Intracerebral hemorrhage
Intracerebral hemorrhage (ICH), also known as cerebral bleed, intraparenchymal bleed, and hemorrhagic stroke, or haemorrhagic stroke, is a sudden bleeding into the tissues of the brain, into its ventricles, or into both.[3][4][1] It is one kind of bleeding within the skull[3] and one kind of stroke.[4] Symptoms can include headache, one-sided weakness, vomiting, seizures, decreased level of consciousness, and neck stiffness.[2] Often, symptoms get worse over time.[1] Fever is also common.[1]
| Intracerebral hemorrhage | |
|---|---|
| Other names | Cerebral haemorrhage, cerebral hemorrhage, intra-axial hemorrhage, cerebral hematoma, cerebral bleed, brain bleed |
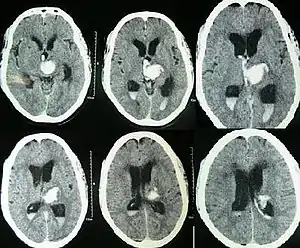
.jpg.webp) | |
| CT scan of a spontaneous intracerebral bleed, leaking into the lateral ventricles | |
| Specialty | Neurosurgery |
| Symptoms | Headache, one-sided weakness, vomiting, seizures, decreased level of consciousness, neck stiffness, fever[1][2] |
| Causes | Brain trauma, aneurysms, arteriovenous malformations, brain tumors[1] |
| Risk factors | High blood pressure, amyloidosis, alcoholism, low cholesterol, blood thinners, cocaine use[2] |
| Diagnostic method | CT scan[1] |
| Differential diagnosis | Ischemic stroke[1] |
| Treatment | Blood pressure control, surgery, ventricular drain[1] |
| Prognosis | 20% good outcome[2] |
| Frequency | 2.5 per 10,000 people a year[2] |
| Deaths | 44% die within one month[2] |
Causes include brain trauma, aneurysms, arteriovenous malformations, and brain tumors.[1] The largest risk factors for spontaneous bleeding are high blood pressure and amyloidosis.[2] Other risk factors include alcoholism, low cholesterol, blood thinners, and cocaine use.[2] Diagnosis is typically by CT scan.[1] Other conditions that may present similarly include ischemic stroke.[1]
Treatment should typically be carried out in an intensive care unit.[1] Guidelines recommend decreasing the blood pressure to a systolic of 140 mmHg.[1][5] Blood thinners should be reversed if possible and blood sugar kept in the normal range.[1] Surgery to place a ventricular drain may be used to treat hydrocephalus, but corticosteroids should not be used.[1] Surgery to remove the blood is useful in certain cases.[1]
Cerebral bleeding affects about 2.5 per 10,000 people each year.[2] It occurs more often in males and older people.[2] About 44% of those affected die within a month.[2] A good outcome occurs in about 20% of those affected.[2] Intracerebral hemorrhage, a type of hemorrhagic stroke, was first distinguished from ischemic strokes due to insufficient blood flow, so called "leaks and plugs", in 1823.[6]
Signs and symptoms
People with intracerebral bleeding have symptoms that correspond to the functions controlled by the area of the brain that is damaged by the bleed.[7] These localizing signs and symptoms can include hemiplegia (or weakness localized to one side of the body) and paresthesia (loss of sensation) including hemisensory loss (if localized to one side of the body).[8] These symptoms are usually rapid in onset, sometimes occurring in minutes, but not as rapid as the symptom onset in ischemic stroke.[8] Other symptoms include those that indicate a rise in intracranial pressure caused by a large mass (due to hematoma expansion) putting pressure on the brain.[7] These symptoms include headaches, nausea, vomiting, a depressed level of consciousness, stupor and death.[8] Continued elevation in the intracranial pressure and the accompanying mass effect may eventually cause brain herniation (when different parts of the brain are displaced or shifted to new areas in relation to the skull and surrounding dura mater supporting structures). Brain herniation is associated with hyperventilation, extensor rigidity, pupillary asymmetry, pyramidal signs, coma and death.[9]
Hemorrhage into the basal ganglia or thalamus causes contralateral hemiplegia due to damage to the internal capsule.[8] Other possible symptoms include gaze palsies or hemisensory loss.[8] Intracerebral hemorrhage into the cerebellum may cause ataxia, vertigo, incoordination of limbs and vomiting.[8] Some cases of cerebellar hemorrhage lead to blockage of the fourth ventricle with subsequent impairment of drainage of cerebrospinal fluid from the brain.[8] The ensuing hydrocephalus, or fluid buildup in the ventricles of the brain leads to a decreased level of consciousness and coma.[8] Brainstem hemorrhage most commonly occurs in the pons and is associated with cranial nerve palsies, pinpoint (but reactive) pupils, gaze palsies, facial weakness, and coma (if there is damage to the reticular activating system).[8]
Causes

Intracerebral bleeds are the second most common cause of stroke, accounting for 10% of hospital admissions for stroke.[11] High blood pressure raises the risks of spontaneous intracerebral hemorrhage by two to six times.[10] More common in adults than in children, intraparenchymal bleeds are usually due to penetrating head trauma, but can also be due to depressed skull fractures. Acceleration-deceleration trauma,[12][13][14] rupture of an aneurysm or arteriovenous malformation (AVM), and bleeding within a tumor are additional causes. Amyloid angiopathy is not an uncommon cause of intracerebral hemorrhage in patients over the age of 55. A very small proportion is due to cerebral venous sinus thrombosis.
