Hoarse voice
A hoarse voice, also known as dysphonia or hoarseness,[1] is when the voice involuntarily sounds breathy, raspy, or strained, or is softer in volume or lower in pitch.[2][3] A hoarse voice, can be associated with a feeling of unease or scratchiness in the throat.[2] Hoarseness is often a symptom of problems in the vocal folds of the larynx.[2] It may be caused by laryngitis, which in turn may be caused by an upper respiratory infection, a cold, or allergies.[2] Cheering at sporting events, speaking loudly in noisy situations, talking for too long without resting one's voice, singing loudly, or speaking with a voice that's too high or too low can also cause temporary hoarseness.[2] A number of other causes for losing one's voice exist, and treatment is generally by resting the voice and treating the underlying cause.[2] If the cause is misuse or overuse of the voice, drinking plenty of water may alleviate the problems.[2]
| Hoarse voice | |
|---|---|
| Other names | Hoarseness, dysphonia |
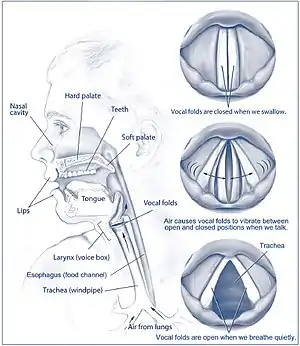 | |
| The vocal folds (or vocal cords) in the larynx vibrate to produce sound. When this process is disturbed hoarseness may ensue. | |
| Specialty | Otolaryngology |
It appears to occur more commonly in females and the elderly.[4] Furthermore, certain occupational groups, such as teachers and singers, are at an increased risk.[5][6]
Long-term hoarseness, or hoarseness that persists over three weeks, especially when not associated with a cold or flu should be assessed by a medical doctor.[2] It is also recommended to see a doctor if hoarseness is associated with coughing up blood, difficulties swallowing, a lump in the neck, pain when speaking or swallowing, difficulty breathing, or complete loss of voice for more than a few days.[2] For voice to be classified as "dysphonic", abnormalities must be present in one or more vocal parameters: pitch, loudness, quality, or variability.[7] Perceptually, dysphonia can be characterised by hoarse, breathy, harsh, or rough vocal qualities, but some kind of phonation remains.[7]
Dysphonia can be categorized into two broad main types: organic and functional, and classification is based on the underlying pathology. While the causes of dysphonia can be divided into five basic categories, all of them result in an interruption of the ability of the vocal folds to vibrate normally during exhalation, which affects the voice. The assessment and diagnosis of dysphonia is done by a multidisciplinary team, and involves the use of a variety of subjective and objective measures, which look at both the quality of the voice as well as the physical state of the larynx. Multiple treatments have been developed to address organic and functional causes of dysphonia. Dysphonia can be targeted through direct therapy, indirect therapy, medical treatments, and surgery. Functional dysphonias may be treated through direct and indirect voice therapies, whereas surgeries are recommended for chronic, organic dysphonias.[8]
Types
Voice disorders can be divided into 2 broad categories: organic and functional.[9] The distinction between these broad classes stems from their cause, whereby organic dysphonia results from some sort of physiological change in one of the subsystems of speech (for voice, usually respiration, laryngeal anatomy, and/or other parts of the vocal tract are affected). Conversely, functional dysphonia refers to hoarseness resulting from vocal use (i.e. overuse/abuse).[10] Furthermore, according to ASHA, organic dysphonia can be subdivided into structural and neurogenic; neurogenic dysphonia is defined as impaired functioning of the vocal structure due to a neurological problem (in the central nervous system or peripheral nervous system); in contrast, structural dysphonia is defined as impaired functioning of the vocal mechanism that is caused by some sort of physical change (e.g. a lesion on the vocal folds).[10] Notably, an additional subcategory of functional dysphonia recognized by professionals is psychogenic dysphonia, which can be defined as a type of voice disorder that has no known cause and can be presumed to be a product of some sort of psychological stressors in one's environment.[10][11] It is important to note that these types are not mutually exclusive and much overlap occurs. For example, Muscle Tension Dysphonia (MTD) has been found to be a result of many different causes including the following: MTD in the presence of an organic pathology (i.e. organic type), MTD stemming from vocal use (i.e. functional type), and MTD as a result of personality and/or psychological factors (i.e. psychogenic type).[10][12]
- Organic dysphonia
- Laryngitis (Acute: viral, bacterial) - (Chronic: smoking, GERD, LPR)
- Neoplasm (Premalignant: dysplasia) - (Malignant: Squamous cell carcinoma)
