Tetracycline antibiotics
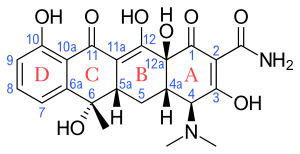
Tetracyclines are a group of broad-spectrum antibiotic compounds that have a common basic structure and are either isolated directly from several species of Streptomyces bacteria or produced semi-synthetically from those isolated compounds.[1] Tetracycline molecules comprise a linear fused tetracyclic nucleus (rings designated A, B, C and D) to which a variety of functional groups are attached.[2] Tetracyclines are named after their four ("tetra-") hydrocarbon rings ("-cycl-") derivation ("-ine"). They are defined as a subclass of polyketides, having an octahydrotetracene-2-carboxamide skeleton and are known as derivatives of polycyclic naphthacene carboxamide.[3] While all tetracyclines have a common structure, they differ from each other by the presence of chloro, methyl, and hydroxyl groups. These modifications do not change their broad antibacterial activity, but do affect pharmacological properties such as half-life and binding to proteins in serum.[1]
Tetracyclines were discovered in the 1940s and exhibited activity against a wide range of microorganisms including gram-positive and gram-negative bacteria, chlamydiota, mycoplasmatota, rickettsiae, and protozoan parasites.[2] Tetracycline itself was discovered later than chlortetracycline and oxytetracycline but is still considered as the parent compound for nomenclature purposes.[4] Tetracyclines are among the cheapest classes of antibiotics available and have been used extensively in prophylaxis and in treatment of human and animal infections, as well as at subtherapeutic levels in animal feed as growth promoters.[2]
Tetracyclines are growth inhibitors (bacteriostatic) rather than killers of the infectious agent (bacteriocidal) and are only effective against multiplying microorganisms.[1] They are short-acting and passively diffuse through porin channels in the bacterial membrane. They inhibit protein synthesis by binding reversibly to the bacterial 30S ribosomal subunit and preventing the aminoacyl tRNA from binding to the A site of the ribosome. They also bind to some extent the bacterial 50S ribosomal subunit and may alter the cytoplasmic membrane causing intracellular components to leak from bacterial cells.
Tetracyclines all have the same antibacterial spectrum, although there are differences in species' sensitivity to types of tetracyclines. Tetracyclines inhibit protein synthesis in both bacterial and human cells. Bacteria have a system that allows tetracyclines to be transported into the cell, whereas human cells do not. Human cells therefore are spared the effects of tetracycline on protein synthesis.[1]
Tetracyclines retain an important role in medicine, although their usefulness has been reduced with the onset of antibiotic resistance.[2] Tetracyclines remain the treatment of choice for some specific indications.[2] Because not all of the tetracycline administered orally is absorbed from the gastrointestinal tract, the bacterial population of the intestine can become resistant to tetracyclines, resulting in overgrowth of resistant organisms. The widespread use of tetracyclines is thought to have contributed to an increase in the number of tetracycline-resistant organisms, in turn rendering certain infections more resilient to treatment.[1] Tetracycline resistance is often due to the acquisition of new genes, which code for energy-dependent efflux of tetracyclines or for a protein that protects bacterial ribosomes from the action of tetracyclines. Furthermore, a limited number of bacteria acquire resistance to tetracyclines by mutations.[2][5]
Medical uses
Tetracyclines are generally used in the treatment of infections of the urinary tract, respiratory tract, and the intestines and are also used in the treatment of chlamydia, especially in patients allergic to β-lactams and macrolides; however, their use for these indications is less popular than it once was due to widespread development of resistance in the causative organisms.[6][7] Tetracyclines are widely used in the treatment of moderately severe acne and rosacea (tetracycline, oxytetracycline, doxycycline or minocycline).[8] Anaerobic bacteria are not as susceptible to tetracyclines as are aerobic bacteria.[9] Doxycycline is also used as a prophylactic treatment for infection by Bacillus anthracis (anthrax) and is effective against Yersinia pestis, the infectious agent of bubonic plague. It is also used for malaria treatment and prophylaxis, as well as treating elephantitis filariasis.[10] Tetracyclines remain the treatment of choice for infections caused by chlamydia (trachoma, psittacosis, salpingitis, urethritis and L. venereum infection), Rickettsia (typhus, Rocky Mountain spotted fever), brucellosis and spirochetal infections (Lyme disease/borreliosis and syphilis).[2] They are also used in veterinary medicine.[2] They may have a role in reducing the duration and severity of cholera, although drug-resistance is mounting[11] and their effect on overall mortality is questioned.[12]