Risk factors for ICH include:[15]
- Hypertension (high blood pressure)
- Diabetes mellitus
- Menopause
- Excessive alcohol consumption
- Severe migraine
Hypertension is the strongest risk factor associated with intracerebral hemorrhage and long term control of elevated blood pressure has been shown to reduce the incidence of hemorrhage.[8] Cerebral amyloid angiopathy, a disease characterized by deposition of amyloid beta peptides in the walls of the small blood vessels of the brain, leading to weakened blood vessel walls and an increased risk of bleeding; is also an important risk factor for the development of intracerebral hemorrhage. Other risk factors include advancing age (usually with a concomitant increase of cerebral amyloid angiopathy risk in the elderly), use of anticoagulants or antiplatelet medications, the presence of cerebral microbleeds, chronic kidney disease, and low low density lipoprotein (LDL) levels (usually below 70).[16][17] The direct oral anticoagulants (DOACs) such as the factor Xa inhibitors or direct thrombin inhibitors are thought to have a lower risk of intracerebral hemorrhage as compared to the vitamin K antagonists such as warfarin.[8]
Cigarette smoking may be a risk factor but the association is weak.[18]
Traumautic intracerebral hematomas are divided into acute and delayed. Acute intracerebral hematomas occur at the time of the injury while delayed intracerebral hematomas have been reported from as early as 6 hours post injury to as long as several weeks.
Diagnosis
Both computed tomography angiography (CTA) and magnetic resonance angiography (MRA) have been proved to be effective in diagnosing intracranial vascular malformations after ICH.[19] So frequently, a CT angiogram will be performed in order to exclude a secondary cause of hemorrhage[20] or to detect a "spot sign".
Intraparenchymal hemorrhage can be recognized on CT scans because blood appears brighter than other tissue and is separated from the inner table of the skull by brain tissue. The tissue surrounding a bleed is often less dense than the rest of the brain because of edema, and therefore shows up darker on the CT scan.[20]
Location
When due to high blood pressure, intracerebral hemorrhages typically occur in the putamen (50%) or thalamus (15%), cerebrum (10–20%), cerebellum (10–13%), pons (7–15%), or elsewhere in the brainstem (1–6%).[21][22]
Treatment
Treatment depends substantially on the type of ICH. Rapid CT scan and other diagnostic measures are used to determine proper treatment, which may include both medication and surgery.
