Fibrodysplasia ossificans progressiva
Fibrodysplasia ossificans progressiva (/ˌfaɪbroʊdɪˈspleɪʒ(i)ə ɒˈsɪfɪkænz prəˈɡrɛsɪvə/;[1] abbr. FOP; also called Münchmeyer disease and formerly called myositis ossificans progressiva or Stoneman disease) is an extremely rare connective tissue disease in which fibrous connective tissue such as muscle, tendons, and ligaments turn into bone tissue. It is the only known medical condition where one organ system changes into another.[2] It is a severe, disabling disorder with no current cure or treatment.
| Fibrodysplasia ossificans progressiva | |
|---|---|
| Other names | FOP, Stoneman disease, Münchmeyer disease |
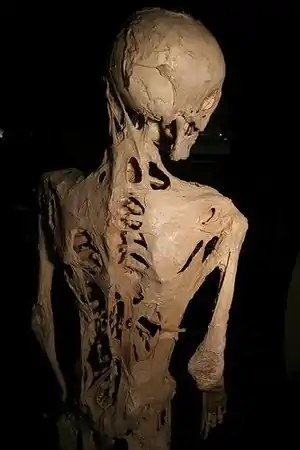 | |
| The effects of fibrodysplasia ossificans progressiva, a disease which causes damaged soft tissue to regrow as bone.(Skeleton of Harry Raymond Eastlack) | |
| Specialty | Medical genetics, rheumatology |
| Symptoms | Continuous bone growth |
| Usual onset | Before age 10 |
| Differential diagnosis | Fibrous dysplasia |
| Treatment | None |
| Prognosis | Median life expectancy ≈ 40 years old (if properly managed) |
| Frequency | 801 confirmed cases worldwide (2017); incidence rate estimated to be 0.5 cases per million people (1 in 2 million) |
FOP is caused by a mutation of the gene ACVR1. The mutation affects the body's repair mechanism, causing fibrous tissue including muscle, tendons, and ligaments to become ossified, either spontaneously or when damaged as the result of trauma. In many cases, otherwise minor injuries can cause joints to become permanently fused as new bone forms, replacing the damaged muscle tissue. This new bone formation (known as "heterotopic ossification") eventually forms a secondary skeleton and progressively restricts the patient's ability to move. Bone formed as a result of this process is identical to "normal" bone, simply in improper locations. Circumstantial evidence suggests that the disease can cause joint degradation separate from its characteristic bone growth.[3]
Surgical removal of the extra bone growth has been shown to cause the body to "repair" the affected area with additional bone. Although the rate of bone growth may differ depending on the patient, the condition ultimately leaves those affected by the condition immobilized as new bone replaces musculature and fuses with the existing skeleton.
Signs and symptoms
For unknown reasons, children born with FOP often have malformed big toes, sometimes missing a joint or, in other cases, simply presenting with a notable lump at the minor joint.[4] The first "flare-up" that leads to the formation of FOP bone usually occurs before the age of 10.[4] The bone growth generally progresses from the top of the body downward, just as bones grow in fetuses. A child with FOP will typically develop additional bones starting at the neck, then at the shoulders, arms, chest area, and finally at the feet.
Specifically, ossification is typically first seen in the dorsal, axial, cranial and proximal regions of the body. Later the disease progresses in the ventral, appendicular, caudal and distal regions.[4] However, it does not necessarily occur in this order due to injury-caused flare-ups. Often, the tumor-like lumps that characterize a flare-up of the disease appear suddenly.
