Pancreatic beta cell function
Pancreatic beta cell function (synonyms Gβ or, if calculated from fasting concentrations of insulin and glucose, HOMA-Beta or SPINA-GBeta) is one of the preconditions of euglycaemia, i.e. normal blood sugar regulation. It is defined as insulin secretory capacity, i.e. the maximum amount of insulin to be produced by beta cells in a given unit of time.
| Pancreatic beta cell function | |
|---|---|
| Other names | Gβ, HOMA-Beta, IGI, SPINA-GBeta |
| Specialty | Endocrinology |
Physiology and pathophysiology
Beta cells play a paramount role in glucose homeostasis. Progressive loss of insulin secretory capacity is a key defect associated with the transition from a healthy glycaemic state to hyperglycaemia, characteristic of untreated diabetes mellitus. In type 1 diabetes mellitus and pancreatogenic diabetes beta cell destruction is a primary event from the perspective of the feedback loop. In type 2 diabetes beta cell dysfunction is an essential constituent as well,[1] but subsequent to the development of insulin resistance.[2][3] Other mechanisms, including lipotoxicity, amyloid deposition, oxidative stress, mitochondrial dysfunction, ER stress and inflammation may be involved as well.[4][3] The beta cell loss in type 2 diabetes is mainly caused by reduced beta cell number rather than size.[5] Hyperglycaemia becomes clinically significant once insulin over-secretion can no longer compensate for the degree of insulin resistance.[2][4][1]
Assessing beta cell function
Measuring beta-cell function is a challenge, since insulin secretory capacity cannot be readily assessed. Therefore, indirect methods of measurement have been developed. They include dynamic and static function tests.[6][7]
Single-point measurements
One-time measurements of certain hormones or metabolites provide some limited information. Examples are:
- Fasting glucose concentration
- Fasting or random C-peptide concentration
Although single-point measurements have the benefit of being convenient and inexpensive, they are generally not regareded as sufficiently informative for early diagnosis of impaired glucose homeostasis or early-stage type 1 diabetes.[8]
Dynamic function tests
Dynamic function tests for beta-cell function include:
- Oral glucose tolerance testing (OGTT)
- Intravenous glucose tolerance tests (IVGTT)
- Meal tolerance tests
- Hyperglycaemic clamp
Challenges and limits
Measuring beta-cell function requires the rate of secretion to be interpreted in relation to the prevailing glucose concentration.[13] Therefore, a mathematical model is needed that links the time courses of insulin secretion and glucose concentration as a mechanistic causal relationship.[14][8]
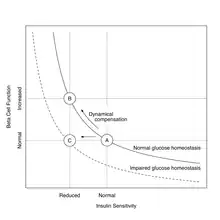
Additionally, beta-cell function has to be interpreted in light of the prevailing insulin sensitivity.[14][13] This is necessary since the beta cell mass is adjusted as required by dynamical compensation,[15] giving rise to a hyperbolic relationship between insulin sensitivity and beta cell function.[4][7][1][12] In the state of insulin resistance beta cells proliferate and their secretory capacity subsequently rises. One possibility to address this relation is to resort to a normalization of beta cell function based on a disposition metric.[13] The disposition index, calculated as product of insulin sensitivity and beta cell function, is assumed to be a constant during the development of insulin resistance. It is generally assumed that the glucose tolerance of an individual is related to the disposition index. In this model, different values of glucose tolerance are represented by different hyperbolas, so that within one hyperbola the product of insulin sensitivity and beta cell function remains a constant.
In summary, to provide a meaningful mechanistic explanation of insulin-glucose homeostasis, beta cell function and insulin sensitivity have to be assessed simultaneously and it is necessary to interpret all observations in the context of insulin sensitivity[16] or resistance.[2]
References
- Weir, GC; Gaglia, J; Bonner-Weir, S (March 2020). "Inadequate β-cell mass is essential for the pathogenesis of type 2 diabetes". The Lancet. Diabetes & Endocrinology. 8 (3): 249–256. doi:10.1016/S2213-8587(20)30022-X. PMC 7098467. PMID 32006519. S2CID 211004857.
- Cersosimo, E; Solis-Herrera, C; Trautmann, ME; Malloy, J; Triplitt, CL (January 2014). "Assessment of pancreatic β-cell function: review of methods and clinical applications". Current Diabetes Reviews. 10 (1): 2–42. doi:10.2174/1573399810666140214093600. PMC 3982570. PMID 24524730.
- Wysham, C; Shubrook, J (November 2020). "Beta-cell failure in type 2 diabetes: mechanisms, markers, and clinical implications". Postgraduate Medicine. 132 (8): 676–686. doi:10.1080/00325481.2020.1771047. PMID 32543261. S2CID 219705786.