- Trauma (Iatrogenic: surgery, intubation) - (Accidental: blunt, penetrating, thermal)
- Endocrine (Hypothyroidism, hypogonadism)
- Haematological (Amyloidosis)
- Iatrogenic (inhaled corticosteroids)
- Functional dysphonia
- Psychogenic
- Vocal misuse
- Idiopathic
Causes
The most common causes of hoarseness is laryngitis (acute 42.1%; chronic 9.7%) and functional dysphonia (30%).[13] Hoarseness can also be caused by laryngeal tumours (benign 10.7 - 31%; malignant 2.2 - 3.0%).[13] Causes that are overall less common include neurogenic conditions (2.8 - 8.0%), psychogenic conditions (2.0 - 2.2%), and aging (2%).[13]
A variety of different causes, which result in abnormal vibrations of the vocal folds, can cause dysphonia. These causes can range from vocal abuse and misuse to systemic diseases. Causes of dysphonia can be divided into five basic categories, although overlap may occur between categories.[14][15][16][17] (Note that this list is not exhaustive):
- Neoplastic/structural: Abnormal growths of the vocal fold tissue.
- Inflammatory: Changes in the vocal fold tissue as a result of inflammation.
- Allergy
- Infections
- Reflux
- Smoking
- Trauma
- Voice abuse
- Neuromuscular: Disturbances in any of the components of the nervous system that control laryngeal function.
- Associated Systemic Diseases: Systemic diseases which have manifestations that affect the voice.
- Technical: Associated with poor muscle functioning or psychological stresses, with no corresponding physiological abnormalities of the larynx.
- Psychogenic such as dissociation disorder[18]
- Excess demands
- Stress
- Vocal strain
Employment
It has been suggested that certain occupational groups may be at increased risk of developing dysphonia[5][6] due to the excessive or intense vocal demands of their work.[19] Research on this topic has primarily focused on teachers and singers, although some studies have examined other groups of heavy voice users (e.g. actors, cheerleaders, aerobic instructors, etc.).[5][20] At present, it is known that teachers and singers are likely to report dysphonia.[19][21] Moreover, physical education teachers, teachers in noisy environments, and those who habitually use a loud speaking voice are at increased risk.[19] The term clergyman's throat or dysphonia clericorum was previously used for painful dysphonia associated with public speaking, particularly among preachers.[22] However, the exact prevalence rates for occupational voice users are unclear, as individual studies have varied widely in the methodologies used to obtain data (e.g. employing different operational definitions for "singer").[19][21]
Mechanism
Located in the anterior portion of the neck is the larynx (also known as the voice box), a structure made up of several supporting cartilages and ligaments, which houses the vocal folds.[23] In normal voice production, exhaled air moves out of the lungs and passes upward through the vocal tract.[23] At the level of the larynx, the exhaled air causes the vocal folds to move toward the midline of the tract (a process called adduction). The adducted vocal folds do not close completely but instead remain partially open. The narrow opening between the folds is referred to as the glottis.[23][7] As air moves through the glottis, it causes a distortion of the air particles which sets the vocal folds into vibratory motion. It is this vibratory motion that produces phonation or voice.[7] In dysphonia, there is an impairment in the ability to produce an appropriate level of phonation. More specifically, it results from an impairment in vocal fold vibration or the nerve supply of the larynx.[7]
Diagnosis
The assessment and diagnosis of a dysphonic voice is completed by a multidisciplinary team, such as an otolaryngologist (ear, nose and throat doctor) and Speech-Language Pathologist, involving the use of both objective and subjective measures to evaluate the quality of the voice as well as the condition of the vocal fold tissue and vibration patterns.[24]
Definition
Dysphonia is a broad clinical term which refers to abnormal functioning of the voice.[23][7] More specifically, a voice can be classified as "dysphonic" when there are abnormalities or impairments in one or more of the following parameters of voice: pitch, loudness, quality, and variability.[7] For example, abnormal pitch can be characterized by a voice that is too high or low whereas abnormal loudness can be characterized by a voice that is too quiet or loud.[7] Similarly, a voice that has frequent, inappropriate breaks characterizes abnormal quality while a voice that is monotone (i.e., very flat) or inappropriately fluctuates characterizes abnormal variability.[7] While hoarseness is used interchangeably with the term dysphonia, it is important to note that the two are not synonymous. Hoarseness is merely a subjective term to explain the perceptual quality (or sound) of a dysphonic voice.[25] While hoarseness is a common symptom (or complaint) of dysphonia,[23] there are several other signs and symptoms that can be present such as: breathiness, roughness, and dryness. Furthermore, a voice can be classified as dysphonic when it poses problems in the functional or occupational needs of the individual or is inappropriate for their age or sex.[7]
