Calcium metabolism
Calcium metabolism is the movement and regulation of calcium ions (Ca2+) in (via the gut) and out (via the gut and kidneys) of the body, and between body compartments: the blood plasma, the extracellular and intracellular fluids, and bone. Bone acts as a calcium storage center for deposits and withdrawals as needed by the blood via continual bone remodeling.[1]: 276–277
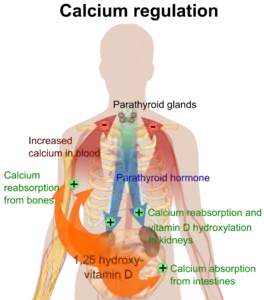
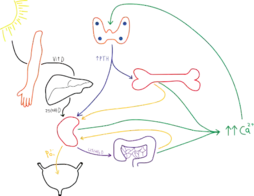
An important aspect of calcium metabolism is plasma calcium homeostasis, the regulation of calcium ions in the blood plasma within narrow limits.[2] The level of the calcium in plasma is regulated by the hormones parathyroid hormone (PTH) and calcitonin. PTH is released by the chief cells of the parathyroid glands when the plasma calcium level falls below the normal range in order to raise it; calcitonin is released by the parafollicular cells of the thyroid gland when the plasma level of calcium is above the normal range in order to lower it.
Body compartment content
Calcium is the most abundant mineral in the human body.[3] The average adult body contains in total approximately 1 kg, 99% in the skeleton in the form of calcium phosphate salts.[3] The extracellular fluid (ECF) contains approximately 22 mmol, of which about 9 mmol is in the plasma.[4] Approximately 10 mmol of calcium is exchanged between bone and the ECF over a period of twenty-four hours.[5]
Blood concentration
The concentration of calcium ions inside cells (in the intracellular fluid) is more than 7,000 times lower than in the blood plasma (i.e. at <0.0002 mmol/L, compared with 1.4 mmol/L in the plasma)
Normal plasma levels
The plasma total calcium concentration is in the range of 2.2–2.6 mmol/L (9–10.5 mg/dL), and the normal ionized calcium is 1.3–1.5 mmol/L (4.5–5.6 mg/dL).[4] The amount of total calcium in the blood varies with the level of plasma albumin, the most abundant protein in plasma, and therefore the main carrier of protein-bound calcium in the blood. The biologic effect of calcium is, however, determined by the amount of ionized calcium, rather than the total calcium. It is therefore the plasma ionized calcium level which is tightly regulated to remain within very narrow limits by homeostatic negative feedback systems.
Between 35 and 50% of the calcium in plasma is protein-bound, and 5–10% is in the form of complexes with organic acids and phosphates. The remainder (50–60%) is ionized. The ionized calcium can be determined directly by colorimetry, or it can be read off from nomograms, though the usefulness of the latter is limited when the pH and protein content of the plasma deviate widely from the normal.[4]
Function
Calcium has several main functions in the body.
Bound to serum proteins
It readily binds to proteins, particularly those with amino acids whose side chains terminate in carboxyl (-COOH) groups (e.g. glutamate residues). When such binding occurs the electrical charges on the protein chain change, causing the protein's tertiary structure (i.e. 3-dimensional form) to change. Good examples of this are several of the clotting factors in the blood plasma, which are functionless in the absence of calcium ions, but become fully functional on the addition of the correct concentration of calcium salts.
Voltage gated sodium channels
The voltage gated sodium ion channels in the cell membranes of nerves and muscle are particularly sensitive to the calcium ion concentration in the plasma.[6] Relatively small decreases in the plasma ionized calcium levels (hypocalcemia) cause these channels to leak sodium into the nerve cells or axons, making them hyper-excitable (positive bathmotropic effect), thus causing spontaneous muscle spasms (tetany) and paraesthesia (the sensation of "pins and needles") of the extremities and round the mouth.[7] When the plasma ionized calcium rises above normal (hypercalcemia) more calcium is bound to these sodium channels having a negative bathmotropic effect on them, causing lethargy, muscle weakness, anorexia, constipation and labile emotions.[7]
Intracellular signalling
Because the intracellular calcium ion concentration is extremely low (see above) the entry of minute quantities of calcium ions from the endoplasmic reticulum or from the extracellular fluids, cause rapid, very marked, and readily reversible changes in the relative concentration of these ions in the cytosol. This can therefore serve as a very effective intracellular signal (or "second messenger") in a variety of circumstances, including muscle contraction, the release of hormones (e.g. insulin from the beta cells in the pancreatic islets) or neurotransmitters (e.g. acetylcholine from pre-synaptic terminals of nerves) and other functions.