Side effects
Side-effects from tetracyclines are not common, but of particular note is phototoxicity. It increases the risk of sunburn under exposure to light from the sun or other sources. This may be of particular importance for those intending to take on vacations long-term doxycycline as a malaria prophylaxis. They may cause stomach or bowel upsets, and, on rare occasions, allergic reactions. Very rarely, severe headache and vision problems may be signs of dangerous secondary intracranial hypertension, also known as idiopathic intracranial hypertension. Tetracyclines are teratogens due to the likelihood of causing teeth discolouration in the fetus as they develop in infancy. For this same reason, tetracyclines are contraindicated for use in children under 8 years of age. Some adults also experience teeth discoloration (mild grey hue) after use. They are, however, safe to use in the first 18 weeks of pregnancy.[13][14] Some patients taking tetracyclines require medical supervision because they can cause steatosis and liver toxicity.[15][16][17]
Cautions
Tetracyclines should be used with caution by those with liver impairment. Also, because the molecules are soluble in water it can worsen kidney failure (this is not true of the lipid-soluble agents doxycycline and minocycline). They may increase muscle weakness in myasthenia gravis and exacerbate systemic lupus erythematosus. Antacids containing aluminium and calcium reduce the absorption of all tetracyclines, and dairy products reduce absorption greatly for all but minocycline. The breakdown products of tetracyclines are toxic and can cause Fanconi syndrome, a potentially fatal disease affecting proximal tubular function in the nephrons of the kidney. Prescriptions of these drugs should be discarded once expired because they can cause hepatotoxicity. It was once believed that tetracycline antibiotics impair the effectiveness of many types of hormonal contraception. Recent research has shown no significant loss of effectiveness in oral contraceptives while using most tetracyclines. Despite these studies, many physicians still recommend the use of barrier contraception for people taking any tetracyclines to prevent unwanted pregnancy.[18][19][20]
Contraindications
Tetracycline use should be avoided in pregnant or lactating women, and in children with developing teeth because they may result in permanent staining (dark yellow-gray teeth with a darker horizontal band that goes across the top and bottom rows of teeth), and possibly affect the growth of teeth and bones. Usage during the first 12 weeks of pregnancy does not appear to increase the risk of any major birth defects.[21] There may be a small increased risk for minor birth defects such as an inguinal hernia, but the number of reports is too small to be sure if there actually is any risk.[21] In tetracycline preparation, stability must be considered in order to avoid formation of toxic epi-anhydrotetracyclines.
Mechanism of action
Tetracycline antibiotics are protein synthesis inhibitors.[22] They inhibit the initiation of translation in variety of ways by binding to the 30S ribosomal subunit, which is made up of 16S rRNA and 21 proteins. They inhibit the binding of aminoacyl-tRNA to the mRNA translation complex. Some studies have shown that tetracyclines may bind to both 16S and 23S rRNAs.[23] Tetracyclines also have been found to inhibit matrix metalloproteinases. This mechanism does not add to their antibiotic effects, but has led to extensive research on chemically modified tetracyclines or CMTs (like incyclinide) for the treatment of rosacea, acne, diabetes and various types of neoplasms.[24][25][26] It has been shown that tetracyclines are not only active against broad spectrum of bacteria, but also against viruses, protozoa that lack mitochondria and some noninfectious conditions. The binding of tetracyclines to cellular dsRNA (double stranded RNA) may be an explanation for their wide range of effect. It can also be attributed to the nature of ribosomal protein synthesis pathways among bacteria.[23] Incyclinide was announced to be ineffective for rosacea in September 2007.[27] Several trials have examined modified and unmodified tetracyclines for the treatment of human cancers; of those, very promising results were achieved with CMT-3 for patients with Kaposi Sarcoma.[28]