Auditory-perceptual measures
Auditory-perceptual measures are the most commonly used tool by clinicians to evaluate the voice quality due to its quick and non-invasive nature.[26] Additionally, these measures have been proven to be reliable in a clinical setting.[27] Ratings are used to evaluate the quality of a patient's voice for a variety of voice features, including overall severity, roughness, breathiness, strain, loudness and pitch. These evaluations are done during spontaneous speech, sentence or passage reading or sustained vowel productions.[17] The GRBAS (Grade, Roughness, Breathiness, Asthenia, Strain) and the CAPE-V (Consensus Auditory Perceptual Evaluation—Voice) are two formal voice rating scales commonly used for this purpose.[26]
Vocal fold imaging
Vocal fold imaging techniques are used by clinicians to examine the vocal folds and allows them to detect vocal pathology and assess the quality of the vocal fold vibrations. Laryngeal stroboscopy is the primary clinical tool used for this purpose. Laryngeal stroboscopy uses a synchronized flashing light passed through either a rigid or flexible laryngoscope to provide an image of the vocal fold motion; the image is created by averaging over several vibratory cycles and is thus not provided in real-time.[28] As this technique relies on periodic vocal fold vibration, it cannot be used in patients with moderate to severe dysphonia.[17] High speed digital imaging of the vocal folds (videokymography), another imaging technique, is not subject to the same limitations as laryngeal stroboscopy. A rigid endoscope is used to take images at a rate of 8000 frames per second, and the image is displayed in real time. As well, this technique allows imaging of aperiodic vibrations[17] and can thus be used with patients presenting with all severities of dysphonia.
Acoustic measures
Acoustic measures can be used to provide objective measures of vocal function. Signal processing algorithms are applied to voice recordings made during sustained phonation or during spontaneous speech.[29] The acoustic parameters which can then be examined include fundamental frequency, signal amplitude, jitter, shimmer, and noise-to-harmonic ratios.[17] However, due to limitations imposed by the algorithms employed, these measures cannot be used with patients who exhibit severe dysphonia.[29]
Aerodynamic measures
Aerodynamic measures of voice include measures of air volume, air flow and sub glottal air pressure. The normal aerodynamic parameters of voice vary considerably among individuals, which leads to a large overlapping range of values between dysphonic and non-dysphonic patients. This limits the use of these measures as a diagnostic tool.[17] Nonetheless, they are useful when used in adjunct with other voice assessment measures, or as a tool for monitoring therapeutic effects over time.[27]
Prevention
Given that certain occupations are more at risk for developing dysphonia (e.g. teachers) research into prevention studies have been conducted.[30] Research into the effectiveness of prevention strategies for dysphonia have yet to produce definitive results, however, research is still ongoing.[9][30] Primarily, there are two types of vocal training recognized by professionals to help with prevention: direct and indirect. Direct prevention describes efforts to reduce conditions that may serve to increase vocal strain (such as patient education, relaxation strategies, etc.), while indirect prevention strategies refer to changes in the underlying physiological mechanism for voice production (e.g., adjustments to the manner in which vocal fold adduction occurs, respiratory training, shifting postural habits, etc.).[9][30]
Treatment
Although there is no universal classification of voice problems, voice disorders can be separated into certain categories: organic (structural or neurogenic), functional, neurological (psychogenic) or iatrogenic, for example.[31] Depending on the diagnosis and severity of the voice problem, and depending on the category that the voice disorder falls into, there are various treatment methods that can be suggested to the patient. The professional has to keep in mind there is not one universal treatment, but rather the clinical approach must find what the optimal effective course of action for that particular patient is.