Bone
Calcium acts structurally as supporting material in bones as calcium hydroxyapatite (Ca10(PO4)6(OH)2).
Muscle
In skeletal and heart muscle, calcium ions, released from the sarcoplasmic reticulum (the endoplasmic reticulum of striated muscles), bind to the troponin C protein present on the actin-containing thin filaments of the myofibrils. The troponin's 3D structure changes as a result, causing the tropomyosin to which it is attached to be rolled away from the myosin-binding sites on the actin molecules that form the back-bone of the thin filaments. Myosin can then bind to the exposed myosin-binding sites on the thin filament, to undergo a repeating series of conformational changes called the cross-bridge cycle, for which ATP provides the energy. During the cycle, each myosin protein ‘paddles’ along the thin actin filament, repeatedly binding to myosin-binding sites along the actin filament, ratcheting and letting go. In effect, the thick filament moves or slides along the thin filament, resulting in muscle contraction. This process is known as the sliding filament model of muscle contraction.[8][9][10][11][12]
Sources
Not all the calcium in the diet can be readily absorbed from the gut. The calcium that is most readily absorbed is found in dairy products (72%), vegetables (7%), grains (5%), legumes (4%), fruit (3%), protein (3%). The calcium contained in vegetable matter is often complexed with phytates,[13] oxalates,[14] citrate and other organic acids, such as the long-chained fatty acids (e.g. palmitic acid), with which calcium binds to form insoluble calcium soaps.[15]
Bone storage
Calcium flow to and from the bone may be positive, negative, or neutral. When it is neutral, about 5–10 mmol is turned over a day. Bone serves as an important storage point for calcium, as it contains 99% of the total body calcium. Calcium release from bone is regulated by parathyroid hormone in conjunction with calcitriol manufactured in the kidney under the influence of PTH. Calcitonin (a hormone secreted by the thyroid gland when plasma ionized calcium levels are high or rising; not to be confused with "calcitriol" which is manufactured in the kidney) stimulates incorporation of calcium into bone.
Intestinal absorption
The normal adult diet contains about 25 mmol of calcium per day. Only about 5 mmol of this is absorbed into the body per day (see below).[16]
Calcium is absorbed across the intestinal epithelial cell's brush border membrane. The TRPV6 channel was proposed to be the major player in intestinal Ca2+ uptake.[17] However, Trpv6 KO mice didn't display significant reduction of serum calcium levels and showed only slightly reduced [17] or even unchanged intestinal Ca2+ absorption,[18][19] indicating that other absorption pathways must exist. Recently, TRPM7 was linked to intestinal calcium uptake. The authors could show that intestinal deletion of TRPM7 results in strongly reduced calcium levels in serum and bones,[20] and intensively increased levels of calcitriol and PTH, indicating that TRPM7 is essential for the intestinal bulk uptake of calcium. After the cellular uptake, calcium is immediately bound to calbindin, a vitamin D-dependent calcium-binding protein. Calbindin transfers the calcium directly into the epithelial cell's endoplasmic reticulum, through which the calcium is transferred to the basal membrane on the opposite side of the cell, without entering its cytosol or intracellular fluid. From there calcium pumps (PMCA1) actively transport calcium into the body.[21] Active transport of calcium occurs primarily in the duodenum portion of the intestine when calcium intake is low; and through passive paracellular transport in the jejunum and ileum parts when calcium intake is high, independently of Vitamin D level.[22]