Structure-activity relationship
Tetracyclines are composed of a rigid skeleton of 4 fused rings.[2] The rings structure of tetracyclines is divided into an upper modifiable region and a lower non modifiable region.[29][30] An active tetracycline requires a C10 phenol as well as a C11-C12 keto-enol substructure in conjugation with a 12a-OH group and a C1-C3 diketo substructure.[2][30][29] Removal of the dimethylamine group at C4 reduces antibacterial activity.[30][29] Replacement of the carboxylamine group at C2 results in reduced antibacterial activity but it is possible to add substituents to the amide nitrogen to get more soluble analogs like the prodrug lymecycline.[2] The simplest tetracycline with measurable antibacterial activity is 6-deoxy-6-demethyltetracycline and its structure is often considered to be the minimum pharmacophore for the tetracycle class of antibiotics.[2][31] C5-C9 can be modified to make derivatives with varying antibacterial activity.[30][29]
Mechanism of resistance
Cells can become resistant to tetracycline by enzymatic inactivation of tetracycline, efflux, ribosomal protection,[2] reduced permeability and ribosome mutation.[5]
Inactivation is the rarest type of resistance,[32] where NADPH-dependent oxidoreductase, a class of antibiotic destructase, modifies the tetracycline antibiotic at their oxidative soft spot leading to an inactivation of the tetracycline antibiotic. For example, the oxireductase makes a modification on the C11a site of oxytetracycline. Both Mg2+ chelation and ribosome binding are required for the biological activity of oxytetracycline and the modification attenuate the binding, leading to inactivation of the oxytetracycline antibiotic.[5]
In the most common mechanism of reaction, efflux,[23] various resistance genes encode a membrane protein that actively pumps tetracycline out of the cell by exchanging a proton for a tetracycline cation complex. This exchange leads to a reduced cytoplasmic concentration of tetracycline.[33]
In ribosomal protection, a resistance gene encodes a protein that can have several effects, depending on what gene is transferred.[34] Twelve classes of ribosomal protection genes/proteins have been found.[35]
Possible mechanisms of action of these protective proteins include:
Administration
When ingested, it is usually recommended that the more water-soluble, short-acting tetracyclines (plain tetracycline, chlortetracycline, oxytetracycline, demeclocycline and methacycline) be taken with a full glass of water, either two hours after eating or two hours before eating. This is partly because most tetracyclines bind with food and also easily with magnesium, aluminium, iron and calcium, which reduces their ability to be completely absorbed by the body. Dairy products, antacids and preparations containing iron should be avoided near the time of taking the drug. Partial exceptions to these rules occur for doxycycline and minocycline, which may be taken with food (though not iron, antacids, or calcium supplements). Minocycline can be taken with dairy products because it does not chelate calcium as readily, although dairy products do decrease absorption of minocycline slightly.[39]
History
The history of the tetracyclines involves the collective contributions of thousands of dedicated researchers, scientists, clinicians, and business executives. Tetracyclines were discovered in the 1940s, first reported in scientific literature in 1948, and exhibited activity against a wide range of microorganisms. The first members of the tetracycline group to be described were chlortetracycline and oxytetracycline.[2][40] Chlortetracycline (Aureomycin) was first discovered as an ordinary item in 1945 and initially endorsed in 1948[41] by Benjamin Minge Duggar, a 73-year-old emeritus professor of botany employed by American Cyanamid – Lederle Laboratories, under the leadership of Yellapragada Subbarow. Duggar derived the substance from a Missouri soil sample, golden-colored, fungus-like, soil-dwelling bacterium named Streptomyces aureofaciens.[42] About the same time as Lederle discovered aureomycin, Pfizer was scouring the globe for new antibiotics. Soil samples were collected from jungles, deserts, mountaintops, and oceans. But ultimately Oxytetracycline (terramycin) was isolated in 1949 by Alexander Finlay from a soil sample collected on the grounds of a factory in Terre Haute, Indiana.