There are three main type of treatments: medical treatments, voice therapy and surgical treatments.[32] When necessary, certain voice disorders use a combination of treatment approaches.[9] A medical treatment involves the use of botulinum toxin (botox) or anti-reflux medicines, for example. Botox is a key treatment for voice disorders such as Spasmodic Dysphonia.[33] Voice therapy is mainly used with patients who have an underlying cause of voice misuse or abuse.[34] Laryngologists also recommend this type of treatment to patients who have an organic voice disorder - such as vocal fold nodules, cysts or polyps as well as to treat functional dysphonia.[9] Certain surgical treatments can be implemented as well - phono microsurgery (removal of vocal fold lesions performed with a microscope), laryngeal framework surgery (the manipulation of the voice box), as well as injection augmentation (injection of substance to vocal folds to improve closure). Surgical treatments may be recommended for patients having an organic dysphonia.[35][36]
A combination of both an indirect treatment method (an approach used to change external factors affecting the vocal folds)[37] and a direct treatment method (an approach used where the mechanisms functioning during the use of the vocal folds, such as phonation or respiration, are the main focus)[37] may be used to treat dysphonia.[9][12][38][39]
Direct therapies
Direct therapies address the physical aspects of vocal production.[9] Techniques work to either modify vocal fold contact, manage breathing patterns, and/or change the tension at level of the larynx.[9] Notable techniques include, but are not limited to, the yawn-sigh method, optimal pitch, laryngeal manipulation, humming, the accent method, and the Lee Silverman Voice Treatment.[9][38] An example of a direct therapy is circumlaryngeal manual therapy, which has been used to reduce tension and massage hyoid-laryngeal muscles.[12] This area is often tense from chronic elevation of the larynx.[12] Pressure is applied to these areas as the patient hums or sustains a vowel.[12] Traditional voice therapy is often used to treat muscular tension dysphonia.[12]
Indirect therapies
Indirect therapies take into account external factors that may influence vocal production.[9] This incorporates maintenance of vocal hygiene practices, as well as the prevention of harmful vocal behaviours.[40] Vocal hygiene includes adequate hydration of the vocal folds, monitoring the amount of voice use and rest, avoidance of vocal abuse (e.g., shouting, clearing of the throat), and taking into consideration lifestyle choices that may affect vocal health (e.g., smoking, sleeping habits).[40] Vocal warm-ups and cool-downs may be employed to improve muscle tension and decrease risk of injury before strenuous vocal activities.[40] It should be taken into account that vocal hygiene practices alone are minimally effective in treating dysphonia, and thus should be paired with other therapies.[40]
Medication and surgery
Medical and surgical treatments have been recommended to treat organic dysphonias. An effective treatment for spasmodic dysphonia (hoarseness resulting from periodic breaks in phonation due to hyperadduction of the vocal folds) is botulinum toxin injection.[8][41] The toxin acts by blocking acetylcholine release at the thyro-arytenoid muscle. Although the use of botulinum toxin injections is considered relatively safe, patients' responses to treatment differ in the initial stages; some have reported experiencing swallowing problems and breathy voice quality as a side-effect to the injections.[8][41] Breathiness may last for a longer period of time for males than females.[41]
Surgeries involve myoectomies of the laryngeal muscles to reduce voice breaks, and laryngoplasties, in which laryngeal cartilage is altered to reduce tension.[8]
Epidemiology
Dysphonia is a general term for voice impairment that is sometimes used synonymously with the perceptual voice quality of hoarseness.[13] It is the reason for 1% of all visits to primary care providers.[13] The lifetime risk of hoarse voice complaints among primary care patients is 30%.[13] Since hoarseness is a general symptom, it is associated with a number of laryngeal diagnoses.[13]
There is an interplay of sex and age differences associated with dysphonia. The point prevalence of dysphonia in adults under the age of 65 is 6.6%.[20] Dysphonia is more common in adult females than males,[20][42] possibly due to sex-related anatomical differences of the vocal mechanism.[4] In childhood, however, dysphonia is more often found in boys than girls.[43] As there are no anatomical differences in larynges of boys and girls prior to puberty, it has been proposed that the higher rate of voice impairment found in boys arises from louder social activities, personality factors, or more frequent inappropriate vocal use.[43] The most common laryngeal diagnosis among children is vocal fold nodules,[20] a condition known to be associated with vocally damaging behaviours.[44] However, a causal relationship has not yet been definitively proven.[43] The overall prevalence of dysphonia in children ranges from 3.9% - 23.4%, most commonly affecting children between the ages of 8 - 14.[20] Among the elderly, dysphonia is associated with both naturally occurring anatomical and physiological changes as well as higher rates of pathological conditions.[42] The point prevalence of dysphonia among the elderly is 29%.[20] Findings regarding the prevalence of geriatric dysphonia in the general population are very variable, ranging from 4 - 29.1%.[42] This variability is likely due to different methodology used in obtaining information from participants.[20] The most common laryngeal diagnoses among the elderly are polyps, laryngopharyngeal reflux, muscle tension dysphonia, vocal fold paresis or paralysis, vocal fold mass, glottic insufficiency, malignant lesions, and neurologic conditions affecting the larynx.[42]
References
- "Hoarseness".