The active absorption of calcium from the gut is regulated by the calcitriol (or 1,25 dihydroxycholecalciferol, or 1,25 dihydroxyvitamin D3) concentration in the blood. Calcitriol is a cholesterol derivative. Under the influence of ultraviolet light on the skin, cholesterol is converted to previtamin D3 which spontaneously isomerizes to vitamin D3 (or cholecalciferol). It is then converted from cholecalciferol to calcifediol in the liver.[23] Under the influence of parathyroid hormone, the kidneys convert calcifediol into the active hormone calcitriol, which acts on the epithelial cells (enterocytes) lining the small intestine to increase the rate of absorption of calcium from the intestinal contents. In short the cycle is following:
Cholesterol Previtamin D3 Vitamin D3 Calcifediol Calcitriol
Low PTH levels in the blood (which occur under physiological conditions when the plasma ionized calcium levels are high) inhibit the conversion of cholecalciferol into calcitriol, which in turn inhibits calcium absorption from the gut. The opposite happens when the plasma ionized calcium levels are low: parathyroid hormone is secreted into the blood and the kidneys convert more calcifediol into the active calcitriol, increasing calcium absorption from the gut.[24]

Intestine
Since about 15 mmol of calcium is excreted into the intestine via the bile per day,[4] the total amount of calcium that reaches the duodenum and jejunum each day is about 40 mmol (25 mmol from the diet plus 15 mmol from the bile), of which, on average, 20 mmol is absorbed (back) into the blood. The net result is that about 5 mmol more calcium is absorbed from the gut than is excreted into it via the bile. If there is no active bone building (as in childhood), or increased need for calcium during pregnancy and lactation, the 5 mmol calcium that is absorbed from the gut makes up for urinary losses that are only partially regulated.[16]
Kidneys
The kidneys filter 250 mmol of calcium ions a day in pro-urine (or glomerular filtrate), and resorbs 245 mmol, leading to a net average loss in the urine of about 5 mmol/d. The quantity of calcium ions excreted in the urine per day is partially under the influence of the plasma parathyroid hormone (PTH) level - high levels of PTH decreasing the rate of calcium ion excretion, and low levels increasing it.[note 1] However, parathyroid hormone has a greater effect on the quantity of phosphate ions (HPO42−) excreted in the urine.[25] Phosphates form insoluble salts in combination with calcium ions. High concentrations of HPO42− in the plasma, therefore, lower the ionized calcium level in the extra-cellular fluids. Thus, the excretion of more phosphate than calcium ions in the urine raises the plasma ionized calcium level, even though the total calcium concentration might be lowered.
The kidney influences the plasma ionized calcium concentration in yet another manner. It processes vitamin D3 into calcitriol, the active form that is most effective in promoting the intestinal absorption of calcium. This conversion of vitamin D3 into calcitriol, is also promoted by high plasma parathyroid hormone levels.[24][26]
Excretion
Intestine
Most excretion of excess calcium is via the bile and feces, because the plasma calcitriol levels (which ultimately depend on the plasma calcium levels) regulate how much of the biliary calcium is reabsorbed from the intestinal contents.
Kidneys
Urinary excretion of calcium is normally about 5 mmol (200 mg) /day. This is less in comparison to what is excreted via the feces (15 mmol/day).
Regulation
The plasma ionized calcium concentration is regulated within narrow limits (1.3–1.5 mmol/L). This is achieved by both the parafollicular cells of the thyroid gland, and the parathyroid glands constantly sensing (i.e. measuring) the concentration of calcium ions in the blood flowing through them.
High plasma level
When the concentration of calcium rises, the parafollicular cells of the thyroid gland increase their secretion of calcitonin, a polypeptide hormone, into the blood. At the same time, the parathyroid glands reduce the secretion of parathyroid hormone (PTH), also a polypeptide hormone, into the blood. The resulting high levels of calcitonin in the blood stimulate osteoblasts in bone to remove calcium from blood plasma and deposit it as bone.