[43] It came from a similar soil bacterium named Streptomyces rimosus.[44] From the beginning, terramycin was a molecule enveloped in controversy. It was the subject of the first mass-marketing campaign by a modern pharmaceutical company. Pfizer advertised the drug heavily in medical journals, eventually spending twice as much on marketing as it did to discover and develop terramycin. Still, it turned Pfizer, then a small company, into a pharmaceutical giant.[43] The Pfizer group, led by Francis A. Hochstein, in loose collaboration with and Robert Burns Woodward, determined the structure of oxytetracycline, enabling Lloyd H. Conover to successfully produce tetracycline itself as a synthetic product.[45] In 1955, Conover discovered that hydrogenolysis of aureomycin gives a deschloro product that is just as active as the original product. This proved for the first time that chemically modified antibiotics could have biological activity. Within a few years, a number of semisynthetic tetracyclines had entered the market, and now most antibiotic discoveries are of novel active derivatives of older compounds.[43] Other tetracyclines were identified later, either as naturally occurring molecules, e.g., tetracycline from S. aureofaciens, S. rimosus, and S. viridofaciens and dimethyl-chlortetracycline from S. aureofaciens, or as products of semisynthetic approaches, e.g., methacycline, doxycycline, and minocycline.[2][41]
Research conducted by anthropologist George J. Armelagos and his team at Emory University showed that ancient Nubians from the post-Meroitic period (around AD 350) had deposits of tetracycline in their bones, detectable through analyses of cross-sections through ultraviolet light – the deposits are fluorescent, just as are modern ones. Armelagos suggested that this was due to ingestion of the local ancient beer (very much like the Egyptian beer[46]), made from contaminated stored grains.[47]
Development
Tetracyclines were noted for their broad spectrum antibacterial activity and were commercialized with clinical success beginning in the late 1940s to the early 1950s. The second-generation semisynthetic analogs and more recent third-generation compounds show the continued evolution of the tetracycline platform towards derivatives with increased potency as well as efficacy against tetracycline-resistant bacteria, with improved pharmacokinetic and chemical properties.[40] Shortly after the introduction of tetracycline therapy, the first tetracycline-resistant bacterial pathogen was identified. Since then, tetracycline-resistant bacterial pathogens have continued to be identified, limiting tetracycline's effectiveness in treatment of bacterial disease.[48]
Glycylcyclines and fluorocyclines are new classes of antibiotics derived from tetracycline.[49][50][48] These tetracycline analogues are specifically designed to overcome two common mechanisms of tetracycline resistance, namely resistance mediated by acquired efflux pumps and/or ribosomal protection. In 2005, tigecycline, the first member of a new subgroup of tetracyclines named glycylcyclines, was introduced to treat infections that are resistant to other antimicrobials.[51] Although it is structurally related to minocycline, alterations to the molecule resulted in its expanded spectrum of activity and decreased susceptibility to the development of resistance when compared with other tetracycline antibiotics. Like minocycline, tigecycline binds to the bacterial 30S ribosome, blocking the entry of transfer RNA. This ultimately prevents protein synthesis and thus inhibiting bacterial growth. However, the addition of an N,N,-dimethylglycylamido group at the 9 position of the minocycline molecule increases the affinity of tigecycline for the ribosomal target up to 5 times when compared with minocycline or tetracycline. This allows for an expanded spectrum of activity and decreased susceptibility to the development of resistance.[48] While tigecycline was the first tetracycline approved in over 20 years, other, newer versions of tetracyclines are currently in human clinical trials.[52]
List of tetracycline antibiotics
| Antibiotic (INN) | Source[40] | Half-life[53] | Notes |
|---|---|---|---|
| Tetracycline | Naturally occurring | 6–8 hours (short) | |
| Chlortetracycline | 6–8 hours (short) | ||
| Oxytetracycline | 6–8 hours (short) | ||
| Demeclocycline | 12 hours (intermediate) | ||
| Lymecycline | Semi-synthetic | 6–8 hours (short) | |
| Meclocycline | 6–8 hours (short) | (no longer marketed) | |