- Tracheal intubation is indicated in people with decreased level of consciousness or other risk of airway obstruction.[23]
- IV fluids are given to maintain fluid balance, using isotonic rather than hypotonic fluids.[23]
Medication
- One review found that antihypertensive therapy to bring down the blood pressure in acute phases appears to improve outcomes.[24] Other reviews found an unclear difference between intensive and less intensive blood pressure control.[25][26] The American Heart Association and American Stroke Association guidelines in 2015 recommended decreasing the blood pressure to a SBP of 140 mmHg.[1] However, the evidence finds tentative usefulness as of 2015.[25]
- Giving Factor VIIa within 4 hours limits the bleeding and formation of a hematoma. However, it also increases the risk of thromboembolism.[23] It thus overall does not result in better outcomes in those without hemophilia.[27]
- Frozen plasma, vitamin K, protamine, or platelet transfusions may be given in case of a coagulopathy.[23] Platelets however appear to worsen outcomes in those with spontaneous intracerebral bleeding on antiplatelet medication.[28]
- The specific reversal agents idarucizumab and andexanet alfa may be used to stop continued intracerebral hemorrhage in people taking directly oral acting anticoagulants (such as factor Xa inhibitors or direct thrombin inhibitors).[8] However, if these specialized medications are not available, prothrombin complex concentrate may also be used.[8]
- Fosphenytoin or other anticonvulsant is given in case of seizures or lobar hemorrhage.[23]
- H2 antagonists or proton pump inhibitors are commonly given for to try to prevent stress ulcers, a condition linked with ICH.[23]
- Corticosteroids, were thought to reduce swelling. However, in large controlled studies, corticosteroids have been found to increase mortality rates and are no longer recommended.[29][30]
Surgery
Surgery is required if the hematoma is greater than 3 cm (1 in), if there is a structural vascular lesion or lobar hemorrhage in a young patient.[23]
- A catheter may be passed into the brain vasculature to close off or dilate blood vessels, avoiding invasive surgical procedures.[31]
- Aspiration by stereotactic surgery or endoscopic drainage may be used in basal ganglia hemorrhages, although successful reports are limited.[23]
- A craniectomy may take place, where part of the skull is removed to allow a swelling brain room to expand without being squeezed.
Prognosis
The risk of death from an intraparenchymal bleed in traumatic brain injury is especially high when the injury occurs in the brain stem.[32] Intraparenchymal bleeds within the medulla oblongata are almost always fatal, because they cause damage to cranial nerve X, the vagus nerve, which plays an important role in blood circulation and breathing.[12] This kind of hemorrhage can also occur in the cortex or subcortical areas, usually in the frontal or temporal lobes when due to head injury, and sometimes in the cerebellum.[12][33] Larger volumes of hematoma at hospital admission as well as greater expansion of the hematoma on subsequent evaluation (usually occurring within 6 hours of symptom onset) are associated with a worse prognosis.[8][34] Perihematomal edema, or secondary edema surrounding the hematoma, is associated with secondary brain injury, worsening neurological function and is associated with poor outcomes.[8] Intraventricular hemorrhage, or bleeding into the ventricles of the brain, which may occur in 30-50% of patients, is also associated with long term disability and a poor prognosis.[8] Brain herniation is associated with poor prognoses.[8]
For spontaneous intracerebral hemorrhage seen on CT scan, the death rate (mortality) is 34–50% by 30 days after the injury,[10] and half of the deaths occur in the first 2 days.[35] Even though the majority of deaths occurs in the first days after ICH, survivors have a long term excess mortality of 27% compared to the general population.[36] Of those who survive an intracerebral hemorrhage; 12-39% are independent with regards to self care, others are disabled to varying degrees and require supportive care.[37]
Epidemiology
The incidence of intracerebral hemorrhage is estimated at 24.6 cases per 100,000 person years with the incidence rate being similar in men and women.[8][37] The incidence is much higher in the elderly, especially those who are 85 or older, who are 9.6 times more likely to have an intracerebral hemorrhage as compared to those of middle age.[37] It accounts for 20% of all cases of cerebrovascular disease in the United States, behind cerebral thrombosis (40%) and cerebral embolism (30%).[38]
History
Intracerebral hemorrhage was first distinguished from strokes due to insufficient blood flow, so called "leaks and plugs", in 1823.[6] Franklin D. Roosevelt, the 32nd President of the United States, died from a cerebral hemorrhage in 1945 and so did Soviet dictator Joseph Stalin in 1953.
Research
The inflammatory response triggered by stroke has been viewed as harmful in the early stage, focusing on blood-borne leukocytes, neutrophils and macrophages, and resident microglia and astrocytes.[39][40] A human postmortem study shows that inflammation occurs early and persists for several days after ICH.[41] Modulating microglial activation and polarization might mitigate intracerebral hemorrhage-induced brain injury and improve brain repair.[42] A new area of interest is the role of mast cells in ICH.[40][43]
References
- Hemphill JC, 3rd; Greenberg, SM; Anderson, CS; Becker, K; Bendok, BR; Cushman, M; Fung, GL; Goldstein, JN; Macdonald, RL; Mitchell, PH; Scott, PA; Selim, MH; Woo, D; American Heart Association Stroke Council; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology (July 2015). "Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke: A Journal of Cerebral Circulation. 46 (7): 2032–60. doi:10.1161/str.0000000000000069. PMID 26022637.