The reduced levels of PTH inhibit removal of calcium from the skeleton. The low levels of PTH have several other effects: there is increased loss of calcium in the urine, but more importantly, the loss of phosphate ions through urine is inhibited. Phosphate ions will therefore be retained in the plasma where they form insoluble salts with calcium ions, thereby removing them from the ionized calcium pool in the blood. The low levels of PTH also inhibit the formation of calcitriol (not to be confused with calcitonin) from cholecalciferol (vitamin D3) by the kidneys.
The reduction in the blood calcitriol concentration acts (comparatively slowly) on the epithelial cells (enterocytes) of the duodenum, inhibiting their ability to absorb calcium from the intestinal contents.[2][5][28][29] The low calcitriol levels also act on bone causing the osteoclasts to release fewer calcium ions into the blood plasma.[25]
Low plasma level
When the plasma ionized calcium level is low or falls the opposite happens. Calcitonin secretion is inhibited and PTH secretion is stimulated, resulting in calcium being removed from bone to rapidly correct the plasma calcium level. The high plasma PTH levels inhibit calcium loss via the urine while stimulating the excretion of phosphate ions via that route. They also stimulate the kidneys to manufacture calcitriol (a steroid hormone), which enhances the ability of the cells lining the gut to absorb calcium from the intestinal contents into the blood, by stimulating the production of calbindin in these cells. The PTH stimulated production of calcitriol also causes calcium to be released from bone into the blood, by the release of RANKL (a cytokine, or local hormone) from the osteoblasts which increases the bone resorptive activity by the osteoclasts. These are, however, relatively slow processes[2][5][25][28][29]
Thus fast short term regulation of the plasma ionized calcium level primarily involves rapid movements of calcium into or out of the skeleton. Long term regulation is achieved by regulating the amount of calcium absorbed from the gut or lost via the feces.[2][5][28][29]
Disorders
Hypocalcemia (low blood calcium) and hypercalcemia (high blood calcium) are both serious medical disorders. Osteoporosis, osteomalacia and rickets are bone disorders linked to calcium metabolism disorders and effects of vitamin D. Renal osteodystrophy is a consequence of chronic kidney failure related to the calcium metabolism.
A diet adequately rich in calcium may reduce calcium loss from bone with advancing (post-menopausal) age.[30] A low dietary calcium intake may be a risk factor in the development of osteoporosis in later life; and a diet with sustained adequate amounts of calcium may reduce the risk of osteoporosis.
Research
The role that calcium might have in reducing the rates of colorectal cancer has been the subject of many studies. However, given its modest efficacy, there is no current medical recommendation to use calcium for cancer reduction.
See also
Footnotes
- The main determinant of the amount of calcium excreted into the urine per day is the plasma ionized calcium concentration. The plasma parathyroid hormone (PTH) concentration only increases or decreases the amount of calcium excreted at any given plasma ionized calcium concentration. Thus, in primary hyperparathyroidism the quantity of calcium excreted in the urine per day is increased despite the high levels of PTH in the blood. This is because hyperparathyroidism results in hypercalcemia, which increases the urinary calcium concentration (hypercalcuria) despite the modestly increased rate of calcium re-absorption from the renal tubules caused by PTH's effect on those tubules. Kidney stones are therefore often a first indication of hyperparathyroidism, especially since the hypercalcuria is accompanied by an increase in urinary phosphate excretion (a direct result of the high plasma PTH levels). Together the calcium and phosphate tend to precipitate out as water-insoluble salts, which readily form solid “stones”.
References
- Marieb, Elaine (2000), Essentials of human anatomy and physiology, San Francisco: Benjamin Cummings, ISBN 978-0805349405
- Brini M, Ottolini D, Calì T, Carafoli E (2013). "Chapter 4. Calcium in Health and Disease". In Sigel A, Helmut RK (eds.). Interrelations between Essential Metal Ions and Human Diseases. Metal Ions in Life Sciences. Vol. 13. Springer. pp. 81–137. doi:10.1007/978-94-007-7500-8_4. ISBN 978-94-007-7499-5. PMID 24470090.