| Methacycline | 12 hours (intermediate) | ||
| Minocycline | 16+ hours (long) | ||
| Rolitetracycline | 6–8 hours (short) | ||
| Doxycycline | 16+ hours (long) | ||
| Tigecycline | Glycecyclines | 16+ hours (long) | |
| Eravacycline | Newer | 16+ hours (long) | (formerly known as TP-434) received FDA approval on August 27, 2018 for treatment of complicated intra-abdominal infections.[54] |
| Sarecycline | 16+ hours (long) | (formerly known as WC 3035) received FDA approval on October 1, 2018 for treatment of moderate to severe acne vulgaris.[55] Sarecycline is a narrow-spectrum antibiotic.[56][57] | |
| Omadacycline | 16+ hours (long) | (formerly known as PTK-0796[58]) received FDA approval on October 2, 2018 for treatment of community-acquired pneumonia[59] and acute skin and skin structure infections.[60] |
Use as research reagents
Members of the tetracycline class of antibiotics are often used as research reagents in in vitro and in vivo biomedical research experiments involving bacteria as well in experiments in eukaryotic cells and organisms with inducible protein expression systems using tetracycline-controlled transcriptional activation.[61] The mechanism of action for the antibacterial effect of tetracyclines relies on disrupting protein translation in bacteria, thereby damaging the ability of microbes to grow and repair; however protein translation is also disrupted in eukaryotic mitochondria leading to effects that may confound experimental results.[62][63] It can be used as an artificial biomarker in wildlife to check if wild animals are consuming a bait that contains a vaccine or medication. Since it is fluorescent and binds to calcium, a UV lamp can be used to check if it is in a tooth pulled from an animal. For example, it was used to check uptake of oral rabies vaccine baits by raccoons in the USA. However, this is an invasive procedure for the animal and labour-intensive for the researcher. Therefore, other dyes such as rhodamine B that can be detected in hair and whiskers are preferred.[64]
See also
References
- "Tetracycline". Encyclopedia Britannica. Retrieved 1 October 2018.
- Chopra I, Roberts M (June 2001). "Tetracycline antibiotics: mode of action, applications, molecular biology, and epidemiology of bacterial resistance". Microbiology and Molecular Biology Reviews. 65 (2): 232–60, second page, table of contents. doi:10.1128/MMBR.65.2.232-260.2001. PMC 99026. PMID 11381101.
- "Tetracyclines". IUPAC Compendium of Chemical Terminology. 2009. doi:10.1351/goldbook.T06287. ISBN 978-0-9678550-9-7.
{{cite book}}:|website=ignored (help) - Blackwood RK, English AR (1970). "Structure–Activity Relationships in the Tetracycline Series". Advances in Applied Microbiology. 13: 237–266. doi:10.1016/S0065-2164(08)70405-2. ISBN 9780120026135.
- Markley JL, Wencewicz TA (30 May 2018). "Tetracycline-Inactivating Enzymes". Frontiers in Microbiology. 9: 1058. doi:10.3389/fmicb.2018.01058. PMC 5988894. PMID 29899733.
- Sloan B, Scheinfeld N (September 2008). "The use and safety of doxycycline hyclate and other second-generation tetracyclines". Expert Opinion on Drug Safety. 7 (5): 571–7. doi:10.1517/14740338.7.5.571. PMID 18759709. S2CID 73300549.
- WHO Advisory Group on Integrated Surveillance of Antimicrobial Resistance (2017). Critically important antimicrobials for human medicine : ranking of antimicrobial agents for risk management of antimicrobial resistance due to non-human use (5th revision 2016 ed.). [Geneva, Switzerland?]: World Health Organization. ISBN 9789241512220. OCLC 982301334.
- Simonart T, Dramaix M, De Maertelaer V (February 2008). "Efficacy of tetracyclines in the treatment of acne vulgaris: a review". The British Journal of Dermatology. 158 (2): 208–16. doi:10.1111/j.1365-2133.2007.08286.x. PMID 17986300. S2CID 8103852.
- Chow AW, Patten V, Guze LB (January 1975). "Comparative susceptibility of anaerobic bacteria to minocycline, doxycycline, and tetracycline". Antimicrobial Agents and Chemotherapy. 7 (1): 46–9. doi:10.1128/aac.7.1.46. PMC 429070. PMID 1137358.
- Taylor, MJ; Makunde, WH; McGarry, HF; Turner, JD; Mand, S; Hoerauf, A (June 2005). "Macrofilaricidal activity after doxycycline treatment of Wuchereria bancrofti: a double-blind, randomised placebo-controlled trial". Lancet. 365 (9477): 2116–21. doi:10.1016/S0140-6736(05)66591-9. PMID 15964448. S2CID 21382828.
- Bhattacharya SK (February 2003). "An evaluation of current cholera treatment". Expert Opinion on Pharmacotherapy. 4 (2): 141–6. doi:10.1517/14656566.4.2.141. PMID 12562304. S2CID 19819196.