- "Hoarseness". NIDCD. 2015-08-18. Retrieved 2017-07-24.
- Johns MM, Sataloff RT, Merati AL, Rosen CA (August 2010). "Shortfalls of the American Academy of Otolaryngology-Head and Neck Surgery's Clinical practice guideline: Hoarseness (Dysphonia)". Otolaryngology–Head and Neck Surgery. 143 (2): 175–7, discussion 175–80. doi:10.1016/j.otohns.2010.05.026. PMID 20647114. S2CID 22553812.
- Cohen SM, Kim J, Roy N, Asche C, Courey M (February 2012). "Prevalence and causes of dysphonia in a large treatment-seeking population". The Laryngoscope. 122 (2): 343–8. doi:10.1002/lary.22426. PMID 22271658. S2CID 31457683.
- Williams, N. R. (2003). "Occupational groups at risk for voice disorders: A review of the literature". Occupational Medicine. 53 (7): 456–460. doi:10.1093/occmed/kqg113. PMID 14581643.
- Verdolini K, Ramig LO (2001). "Review: occupational risks for voice problems". Logopedics, Phoniatrics, Vocology. 26 (1): 37–46. doi:10.1080/14015430119969. PMID 11432413. S2CID 7436065.
- Aronson AE, Bless DM (2009). Clinical voice disorders. New York: Thieme. pp. 1–5.
- Ludlow CL (June 2009). "Treatment for spasmodic dysphonia: limitations of current approaches". Current Opinion in Otolaryngology & Head and Neck Surgery. 17 (3): 160–5. doi:10.1097/moo.0b013e32832aef6f. PMC 2763389. PMID 19337127.
- Ruotsalainen J, Sellman J, Lehto L, Verbeek J (May 2008). "Systematic review of the treatment of functional dysphonia and prevention of voice disorders". Otolaryngology–Head and Neck Surgery. 138 (5): 557–65. doi:10.1016/j.otohns.2008.01.014. PMID 18439458.
- "Voice Disorders Overview". American Speech-Language Hearing Association. Retrieved October 2, 2016.
- Duffy JR, Yorkston KM (2003). "Medical interventions for Spasmodic Dysphonia and some related conditions: A systematic review". Journal of Medical Speech-Language Pathology. 11.
- Van Houtte E, Van Lierde K, Claeys S (March 2011). "Pathophysiology and treatment of muscle tension dysphonia: a review of the current knowledge". Journal of Voice. 25 (2): 202–7. doi:10.1016/j.jvoice.2009.10.009. PMID 20400263.
- Reiter R, Hoffmann TK, Pickhard A, Brosch S (May 2015). "Hoarseness-causes and treatments". Deutsches Ärzteblatt International. 112 (19): 329–37. doi:10.3238/arztebl.2015.0329. PMC 4458789. PMID 26043420.
- Feierabend RH, Shahram MN (August 2009). "Hoarseness in adults". American Family Physician. 80 (4): 363–70. PMID 19678604.
- Pylypowich A, Duff E (2016). "Differentiating the Symptom of Dysphonia". The Journal for Nurse Practitioners. 12 (7): 459–466. doi:10.1016/j.nurpra.2016.04.025.
- Harries M (2013). "Hoarseness and Voice Disorders". In Ludman HS, Bradley PJ (eds.). ABC of ear, nose, and throat. West Sussex, UK: Wiley-Blackwell. p. 95.