- Saisho, Y (15 February 2015). "β-cell dysfunction: Its critical role in prevention and management of type 2 diabetes". World Journal of Diabetes. 6 (1): 109–24. doi:10.4239/wjd.v6.i1.109. PMC 4317303. PMID 25685282. S2CID 7631395.
- Sasaki, H; Saisho, Y; Inaishi, J; Watanabe, Y; Tsuchiya, T; Makio, M; Sato, M; Nishikawa, M; Kitago, M; Yamada, T; Itoh, H (August 2021). "Reduced beta cell number rather than size is a major contributor to beta cell loss in type 2 diabetes". Diabetologia. 64 (8): 1816–1821. doi:10.1007/s00125-021-05467-7. PMC 8245378. PMID 33938968. S2CID 233479427.
- Choi, CS; Kim, MY; Han, K; Lee, MS (March 2012). "Assessment of β-cell function in human patients". Islets. 4 (2): 79–83. doi:10.4161/isl.19270. PMID 22627463. S2CID 29265470.
- Hannon, TS; Kahn, SE; Utzschneider, KM; Buchanan, TA; Nadeau, KJ; Zeitler, PS; Ehrmann, DA; Arslanian, SA; Caprio, S; Edelstein, SL; Savage, PJ; Mather, KJ; RISE, Consortium (January 2018). "Review of methods for measuring β-cell function: Design considerations from the Restoring Insulin Secretion (RISE) Consortium". Diabetes, Obesity & Metabolism. 20 (1): 14–24. doi:10.1111/dom.13005. hdl:1805/13697. PMC 6095472. PMID 28493515. S2CID 30114663.
- Galderisi, A; Carr, ALJ; Martino, M; Taylor, P; Senior, P; Dayan, C (15 September 2023). "Quantifying beta cell function in the preclinical stages of type 1 diabetes". Diabetologia. doi:10.1007/s00125-023-06011-5. PMID 37712956.
- Li, X; Zhang, F; Chen, H; Yu, H; Zhou, J; Li, M; Li, Q; Li, L; Yin, J; Liu, F; Bao, Y; Han, J; Jia, W (30 January 2017). "Diagnosis of insulinoma using the ratios of serum concentrations of insulin and C-peptide to glucose during a 5-hour oral glucose tolerance test". Endocrine Journal. 64 (1): 49–57. doi:10.1507/endocrj.EJ16-0292. PMID 27725372.
- Nauck, MA; Meier, JJ (4 December 2012). "Diagnostic accuracy of an "amended" insulin-glucose ratio for the biochemical diagnosis of insulinomas". Annals of Internal Medicine. 157 (11): 767–75. doi:10.7326/0003-4819-157-11-201212040-00004. PMID 23208166. S2CID 27336701.
- Matthews, DR; Hosker, JP; Rudenski, AS; Naylor, BA; Treacher, DF; Turner, RC (July 1985). "Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man". Diabetologia. 28 (7): 412–9. doi:10.1007/BF00280883. PMID 3899825. S2CID 24872571.
- Dietrich, JW; Dasgupta, R; Anoop, S; Jebasingh, F; Kurian, ME; Inbakumari, M; Boehm, BO; Thomas, N (21 October 2022). "SPINA Carb: a simple mathematical model supporting fast in-vivo estimation of insulin sensitivity and beta cell function". Scientific Reports. 12 (1): 17659. Bibcode:2022NatSR..1217659D. doi:10.1038/s41598-022-22531-3. PMC 9587026. PMID 36271244. S2CID 253041870.
- Cobelli, C; Toffolo, GM; Dalla Man, C; Campioni, M; Denti, P; Caumo, A; Butler, P; Rizza, R (July 2007). "Assessment of beta-cell function in humans, simultaneously with insulin sensitivity and hepatic extraction, from intravenous and oral glucose tests". American Journal of Physiology. Endocrinology and Metabolism. 293 (1): E1–E15. doi:10.1152/ajpendo.00421.2006. PMID 17341552.
- Ferrannini, E; Mari, A (May 2004). "Beta cell function and its relation to insulin action in humans: a critical appraisal". Diabetologia. 47 (5): 943–56. doi:10.1007/s00125-004-1381-z. PMID 15105990. S2CID 23061377.
- Karin, O; Swisa, A; Glaser, B; Dor, Y; Alon, U (8 November 2016). "Dynamical compensation in physiological circuits". Molecular Systems Biology. 12 (11): 886. doi:10.15252/msb.20167216. PMC 5147051. PMID 27875241. S2CID 2643944.
- Ahrén, B; Pacini, G (February 2004). "Importance of quantifying insulin secretion in relation to insulin sensitivity to accurately assess beta cell function in clinical studies". European Journal of Endocrinology. 150 (2): 97–104. doi:10.1530/eje.0.1500097. PMID 14763905.