- Parsi VK (May 2001). "Cholera". Primary Care Update for Ob/Gyns. 8 (3): 106–109. doi:10.1016/S1068-607X(00)00086-X. PMID 11378428.
- "Drugs and their categories in pregnancy and breastfeeding". www.tg.org.au. Archived from the original on 14 September 2009. Retrieved 3 February 2022.
- "Archived copy". Archived from the original on 2016-04-09. Retrieved 2019-04-16.
{{cite web}}: CS1 maint: archived copy as title (link) - Deboyser D, Goethals F, Krack G, Roberfroid M (March 1989). "Investigation into the mechanism of tetracycline-induced steatosis: study in isolated hepatocytes". Toxicology and Applied Pharmacology. 97 (3): 473–9. doi:10.1016/0041-008X(89)90252-4. PMID 2609344.
- Amacher DE, Martin BA (December 1997). "Tetracycline-induced steatosis in primary canine hepatocyte cultures". Fundamental and Applied Toxicology. 40 (2): 256–63. doi:10.1006/faat.1997.2389. PMID 9441722.
- Ekwall B, Acosta D (1982). "In vitro comparative toxicity of selected drugs and chemicals in HeLa cells, Chang liver cells, and rat hepatocytes". Drug and Chemical Toxicology. 5 (3): 219–31. doi:10.3109/01480548209041054. PMID 7151717.
- Archer JS, Archer DF (June 2002). "Oral contraceptive efficacy and antibiotic interaction: a myth debunked". Journal of the American Academy of Dermatology. 46 (6): 917–23. doi:10.1067/mjd.2002.120448. PMID 12063491.
- Dréno B, Bettoli V, Ochsendorf F, Layton A, Mobacken H, Degreef H (2004). "European recommendations on the use of oral antibiotics for acne". European Journal of Dermatology. 14 (6): 391–9. PMID 15564203.
- DeRossi SS, Hersh EV (October 2002). "Antibiotics and oral contraceptives". Dental Clinics of North America. 46 (4): 653–64. CiteSeerX 10.1.1.620.9933. doi:10.1016/S0011-8532(02)00017-4. PMID 12436822.
- "Tetracycline and Pregnancy" (PDF). Organization of Teratology Information Specialists. July 2010. Archived from the original (PDF) on 2011-08-27.
- "Mechanism of Action of Tetracyclines - Animations - PharmaXChange.info". 27 May 2011. Retrieved 13 March 2017.
- Chukwudi CU (August 2016). "rRNA Binding Sites and the Molecular Mechanism of Action of the Tetracyclines". Antimicrobial Agents and Chemotherapy. 60 (8): 4433–41. doi:10.1128/AAC.00594-16. PMC 4958212. PMID 27246781.
- Spreitzer H (July 2, 2007). "Neue Wirkstoffe – Incyclinid". Österreichische Apothekerzeitung (in German) (14/2007): 655.
- Viera MH, Perez OA, Berman B (2007). "Incyclinide". Drugs of the Future. 32 (3): 209–214. doi:10.1358/dof.2007.032.03.1083308.
- Ryan ME, Usman A, Ramamurthy NS, Golub LM, Greenwald RA (February 2001). "Excessive matrix metalloproteinase activity in diabetes: inhibition by tetracycline analogues with zinc reactivity". Current Medicinal Chemistry. 8 (3): 305–16. doi:10.2174/0929867013373598. PMID 11172685.
- "CollaGenex says incyclinide ineffective for rosacea". Reuters. 26 September 2016. Retrieved 13 March 2017.
- Richards C, Pantanowitz L, Dezube BJ (February 2011). "Antimicrobial and non-antimicrobial tetracyclines in human cancer trials". Pharmacological Research. 63 (2): 151–6. doi:10.1016/j.phrs.2010.10.008. PMID 20951804.
- Tariq S, Rizvi SF, Anwar U (25 July 2018). "Tetracycline: Classification, Structure Activity Relationship and Mechanism of Action as a Theranostic Agent for Infectious Lesions-A Mini Review" (PDF). Biomedical Journal of Scientific & Technical Research. 7 (2). doi:10.26717/BJSTR.2018.07.001475.
- Fuoco D (June 2012). "Classification Framework and Chemical Biology of Tetracycline-Structure-Based Drugs". Antibiotics. 1 (1): 1–13. doi:10.3390/antibiotics1010001. PMC 4790241. PMID 27029415.
