Atrioventricular septal defect
Atrioventricular septal defect (AVSD) or atrioventricular canal defect (AVCD), also known as "common atrioventricular canal" (CAVC) or "endocardial cushion defect" (ECD), is characterized by a deficiency of the atrioventricular septum of the heart. It is caused by an abnormal or inadequate fusion of the superior and inferior endocardial cushions with the mid portion of the atrial septum and the muscular portion of the ventricular septum.
| Atrioventricular septal defect | |
|---|---|
| Other names | Atrioventricular canal defect |
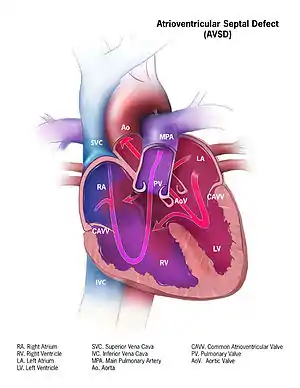 | |
| Illustration of a atrioventricular septal defect | |
| Specialty | Medical genetics |
Symptoms and signs
Symptoms include difficulty breathing (dyspnoea) and bluish discoloration on skin and lips (cyanosis). A newborn baby will show signs of heart failure such as edema, fatigue, wheezing, sweating and irregular heartbeat.[1]
Complications
When there are holes in the septum that divide the four chambers of the heart the oxygen-rich blood and oxygen-poor blood mix this creates more stress on the heart to pump blood to where oxygen is needed. As a result, you get enlargement of the heart, heart failure (being unable to adequately supply body with needed oxygen), pulmonary hypertension, and pneumonia.[1]
The development of pulmonary hypertension is very serious. And this because the left ventricle is weakened due to its overuse. When this happens, the pressure backs up into the pulmonary veins and the lungs.[1] This type of damage is irreversible which is why immediate treatment is recommended after diagnosis.[2]
Associated conditions
Down syndrome is often associated with AVCD.[3] Other risk factors include: having a parent with a congenital heart defect, alcohol use while pregnant, uncontrolled diabetes treatment during pregnancy and some medications during pregnancy.[1]
This type of congenital heart defect is associated with patients with Down syndrome (trisomy 21) or heterotaxy syndromes.[4] 45% of children with Down syndrome have congenital heart disease. Of these, 35–40% have AV septal defects.[5] Similarly, one-third of all children born with AVSDs also have Down syndrome.[6]
A study also showed that there is also an increased risk of atrioventricular canal in patients who have Noonan syndrome. The pattern seen in those patients with Noonan syndrome differ from those patients who have Down syndrome in that "partial" AVCD is more prevalent in those with NS, whereas those with down syndrome show a prevalence of the "complete" form of AVCD.[7]
Pathophysiology
If there is a defect in the septum, it is possible for blood to travel from the left side of the heart to the right side of the heart, or the other way around. Since the right side of the heart contains venous blood with a low oxygen content, and the left side of the heart contains arterial blood with a high oxygen content, it is beneficial to prevent any communication between the two sides of the heart and prevent the blood from the two sides of the heart from mixing with each other.
Genetic Relationship
TBX2 is a T-box transcription factor and is usually expressed during various areas of embryogenesis. One notable expression is when it is shown in the development of the outflow system and atrioventricular canal of the developing heart.
In a study, they used targeted mutagenesis in mice to delete Tbx2 locus in some specimen. The results showed that mice who were homozygous and heterozygous null (+/+ & +/-) for Tbx2 resulted in the development of a healthier heart, while those who were homozygous null (-/-) for Tbx2 died early because of the inability of the heart to supply the body. It showed that there was insufficient formation of the endocardial cushion. There was a clear abnormality not only in the atrioventricular canal but also in the left ventricle. This study supports the fact that Tbx2 expression is important in the development of proper chamber differentiation, and in turn cannot have a direct relation to the development of atrioventricular canal defect.[8]
Diagnosis

AVSDs can be detected by cardiac auscultation; they cause atypical murmurs and loud heart tones. Confirmation of findings from cardiac auscultation can be obtained with a cardiac ultrasound (echocardiography - less invasive) and cardiac catheterization (more invasive).
Tentative diagnosis can also be made in utero via fetal echocardiogram. An AVSD diagnosis made before birth is a marker for Down syndrome, although other signs and further testing are required before any definitive confirmation of either can be made.
Classification
A variety of different classifications have been used, but the defects are usefully divided into "partial" and "complete" forms.
- In the partial AVSD, there is a defect in the primum or inferior part of the atrial septum but no direct intraventricular communication (ostium primum defect).