- Caceres, JA; Goldstein, JN (August 2012). "Intracranial hemorrhage". Emergency Medicine Clinics of North America. 30 (3): 771–94. doi:10.1016/j.emc.2012.06.003. PMC 3443867. PMID 22974648.
- "Brain Bleed/Hemorrhage (Intracranial Hemorrhage): Causes, Symptoms, Treatment".
- Naidich, Thomas P.; Castillo, Mauricio; Cha, Soonmee; Smirniotopoulos, James G. (2012). Imaging of the Brain, Expert Radiology Series,1: Imaging of the Brain. Elsevier Health Sciences. p. 387. ISBN 978-1416050094. Archived from the original on 2016-10-02.
- Ko, SB; Yoon, BW (December 2017). "Blood Pressure Management for Acute Ischemic and Hemorrhagic Stroke: The Evidence". Seminars in Respiratory and Critical Care Medicine. 38 (6): 718–725. doi:10.1055/s-0037-1608777. PMID 29262429.
- Hennerici, Michael (2003). Imaging in Stroke. Remedica. p. 1. ISBN 9781901346251. Archived from the original on 2016-10-02.
- Vinas FC and Pilitsis J. 2006. "Penetrating Head Trauma." Archived 2005-09-13 at the Wayback Machine Emedicine.com.
- Sheth, Kevin N. (27 October 2022). "Spontaneous Intracerebral Hemorrhage". New England Journal of Medicine. 387 (17): 1589–1596. doi:10.1056/NEJMra2201449. PMID 36300975. S2CID 253159180.
- Kalita, J.; Misra, U. K.; Vajpeyee, A.; Phadke, R. V.; Handique, A.; Salwani, V. (April 2009). "Brain herniations in patients with intracerebral hemorrhage". Acta Neurologica Scandinavica. 119 (4): 254–260. doi:10.1111/j.1600-0404.2008.01095.x. PMID 19053952. S2CID 21870062.
- Yadav YR, Mukerji G, Shenoy R, Basoor A, Jain G, Nelson A (2007). "Endoscopic management of hypertensive intraventricular haemorrhage with obstructive hydrocephalus". BMC Neurol. 7: 1. doi:10.1186/1471-2377-7-1. PMC 1780056. PMID 17204141.
- Go AS, Mozaffarian D, Roger VL, et al. (January 2013). "Heart disease and stroke statistics—2013 update: a report from the American Heart Association". Circulation. 127 (1): e6–e245. doi:10.1161/CIR.0b013e31828124ad. PMC 5408511. PMID 23239837.
- McCaffrey P. 2001. "The Neuroscience on the Web Series: CMSD 336 Neuropathologies of Language and Cognition." Archived 2005-11-25 at the Wayback Machine California State University, Chico. Retrieved on June 19, 2007.
- Orlando Regional Healthcare, Education and Development. 2004. "Overview of Adult Traumatic Brain Injuries." Archived 2008-02-27 at the Wayback Machine Retrieved on 2008-01-16.
- Shepherd S. 2004. "Head Trauma." Archived 2005-10-26 at the Wayback Machine Emedicine.com. Retrieved on June 19, 2007.
- Feldmann, Edward; Broderick, Joseph P.; Kernan, Walter N.; Viscoli, Catherine M.; Brass, Lawrence M.; Brott, Thomas; Morgenstern, Lewis B.; Lee Wilterdink, Janet; Horwitz, Ralph I. (2005). "Major Risk Factors for Intracerebral Hamorrhage in the Young Are Modifiable". Stroke. 36 (9): 1881–5. doi:10.1161/01.str.0000177480.62341.6b. PMID 16081867.
- Ma, Chaoran; Gurol, M. Edip; Huang, Zhe; Lichtenstein, Alice H.; Wang, Xiuyan; Wang, Yuzhen; Neumann, Samantha; Wu, Shouling; Gao, Xiang (30 July 2019). "Low-density lipoprotein cholesterol and risk of intracerebral hemorrhage: A prospective study". Neurology. 93 (5): e445–e457. doi:10.1212/WNL.0000000000007853. PMC 6693427. PMID 31266905.
- An, Sang Joon; Kim, Tae Jung; Yoon, Byung-Woo (31 January 2017). "Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update". Journal of Stroke. 19 (1): 3–10. doi:10.5853/jos.2016.00864. PMC 5307940. PMID 28178408.