- "Tetracycline – Structure-activity relationships". University of Bristol. Retrieved 2 October 2018.
- Forsberg KJ, Patel S, Wencewicz TA, Dantas G (July 2015). "The Tetracycline Destructases: A Novel Family of Tetracycline-Inactivating Enzymes". Chemistry & Biology. 22 (7): 888–97. doi:10.1016/j.chembiol.2015.05.017. PMC 4515146. PMID 26097034.
- Roberts MC (October 1996). "Tetracycline resistance determinants: mechanisms of action, regulation of expression, genetic mobility, and distribution". FEMS Microbiology Reviews. 19 (1): 1–24. doi:10.1111/j.1574-6976.1996.tb00251.x. PMID 8916553.
- Grossman TH (April 2016). "Tetracycline Antibiotics and Resistance". Cold Spring Harbor Perspectives in Medicine. 6 (4): a025387. doi:10.1101/cshperspect.a025387. PMC 4817740. PMID 26989065.
- Warburton PJ, Amodeo N, Roberts AP (December 2016). "Mosaic tetracycline resistance genes encoding ribosomal protection proteins". The Journal of Antimicrobial Chemotherapy. 71 (12): 3333–3339. doi:10.1093/jac/dkw304. PMC 5181394. PMID 27494928.
- Li W, Atkinson GC, Thakor NS, Allas U, Lu CC, Chan KY, et al. (12 February 2013). "Mechanism of tetracycline resistance by ribosomal protection protein Tet(O)". Nature Communications. 4 (1): 1477. Bibcode:2013NatCo...4.1477L. doi:10.1038/ncomms2470. PMC 3576927. PMID 23403578.
- Dönhöfer A, Franckenberg S, Wickles S, Berninghausen O, Beckmann R, Wilson DN (October 2012). "Structural basis for TetM-mediated tetracycline resistance". Proceedings of the National Academy of Sciences of the United States of America. 109 (42): 16900–5. Bibcode:2012PNAS..10916900D. doi:10.1073/pnas.1208037109. PMC 3479509. PMID 23027944.
- Connell SR, Tracz DM, Nierhaus KH, Taylor DE (December 2003). "Ribosomal protection proteins and their mechanism of tetracycline resistance". Antimicrobial Agents and Chemotherapy. 47 (12): 3675–81. doi:10.1128/AAC.47.12.3675-3681.2003. PMC 296194. PMID 14638464.
- Piscitelli SC, Rodvold K (2005). Drug Interactions in Infectious Diseases. Humana Press. ISBN 978-1-58829-455-5.
- Nelson ML, Levy SB (December 2011). "The history of the tetracyclines". Annals of the New York Academy of Sciences. 1241 (1): 17–32. Bibcode:2011NYASA1241...17N. doi:10.1111/j.1749-6632.2011.06354.x. PMID 22191524. S2CID 34647314.
- Essays, UK (November 2013). "Tetracycline: History, Properties and Uses". Nottingham, UK: UKEssays.com. Retrieved 2 October 2018.
- "The Pharmaceutical Century".
- Lin DW. "The teteracyclines" (PDF). Baran Lab. Baran labs. Retrieved 3 October 2018.
- Finlay AC, Hobby GL (January 1950). "Terramycin, a new antibiotic". Science. 111 (2874): 85. Bibcode:1950Sci...111...85F. doi:10.1126/science.111.2874.85. PMID 15400447.
- "Lemelson-MIT Program". Archived from the original on 18 March 2003. Retrieved 13 March 2017.
- Samuel D (1996). "Archaeology of ancient Egypt beer" (PDF). Journal of the American Society of Brewing Chemists. 54 (1): 3–12. doi:10.1094/ASBCJ-54-0003.
- Bassett EJ, Keith MS, Armelagos GJ, Martin DL, Villanueva AR (September 1980). "Tetracycline-labeled human bone from ancient Sudanese Nubia (A.D. 350)" (PDF). Science. 209 (4464): 1532–4. Bibcode:1980Sci...209.1532B. doi:10.1126/science.7001623. PMID 7001623. Archived from the original (PDF) on 2016-03-04. Retrieved 2014-06-19.