- Peacock, Munro (2010-01-01). "Calcium Metabolism in Health and Disease". Clinical Journal of the American Society of Nephrology. 5 (Supplement 1): S23–S30. doi:10.2215/CJN.05910809. ISSN 1555-9041. PMID 20089499.
- Diem K, Lenter C. Scientific Tables. Vol. 565 (Seventh ed.). Basel: Ciba-Geigy Limited. pp. 653–654. ISBN 978-3-9801244-0-9.
- Marshall, W. J. (1995). Clinical Chemistry (3rd ed.). London: Mosby. ISBN 978-0-7234-2190-0.
- Armstrong CM, Cota G (Mar 1999). "Calcium block of Na+ channels and its effect on closing rate". Proceedings of the National Academy of Sciences of the United States of America. 96 (7): 4154–7. Bibcode:1999PNAS...96.4154A. doi:10.1073/pnas.96.7.4154. PMC 22436. PMID 10097179.
- Harrison TR. Principles of Internal Medicine (third ed.). New York: McGraw-Hill Book Company. pp. 170, 571–579.
- Silverthorn, Dee Unglaub (2016). "Muscles". Human Physiology: An Integrated Approach (7th ed.). San Francisco, CA: Pearson. pp. 377–416. ISBN 978-0-321-98122-6.
- Cooke R (June 2004). "The sliding filament model: 1972-2004". The Journal of General Physiology. 123 (6): 643–56. doi:10.1085/jgp.200409089. PMC 2234572. PMID 15173218.
- Geeves MA (January 2002). "Stretching the lever-arm theory". Nature. 415 (6868): 129–31. Bibcode:2002Natur.415..129G. doi:10.1038/415129a. PMID 11805818. S2CID 30618615.
- Spudich JA (November 1989). "In pursuit of myosin function". Cell Regulation. 1 (1): 1–11. doi:10.1091/mbc.1.1.1. PMC 361420. PMID 2519609.
- Yanagida T, Arata T, Oosawa F (1985). "Sliding distance of actin filament induced by a myosin crossbridge during one ATP hydrolysis cycle". Nature. 316 (6026): 366–9. Bibcode:1985Natur.316..366Y. doi:10.1038/316366a0. PMID 4022127. S2CID 4352361.
- Graf E (1983). "Calcium binding to phytic acid". Journal of Agricultural and Food Chemistry. 31 (4): 851–855. doi:10.1021/jf00118a045.
- Watts PS (2009). "Effects of oxalic acid ingestion by sheep. II. Large doses to sheep on different diets". The Journal of Agricultural Science. 52 (2): 250–255. doi:10.1017/S0021859600036765.
- López-López A, Castellote-Bargalló AI, Campoy-Folgoso C, Rivero-Urgël M, Tormo-Carnicé R, Infante-Pina D, López-Sabater MC (Nov 2001). "The influence of dietary palmitic acid triacylglyceride position on the fatty acid, calcium and magnesium contents of at term newborn faeces". Early Human Development. 65 Suppl: S83–94. doi:10.1016/S0378-3782(01)00210-9. PMID 11755039.
- Barrett KE, Barman SM, Boitano S, Brooks H, "Chapter 23. Hormonal Control of Calcium & Phosphate Metabolism & the Physiology of Bone" (Chapter). Barrett KE, Barman SM, Boitano S, Brooks H: Ganong's Review of Medical Physiology, 23e: http://www.accessmedicine.com/content.aspx?aID=5244785 Archived 2011-07-07 at the Wayback Machine.
- Bianco SD, Peng JB, Takanaga H, Suzuki Y, Crescenzi A, Kos CH, Zhuang L, Freeman MR, Gouveia CH, Wu J, Luo H, Mauro T, Brown EM, Hediger MA (February 2007). "Marked disturbance of calcium homeostasis in mice with targeted disruption of the Trpv6 calcium channel gene". Journal of Bone and Mineral Research. 22 (2): 274–85. doi:10.1359/jbmr.061110. PMC 4548943. PMID 17129178.