- In the complete AVSD (CAVSD), there is a large ventricular component beneath either or both the superior or inferior bridging leaflets of the AV valve. The defect involves the whole area of the junction of the upper and lower chambers of the heart, i.e. where the atria join the ventricles. There is a large hole between the lower portion of the atria and the upper or 'inlet' portion of the ventricles and this is associated with a significant abnormality of the valves separating the atria from the ventricles. The valves in effect become a common atrio-ventricular valve, and the severity of the defect depends largely on the supporting attachments of the valve to the ventricles and whether the valve allows dominant flow from the right atrium to right ventricle and from left atrium to left ventricle ("unbalanced" flow). The overall problems are similar to those of VSD but are more complicated. There is an increased flow of blood to the lungs through both the ventricular and atrial components of the defect. In addition, the abnormal atrio-ventricular valve invariably leaks, so that when the ventricles contract, blood flows not only forwards to the body and the lungs, but also backwards into the atria. The back-pressure effect on the atria causes congestion of blood in the left atrium in particular, and this in turn causes congestion in the veins draining the lungs. The effect on the baby is to worsen the heart failure that is associated with an isolated VSD and to hasten the onset of pulmonary hypertension. It should be mentioned that CAVSD is found in approximately one-third of babies who have Down syndrome, but it also occurs as an isolated abnormality.
Treatment
Treatment is surgical and involves closure of the atrial and ventricular septal defects and restoration of a competent left AV valve as far as is possible. Open surgical procedures require a heart-lung machine and are done with a median sternotomy. Surgical mortality for uncomplicated ostium primum defects in experienced centers is 2%; for uncomplicated cases of complete atrioventricular canal defect, 4% or less. Certain complications such as tetralogy of Fallot or highly unbalanced flow across the common AV valve can increase risk significantly.[9][10]
Infants born with AVSD are generally in sufficient health to not require immediate corrective surgery. If surgery is not required immediately after birth, the newborn will be closely monitored for the next several months, and the operation held-off until the first signs of lung distress or heart failure. This gives the infant time to grow, increasing the size of, and thereby the ease of operation on, the heart, as well as the ease of recovery. Infants will generally require surgery within three to six months, however, they may be able to go up to two years before the operation becomes necessary, depending on the severity of the defect.[11]
See also
References
- Mayo Clinic September 12, 2012"Atrioventricular Canal Defect" http://www.mayoclinic.com/health/atrioventricular-canal-defect/DS00745
- Calabrò R, Limongelli G (2006). "Complete atrioventricular canal". Orphanet J Rare Dis. 1: 8. doi:10.1186/1750-1172-1-8. PMC 1459121. PMID 16722604.
- Irving, Claire A.; Chaudhari, Milind P. (April 2012). "Cardiovascular abnormalities in Down's syndrome: spectrum, management and survival over 22 years". Archives of Disease in Childhood. 97 (4): 326–330. doi:10.1136/adc.2010.210534. ISSN 1468-2044. PMID 21835834.
- Report of the New England Regional Infant Cardiac Program" Pediatrics 1980;65(suppl):441–444.
- Al-Hay AA, et al. (2003). "Complete atrioventricular septal defect, Down syndrome and surgical outcome: Risk factors". Ann Thorac Surg. 75 (2): 412–421. doi:10.1016/s0003-4975(02)04026-2. PMID 12607648.
- Children's National Health System. (2019). Pediatric Atrioventricular Canal (AV canal or AVC). [online] Available at: https://childrensnational.org/choose-childrens/conditions-and-treatments/heart/atrioventricular-canal-av-canal-or-avc [Accessed 5 Feb. 2019].
- Marino Bruno (1999). "Congenital Heart Diseases in Children with Noonan Syndrome: An expanded cardiac spectrum with high prevalence of Atrioventricular Canal". The Journal of Pediatrics. 135 (6): 703–706. doi:10.1016/S0022-3476(99)70088-0. PMID 10586172.
- Harrelson, Zachary "Tbx2 is Essential for Patterning the Atrioventricular Canal and for Morphogenesis of the Outflow Tract During Heart Development" 2004 October 15, The Company of Biologists http://dev.biologists.org/content/131/20/5041.full
- Kirklin J, Barratt-Boyes B, ed. Cardiac Surgery, New York: Wiley, 1986:463–497.
- Marx, GR, Fyler DC, "Endiocardial Cusion Defects", in Keane, JF, Lock, JE, Fyler DC ed. Nadas' Pediatric Cardiology 2ed., Philadelphia: Saunders-Elsevier, 2006:663-674..
- Hay, WW, et al. 2007. Lange Current Pediatric Diagnosis and Treatment, 18th ed. New York: McGraw-Hill.