- Roberts MC (February 2003). "Tetracycline therapy: update". Clinical Infectious Diseases. 36 (4): 462–7. doi:10.1086/367622. PMID 12567304.
- Zhanel GG, Cheung D, Adam H, Zelenitsky S, Golden A, Schweizer F, et al. (April 2016). "Review of Eravacycline, a Novel Fluorocycline Antibacterial Agent". Drugs. 76 (5): 567–88. doi:10.1007/s40265-016-0545-8. PMID 26863149. S2CID 36285428.
- Solomkin J, Evans D, Slepavicius A, Lee P, Marsh A, Tsai L, et al. (March 2017). "Assessing the Efficacy and Safety of Eravacycline vs Ertapenem in Complicated Intra-abdominal Infections in the Investigating Gram-Negative Infections Treated With Eravacycline (IGNITE 1) Trial: A Randomized Clinical Trial". JAMA Surgery. 152 (3): 224–232. doi:10.1001/jamasurg.2016.4237. PMID 27851857. S2CID 42977246.
- Olson MW, Ruzin A, Feyfant E, Rush TS, O'Connell J, Bradford PA (June 2006). "Functional, biophysical, and structural bases for antibacterial activity of tigecycline". Antimicrobial Agents and Chemotherapy. 50 (6): 2156–66. doi:10.1128/AAC.01499-05. PMC 1479133. PMID 16723578.
- "How Paratek hopes to succeed in antibiotics despite Tetraphase's fail". Bizjournals.com. Retrieved 2017-03-13.
- Agwuh KN, MacGowan A (August 2006). "Pharmacokinetics and pharmacodynamics of the tetracyclines including glycylcyclines". The Journal of Antimicrobial Chemotherapy. 58 (2): 256–65. doi:10.1093/jac/dkl224. PMID 16816396.
- "Drug Trial Snapshot: Xerava". FDA. Retrieved 2 October 2018.
- "Drug Trial Snapshot: Seysara". FDA. Retrieved 8 February 2019.
- "Sarecycline". PubChem. U.S. National Library of Medicine. Retrieved 2020-06-07.
- Zhanel G, Critchley I, Lin LY, Alvandi N (January 2019). "Microbiological Profile of Sarecycline, a Novel Targeted Spectrum Tetracycline for the Treatment of Acne Vulgaris". Antimicrobial Agents and Chemotherapy. 63 (1). doi:10.1128/AAC.01297-18. PMC 6325184. PMID 30397052.
- "Antibiotic Firm Paratek Joins IPO Queue; Aiming for $92M". Archived from the original on 18 October 2017. Retrieved 13 March 2017.
- "Drug Trial Snapshot: Nuzyra". FDA. Retrieved 8 February 2019.
- "Drug Trial Snapshot: Nuzyra". FDA. Retrieved 8 February 2019.
- Zhu, Z., Zheng, T., Lee, C. G., Homer, R. J., & Elias, J. A. (2002). Tetracycline-controlled transcriptional regulation systems: advances and application in transgenic animal modeling. Seminars in Cell & Developmental Biology, 13(2), 121–128. doi:10.1016/s1084-9521(02)00018-6
- Moullan N, Mouchiroud L, Wang X, Ryu D, Williams EG, Mottis A, et al. (March 2015). "Tetracyclines Disturb Mitochondrial Function across Eukaryotic Models: A Call for Caution in Biomedical Research". Cell Reports. 10 (10): 1681–1691. doi:10.1016/j.celrep.2015.02.034. PMC 4565776. PMID 25772356.
- Chatzispyrou IA, Held NM, Mouchiroud L, Auwerx J, Houtkooper RH (November 2015). "Tetracycline antibiotics impair mitochondrial function and its experimental use confounds research". Cancer Research. 75 (21): 4446–9. doi:10.1158/0008-5472.CAN-15-1626. PMC 4631686. PMID 26475870.
- Fry TL, Dunbar MR (2007). "A Review of Biomarkers Used For Wildlife Damage and Disease Management" (PDF). Proceedings of the 12th Wildlife Damage Management Conference: 217–222. Retrieved 2017-05-03.
External links
 Media related to Tetracycline antibiotics at Wikimedia Commons
Media related to Tetracycline antibiotics at Wikimedia Commons