- Sylvia, Benn, Bryan S. Ajibade, Dare Porta, Angela Dhawan, Puneet Hediger, Matthias Peng, Ji-Bin Jiang, Yi Oh, Goo Taeg Jeung, Eui-Bae Lieben, Liesbet Bouillon, Roger Carmeliet, Geert Christakos. Active Intestinal Calcium Transport in the Absence of Transient Receptor Potential Vanilloid Type 6 and Calbindin-D9k. The Endocrine Society. OCLC 680131487.
- Kutuzova GD, Sundersingh F, Vaughan J, Tadi BP, Ansay SE, Christakos S, Deluca HF (December 2008). "TRPV6 is not required for 1alpha,25-dihydroxyvitamin D3-induced intestinal calcium absorption in vivo". Proceedings of the National Academy of Sciences of the United States of America. 105 (50): 19655–9. Bibcode:2008PNAS..10519655K. doi:10.1073/pnas.0810761105. PMC 2605002. PMID 19073913.
- Mittermeier L, Demirkhanyan L, Stadlbauer B, Breit A, Recordati C, Hilgendorff A, Matsushita M, Braun A, Simmons DG, Zakharian E, Gudermann T, Chubanov V (February 2019). "TRPM7 is the central gatekeeper of intestinal mineral absorption essential for postnatal survival" (PDF). Proceedings of the National Academy of Sciences of the United States of America. 116 (10): 4706–4715. doi:10.1073/pnas.1810633116. PMC 6410795. PMID 30770447.
- Balesaria S, Sangha S, Walters JR (December 2009). "Human duodenum responses to vitamin D metabolites of TRPV6 and other genes involved in calcium absorption". American Journal of Physiology. Gastrointestinal and Liver Physiology. 297 (6): G1193-7. doi:10.1152/ajpgi.00237.2009. PMC 2850091. PMID 19779013.
- "Absorption of Minerals and Metals". www.vivo.colostate.edu. Retrieved 19 April 2018.
- Brandi, M.L. (2010). "Indications on the use of vitamin D and vitamin D metabolites in clinical phenotypes". Clinical Cases in Mineral and Bone Metabolism. 7 (3): 243–250. ISSN 1724-8914. PMC 3213838. PMID 22460535.
- Stryer L. Biochemistry (Fourth Edition). Chapter 27 "Vitamin D is derived from cholesterol by the ring-splitting action of light". New York, W.H. Freeman and Company.
- Blaine J, Chonchol M, Levi M (2015). "Renal control of calcium, phosphate, and magnesium homeostasis". Clinical Journal of the American Society of Nephrology. 10 (7): 1257–72. doi:10.2215/CJN.09750913. PMC 4491294. PMID 25287933.
- Tortora GJ, Anagnostakos NP. Principles of Anatomy and Physiology (Fifth Edition) p. 696. New York, Harper & Row Publishers.
- Boron, Walter F.; Boulpaep, Emile L (2003). "The Parathyroid Glands and Vitamin D". Medical Physiology: A Cellular And Molecular Approach. Elsevier/Saunders. p. 1094. ISBN 978-1-4160-2328-9.
- Walter F. (2003). "The Parathyroid Glands and Vitamin D in". Medical Physiology: A Cellular And Molecular Approach. Elsevier/Saunders. p. 1094. ISBN 978-1-4160-2328-9.
- Guyton A (1976). ‘’Medical Physiology’’. p.1062; New York, Saunders and Co.
- Heaney RP (Apr 2000). "Calcium, dairy products and osteoporosis". Journal of the American College of Nutrition. 19 (2 Suppl): 83S–99S. doi:10.1080/07315724.2000.10718088. PMID 10759135. S2CID 18794160. Archived from the original on 2012-08-03.
External links
- Calcium at Lab Tests Online
- Nosek, Thomas M. "Section 5/5ch6/5ch6line". Essentials of Human Physiology.