the first case reported from Turkey". Turkish Neurosurgery. 19 (3): 256–259. PMID 19621290.
- Nguyen L, Perloff S (2018-07-24). Steele RW (ed.). "Amebic Meningoencephalitis: Overview". EMedicine.
- Guarner J, Bartlett J, Shieh WJ, Paddock CD, Visvesvara GS, Zaki SR (December 2007). "Histopathologic spectrum and immunohistochemical diagnosis of amebic meningoencephalitis". Modern Pathology. 20 (12): 1230–1237. doi:10.1038/modpathol.3800973. PMID 17932496.
- Jayasekera S, Sissons J, Tucker J, Rogers C, Nolder D, Warhurst D, et al. (October 2004). "Post-mortem culture of Balamuthia mandrillaris from the brain and cerebrospinal fluid of a case of granulomatous amoebic meningoencephalitis, using human brain microvascular endothelial cells". Journal of Medical Microbiology. 53 (Pt 10): 1007–1012. doi:10.1099/jmm.0.45721-0. PMID 15358823.
- da Rocha-Azevedo B, Tanowitz HB, Marciano-Cabral F (2009). "Diagnosis of infections caused by pathogenic free-living amoebae". Interdisciplinary Perspectives on Infectious Diseases. 2009: 251406. doi:10.1155/2009/251406. PMC 2719787. PMID 19657454.
- Matin A, Siddiqui R, Jung SY, Kim KS, Stins M, Khan NA (August 2007). "Balamuthia mandrillaris interactions with human brain microvascular endothelial cells in vitro". Journal of Medical Microbiology. 56 (Pt 8): 1110–1115. doi:10.1099/jmm.0.47134-0. PMID 17644721.
- Siddiqui R, Khan NA (February 2008). "Balamuthia amoebic encephalitis: an emerging disease with fatal consequences". Microbial Pathogenesis. 44 (2): 89–97. doi:10.1016/j.micpath.2007.06.008. PMID 17913450.
- Schuster FL, Yagi S, Gavali S, Michelson D, Raghavan R, Blomquist I, et al. (April 2009). "Under the radar: balamuthia amebic encephalitis". Clinical Infectious Diseases. 48 (7): 879–887. doi:10.1086/597260. PMID 19236272.
- Matsui T, Maeda T, Kusakabe S, Arita H, Yagita K, Morii E, Kanakura Y (May 2018). "A case report of granulomatous amoebic encephalitis by Group 1 Acanthamoeba genotype T18 diagnosed by the combination of morphological examination and genetic analysis". Diagnostic Pathology. 13 (1): 27. doi:10.1186/s13000-018-0706-z. PMC 5943995. PMID 29747695.
- Kofman A, Guarner J (January 2022). "Infections Caused by Free-Living Amoebae". Journal of Clinical Microbiology. 60 (1): e0022821. doi:10.1128/JCM.00228-21. PMC 8769735. PMID 34133896.
- Wang J, Nichols L, Martinez AJ. "Final Diagnosis -- Granulomatous Amoebic Encephalitis Due to Acanthamoeba castellanii". Department of Pathology. University of Pittsburgh.
- Akpek G, Uslu A, Huebner T, Taner A, Rapoport AP, Gojo I, et al. (August 2011). "Granulomatous amebic encephalitis: an under-recognized cause of infectious mortality after hematopoietic stem cell transplantation". Transplant Infectious Disease. 13 (4): 366–373. doi:10.1111/j.1399-3062.2011.00612.x. PMID 21338461. S2CID 31162954.
- Deetz TR, Sawyer MH, Billman G, Schuster FL, Visvesvara GS (November 2003). "Successful treatment of Balamuthia amoebic encephalitis: presentation of 2 cases". Clinical Infectious Diseases. 37 (10): 1304–1312. doi:10.1086/379020. PMID 14583863.
- Intalapaporn P, Suankratay C, Shuangshoti S, Phantumchinda K, Keelawat S, Wilde H (June 2004). "Balamuthia mandrillaris meningoencephalitis: the first case in southeast Asia". The American Journal of Tropical Medicine and Hygiene. 70 (6): 666–669. doi:10.4269/ajtmh.2004.70.666. PMID 15211011.
- Laurie, Matthew T.; White, Corin V.; Retallack, Hanna; Wu, Wesley; Moser, Matthew S.; Sakanari, Judy A.; Ang, Kenny; Wilson, Christopher; Arkin, Michelle R.; DeRisi, Joseph L.; Bassler, Bonnie (2018). "Functional Assessment of 2,177 U.S. and International Drugs Identifies the Quinoline Nitroxoline as a Potent Amoebicidal Agent against the Pathogen Balamuthia mandrillaris". mBio. 9 (5). doi:10.1128/mBio.02051-18. ISSN 2150-7511. PMC 6212833. PMID 30377287.
- Kornei, Katherine. "Repurposed drug battles 'brain-eating' amoeba". Science. Retrieved 10 February 2023.
- Spottiswoode, Natasha; Pet, Douglas; Kim, Annie; Gruenberg, Katherine; Shah, Maulik; Ramachandran, Amrutha; Laurie, Matthew T; Zia, Maham; Fouassier, Camille; Boutros, Christine L; Lu, Rufei; Zhang, Yueyuan; Servellita, Venice; Bollen, Andrew; Chiu, Charles Y; Wilson, Michael R; Valdivia, Liza; DeRisi, Joseph L (2023). "Successful Treatment of Balamuthia mandrillaris Granulomatous Amebic Encephalitis with Nitroxoline". Emerging Infectious Diseases. 29 (1): 197–201. doi:10.3201/eid2901.221531. PMC 9796214.
- "Sappinia - Frequently Asked Questions (FAQs)". U.S. Centers for Disease Control and Prevention. Archived from the original on 2011-10-18.