- Carhuapoma, J. Ricardo; Mayer, Stephan A.; Hanley, Daniel F. (2009). Intracerebral Hemorrhage. Cambridge University Press. p. 6. ISBN 978-0-521-87331-4.
- Josephson, Colin B; White, Philip M; Krishan, Ashma; Al-Shahi Salman, Rustum (1 September 2014). "Computed tomography angiography or magnetic resonance angiography for detection of intracranial vascular malformations in patients with intracerebral haemorrhage". The Cochrane Database of Systematic Reviews. 9 (9): CD009372. doi:10.1002/14651858.CD009372.pub2. PMC 6544803. PMID 25177839.
- Yeung R, Ahmad T, Aviv RI, Noel de Tilly L, Fox AJ, Symons SP (2009). "Comparison of CTA to DSA in determining the etiology of spontaneous ICH". Canadian Journal of Neurological Sciences. 36 (2): 176–180. doi:10.1017/s0317167100006533. PMID 19378710.
- Greenberg, Mark S. (2016). Handbook of Neurosurgery. ISBN 9781626232419.
- Prayson, Richard A. (2012). Neuropathology. Elsevier Health Sciences. p. 49. ISBN 978-1437709490. Archived from the original on 2017-03-12.
- eMedicine Specialties > Neurology > Neurological Emergencies > Intracranial Haemorrhage: Treatment & Medication. Archived 2009-03-12 at the Wayback Machine By David S Liebeskind, MD. Updated: Aug 7, 2006
- Tsivgoulis, G; Katsanos, AH; Butcher, KS; Boviatsis, E; Triantafyllou, N; Rizos, I; Alexandrov, AV (21 October 2014). "Intensive blood pressure reduction in acute intracerebral hemorrhage: A meta-analysis". Neurology. 83 (17): 1523–9. doi:10.1212/wnl.0000000000000917. PMID 25239836. S2CID 36315871.
- Ma, J; Li, H; Liu, Y; You, C; Huang, S; Ma, L (2015). "Effects of Intensive Blood Pressure Lowering on Intracerebral Hemorrhage Outcomes: A Meta-Analysis of Randomized Controlled Trials". Turkish Neurosurgery. 25 (4): 544–51. doi:10.5137/1019-5149.JTN.9270-13.0 (inactive 31 July 2022). PMID 26242330.
{{cite journal}}: CS1 maint: DOI inactive as of July 2022 (link) - Boulouis, Gregoire; Morotti, Andrea; Goldstein, Joshua N.; Charidimou, Andreas (1 April 2017). "Intensive blood pressure lowering in patients with acute intracerebral haemorrhage: clinical outcomes and haemorrhage expansion. Systematic review and meta-analysis of randomised trials". Journal of Neurology, Neurosurgery, and Psychiatry. 88 (4): 339–345. doi:10.1136/jnnp-2016-315346. ISSN 1468-330X. PMID 28214798. S2CID 25397701.
- Yuan, ZH; Jiang, JK; Huang, WD; Pan, J; Zhu, JY; Wang, JZ (June 2010). "A meta-analysis of the efficacy and safety of recombinant activated factor VII for patients with acute intracerebral hemorrhage without hemophilia". Journal of Clinical Neuroscience. 17 (6): 685–93. doi:10.1016/j.jocn.2009.11.020. PMID 20399668. S2CID 30590573.
- Al-Shahi Salman, R; Law, ZK; Bath, PM; Steiner, T; Sprigg, N (17 April 2018). "Haemostatic therapies for acute spontaneous intracerebral haemorrhage". The Cochrane Database of Systematic Reviews. 2018 (4): CD005951. doi:10.1002/14651858.CD005951.pub4. PMC 6494564. PMID 29664991.
- Roberts, Ian; Yates, David; Sandercock, Peter; Farrell, Barbara; Wasserberg, Jonathan (9 October 2016). "Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): randomised placebo-controlled trial". Lancet. 364 (9442): 1321–1328. doi:10.1016/S0140-6736(04)17188-2. ISSN 1474-547X. PMID 15474134. S2CID 30210176.
- Edwards, P; Arango, M; Balica, L; Cottingham, R; El-Sayed, H (2005). "Final results of MRC CRASH, a randomised placebo-controlled trial of intravenous corticosteroid in adults with head injury-outcomes at 6 months". Lancet. 365 (9475): 1957–9. doi:10.1016/s0140-6736(05)66552-x. PMID 15936423. S2CID 27713031.