- Morris R, Bernard Harmon A (2010). "Describing Voice Disorders". In Damico J, Muller N, Ball MJ (eds.). Handbook of language and speech disorders. Chichester, U.K.: Wiley-Blackwell. pp. 455–473. ISBN 9781405158626.
- Dr Pragya Semwal, Dr Shobit Garg Chronic Dissociation Presenting as Dysphonia Plica Ventricularis: An Atypical Presentation. Int. j. med. case reports Vol 6 Issue 3 Jul-Sep 2020 1-3. http://www.ijomcr.net
- Cantor Cutiva LC, Vogel I, Burdorf A (March 2013). "Voice disorders in teachers and their associations with work-related factors: a systematic review". Journal of Communication Disorders. 46 (2): 143–55. doi:10.1016/j.jcomdis.2013.01.001. PMID 23415241.
- Stachler RJ, Francis DO, Schwartz SR, Damask CC, Digoy GP, Krouse HJ, McCoy SJ, Ouellette DR, Patel RR, Reavis CC, Smith LJ, Smith M, Strode SW, Woo P, Nnacheta LC (March 2018). "Clinical Practice Guideline: Hoarseness (Dysphonia) (Update)". Otolaryngology–Head and Neck Surgery. 158 (1_suppl): S1–S42. doi:10.1177/0194599817751030. PMID 29494321.
- Pestana PM, Vaz-Freitas S, Manso MC (November 2017). "Prevalence of Voice Disorders in Singers: Systematic Review and Meta-Analysis". Journal of Voice. 31 (6): 722–727. doi:10.1016/j.jvoice.2017.02.010. PMID 28342677.
- Broadwater, Kimberly (2021). "Clergyman's Sore Throat". Journal of Singing. 78 (1): 113–117. doi:10.53830/CNLB1302. ISSN 2769-4046. S2CID 239663449.
- Colton, R. H., Casper, J. K., Leonard, R. (2011). Understanding voice problems: A physiological perspective for diagnosis and treatment. Baltimore, MB: Lippincott Williams & Wilkins. pp. 372–385.
- Mehta DD, Hillman RE (June 2008). "Voice assessment: updates on perceptual, acoustic, aerodynamic, and endoscopic imaging methods". Current Opinion in Otolaryngology & Head and Neck Surgery. 16 (3): 211–5. doi:10.1097/moo.0b013e3282fe96ce. PMC 3775647. PMID 18475073.
- Schwartz SR, Cohen SM, Dailey SH, Rosenfeld RM, Deutsch ES, Gillespie MB, Granieri E, Hapner ER, Kimball CE, Krouse HJ, McMurray JS, Medina S, O'Brien K, Ouellette DR, Messinger-Rapport BJ, Stachler RJ, Strode S, Thompson DM, Stemple JC, Willging JP, Cowley T, McCoy S, Bernad PG, Patel MM (September 2009). "Clinical practice guideline: hoarseness (dysphonia)". Otolaryngology–Head and Neck Surgery. 141 (3 Suppl 2): S1–S31. doi:10.1016/j.otohns.2009.06.744. PMID 19729111. S2CID 14655786.
- Oates J (2009). "Auditory-perceptual evaluation of disordered voice quality: pros, cons and future directions". Folia Phoniatrica et Logopaedica. 61 (1): 49–56. doi:10.1159/000200768. PMID 19204393.
- Dejonckere PH, Bradley P, Clemente P, Cornut G, Crevier-Buchman L, Friedrich G, Van De Heyning P, Remacle M, Woisard V (February 2001). "A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Guideline elaborated by the Committee on Phoniatrics of the European Laryngological Society (ELS)". European Archives of Oto-Rhino-Laryngology. 258 (2): 77–82. doi:10.1007/s004050000299. PMID 11307610. S2CID 3795132.
- Kendall KA (March 2009). "High-speed laryngeal imaging compared with videostroboscopy in healthy subjects". Archives of Otolaryngology–Head & Neck Surgery. 135 (3): 274–81. doi:10.1001/archoto.2008.557. PMID 19289706.
- Little MA, McSharry PE, Roberts SJ, Costello DA, Moroz IM (June 2007). "Exploiting nonlinear recurrence and fractal scaling properties for voice disorder detection". BioMedical Engineering OnLine. 6: 23. arXiv:0707.0086. doi:10.1186/1475-925X-6-23. PMC 1913514. PMID 17594480.