- Cedars-Sinai Health System – Cerebral Hemorrhages Archived 2009-03-12 at the Wayback Machine Retrieved on 02/25/2009
- Sanders MJ and McKenna K. 2001. Mosby's Paramedic Textbook, 2nd revised Ed. Chapter 22, "Head and Facial Trauma." Mosby.
- Graham DI and Gennareli TA. Chapter 5, "Pathology of Brain Damage After Head Injury" Cooper P and Golfinos G. 2000. Head Injury, 4th Ed. Morgan Hill, New York.
- Broderick, J P; Brott, T G; Duldner, J E; Tomsick, T; Huster, G (1 July 1993). "Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality". Stroke. 24 (7): 987–993. doi:10.1161/01.STR.24.7.987. PMID 8322400. S2CID 3107793.
- Broderick, J.; Connolly, S.; Feldmann, E.; Hanley, D.; Kase, C.; Krieger, D.; Mayberg, M.; Morgenstern, L.; Ogilvy, C. S.; Vespa, P.; Zuccarello, M. (3 May 2007). "Guidelines for the Management of Spontaneous Intracerebral Hemorrhage in Adults: 2007 Update: A Guideline From the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists". Stroke. 38 (6): 2001–2023. doi:10.1161/strokeaha.107.183689. PMID 17478736.
- Hansen, B.M.; Nilsson O.G.; Anderson H; et al. (Oct 2013). "Long term (13 years) prognosis after primary intracerebral haemorrhage: a prospective population based study of long term mortality, prognostic factors and causes of death". Journal of Neurology, Neurosurgery & Psychiatry. 84 (10): 1150–1155. doi:10.1136/jnnp-2013-305200. PMID 23715913. S2CID 40379279. Archived from the original on 2014-02-22.
- Asch, Charlotte JJ van; Luitse, Merel JA; Rinkel, Gabriël JE; Tweel, Ingeborg van der; Algra, Ale; Klijn, Catharina JM (1 February 2010). "Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis". The Lancet Neurology. 9 (2): 167–176. doi:10.1016/S1474-4422(09)70340-0. PMID 20056489. S2CID 25364307.
- Page 117 in: Henry S. Schutta; Lechtenberg, Richard (1998). Neurology practice guidelines. New York: M. Dekker. ISBN 978-0-8247-0104-8.
- Wang J (December 2010). "Preclinical and clinical research on inflammation after intracerebral hemorrhage". Prog. Neurobiol. 92 (4): 463–77. doi:10.1016/j.pneurobio.2010.08.001. PMC 2991407. PMID 20713126.
- Ren H, Han R, Chen X, Liu X, Wan J, Wang L, Yang X, Wang J (May 2020). "Potential therapeutic targets for intracerebral hemorrhage-associated inflammation: An update". J Cereb Blood Flow Metab. 40 (9): 1752–1768. doi:10.1177/0271678X20923551. PMC 7446569. PMID 32423330. S2CID 218689863.
- Wu H, Zhang Z, Hu X, Zhao R, Song Y, Ban X, Qi J, Wang J (2010). "Dynamic changes of inflammatory markers in brain after hemorrhagic stroke in humans: a postmortem study". Brain Research. 1342 (1342): 111–1117. doi:10.1016/j.brainres.2010.04.033. PMC 2885522. PMID 20420814.
- Lan X, Han X, Li Q, Yang QW, Wang J (2017). "Modulators of microglial activation and polarization after intracerebral haemorrhage". Nat Rev Neurol. 13 (7): 420–433. doi:10.1038/nrneurol.2017.69. PMC 5575938. PMID 28524175.
- Johannes Lindsberg, Perttu; Strbian, Daniel; Karjalainen-Lindsberg, Marja-Liisa (2010). "Mast Cells as Early Responders in the Regulation of Acute Blood–Brain Barrier Changes after Cerebral Ischemia and Hemorrhage". Journal of Cerebral Blood Flow & Metabolism. 30 (4): 689–702. doi:10.1038/jcbfm.2009.282. PMC 2949160. PMID 20087366.
Further reading
- Hemphill JC, 3rd; Greenberg, SM; Anderson, CS; Becker, K; Bendok, BR; Cushman, M; Fung, GL; Goldstein, JN; Macdonald, RL; Mitchell, PH; Scott, PA; Selim, MH; Woo, D (28 May 2015). "Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association". Stroke: A Journal of Cerebral Circulation. 46 (7): 2032–60. doi:10.1161/STR.0000000000000069. PMID 26022637.