- Ruotsalainen JH, Sellman J, Lehto L, Jauhiainen M, Verbeek JH (October 2007). "Interventions for preventing voice disorders in adults". The Cochrane Database of Systematic Reviews. 4 (4): CD006372. doi:10.1002/14651858.cd006372.pub2. PMC 8923518. PMID 17943906.
- Morrison MD, Rammage LA (May 1993). "Muscle misuse voice disorders: description and classification". Acta Oto-Laryngologica. 113 (3): 428–34. doi:10.3109/00016489309135839. PMID 8517149.
- Maryn Y, De Bodt M, Roy N (May 2010). "The Acoustic Voice Quality Index: toward improved treatment outcomes assessment in voice disorders". Journal of Communication Disorders. 43 (3): 161–74. doi:10.1016/j.jcomdis.2009.12.004. PMID 20080243.
- Kim JW, Park JH, Park KN, Lee SW (2014). "Treatment efficacy of electromyography versus fiberscopy-guided botulinum toxin injection in adductor spasmodic dysphonia patients: a prospective comparative study". TheScientificWorldJournal. 2014: 327928. doi:10.1155/2014/327928. PMC 4213399. PMID 25383369.
- Chow YW, Pietranico R, Mukerji A (October 1975). "Studies of oxygen binding energy to hemoglobin molecule". Biochemical and Biophysical Research Communications. 66 (4): 1424–31. doi:10.1016/0006-291x(75)90518-5. PMID 6.
- Nacci A, Romeo SO, Berrettini S, Matteucci J, Cavaliere MD, Mancini V, Panicucci E, Ursino F, Fattori B (August 2017). "Stabilometric findings in patients affected by organic dysphonia before and after phonomicrosurgery". Acta Otorhinolaryngologica Italica. 37 (4): 286–294. doi:10.14639/0392-100x-1035. PMC 5584100. PMID 28872158.
- Encyclopedia of otolaryngology, head and neck surgery. Kountakis, Stilianos E. Berlin: Springer. 2013. ISBN 9783642234996. OCLC 837855971.
{{cite book}}: CS1 maint: others (link) - "Voice Disorders: Treatment". American Speech-Language-Hearing Association. Retrieved 2018-10-03.
- Hicks DM (June 1999). "The efficacy of voice treatment". Current Opinion in Otolaryngology & Head and Neck Surgery. 7 (3): 125. doi:10.1097/00020840-199906000-00005.
- Ulis JM, Yanagisawa E (June 2009). "What's new in differential diagnosis and treatment of hoarseness?". Current Opinion in Otolaryngology & Head and Neck Surgery. 17 (3): 209–15. doi:10.1097/moo.0b013e32832a2230. PMID 19469052. S2CID 26072006.
- Behlau M, Oliveira G (June 2009). "Vocal hygiene for the voice professional". Current Opinion in Otolaryngology & Head and Neck Surgery. 17 (3): 149–54. doi:10.1097/moo.0b013e32832af105. PMID 19342952. S2CID 38511217.
- Boutsen F, Cannito MP, Taylor M, Bender B (June 2002). "Botox treatment in adductor spasmodic dysphonia: a meta-analysis". Journal of Speech, Language, and Hearing Research. 45 (3): 469–81. doi:10.1044/1092-4388(2002/037). PMID 12069000.
- de Araújo Pernambuco L, Espelt A, Balata PM, de Lima KC (October 2015). "Prevalence of voice disorders in the elderly: a systematic review of population-based studies". European Archives of Oto-Rhino-Laryngology. 272 (10): 2601–9. doi:10.1007/s00405-014-3252-7. PMID 25149291. S2CID 24668793.
- Maia AA, Gama AC, Kümmer AM (April 2014). "Behavioral characteristics of dysphonic children: integrative literature review". CoDAS. 26 (2): 159–63. doi:10.1590/2317-1782/2014408IN. PMID 24918510.
- Mansuri B, Tohidast SA, Soltaninejad N, Kamali M, Ghelichi L, Azimi H (September 2018). "Nonmedical Treatments of Vocal Fold Nodules: A Systematic Review". Journal of Voice. 32 (5): 609–620. doi:10.1016/j.jvoice.2017.08.023. PMID 29032130. S2CID 37755681.