Bone growth occurring during flare-ups may result in the loss of mobility to affected joints, including, if the jaw/mandible is involved, the inability to fully open the mouth, limiting speech and eating. A specific occurrence of a flare-up of this condition in the foot/ankle joints can result in the limited ability to put a foot flat on the ground. Bone growth can also result in the immobilization of the hip or knee, affecting the individual's ability to walk. Extra bone formation around the rib cage restricts the expansion of lungs and diaphragm causing respiratory complications.[4]
Since the disorder is so rare, the condition may be misdiagnosed as cancer or fibrosis. This leads physicians to order biopsies which can exacerbate the growth of FOP bone.[5] The presence of malformed toes or thumbs in those born with FOP help distinguish this disorder from other skeletal problems.[6]
With proper medical management the median age of survival is 40 years. However, delayed diagnosis, trauma, and infections can decrease life expectancy.[7]
Causes
FOP is caused by an autosomal dominant allele on chromosome 2q23-24.[8] The allele has variable expressivity, but complete penetrance. Most cases are caused by spontaneous mutation in the gametes; most people with FOP cannot or choose not to have children. A similar but less catastrophic disease is fibrous dysplasia, which is caused by a post-zygotic mutation.
A mutation in the gene ACVR1 (also known as activin-like kinase 2 (ALK2)) is responsible for the disease.[8] ACVR1 encodes activin receptor type-1, a BMP type-1 receptor. The mutation causes substitution of codon 206 from arginine to histidine in the ACVR1 protein.[9][10] This substitution causes abnormal activation of ACVR1, leading to the transformation of connective tissue and muscle tissue into a secondary skeleton. This causes endothelial cells to transform to mesenchymal stem cells and then to bone.[11] Normally, the ACVR1 gene encodes the activin receptor type-1 transmembrane kinase that bind BMP receptors (Type I BMPR and Type II BMPR) for chondrogenesis signaling. BMPs belong to a superfamily of proteins known as Transforming growth factor-beta (TGF-β) proteins. The binding of ACVR1 protein to BMP receptors start a signaling cascade that is crucial for inducing endochondral bone formation during development, as well as, skeletal and tissue homeostasis.[12]
Genetics

FOP is an autosomal dominant disorder. Thus, a child of an affected heterozygous parent and an unaffected parent has a 50% probability of being affected. Two affected individuals can produce unaffected children. Two unaffected individuals can produce an affected offspring as a result of the mutation of the gene. The homozygous dominant form is more severe than the heterozygous form.[13]
The protein that causes ossification is normally deactivated by an inhibitory protein after a fetus's bones are formed in the womb, but in patients with FOP, the protein keeps working. Aberrant bone formation in patients with FOP occurs when injured connective tissue or muscle cells at the sites of injury or growth incorrectly express an enzyme for bone repair during apoptosis (self-regulated cell death), resulting in lymphocytes containing excess bone morphogenetic protein 4 (BMP4) provided during the immune system response. The bone that results occurs independently of the normal skeleton, forming its own discrete skeletal elements. These elements, however, can fuse with normal skeletal bone.[14] The diaphragm, tongue, and extra-ocular muscles are spared in this process, as well as cardiac and smooth muscle.[4] Since the incorrect enzyme remains unresolved within the immune response, the body continues providing the incorrect BMP4-containing lymphocytes. BMP4 is a product that contributes to the development of the skeleton in the normal embryo.[15]
The ACVR1 gene encodes a bone morphogenic protein (BMP) receptor; this gene is mutated in FOP. It is responsible for growth and development of bone and muscles. The typical mutation, R202H, makes the inhibitor FKBP1A bind less tightly to the activation GS-loop.[16] The result is that ACVR1 is not effectively turned off, and an overgrowth of bone and cartilage and fusion of joints occurs.[17] Atypical mutations involving other residues work similarly. In some cases, the receptor can end up signalling that it's active without being bound to its activating ligand.[18]
Most of the cases of FOP were results of a new gene mutation: these people had no history of this particular disorder in their family. There are some cases where the individual has inherited the mutation from one affected parent.[17]
Diagnosis
Generally, FOP can be diagnosed with radiographs. Early diagnosis of this disorder through radiology is very important to avoid unnecessary invasive investigations like biopsies. The smallest or trivial trauma or intramuscular injections can amplify progression of the disease through inflammation hence the favorability of radiology. Clinicians should be aware of this rare entity, as it is frequently misdiagnosed as cancer or other benign entities such as infection, resulting in biopsies that can often hasten disease progression.[19]
Outbreaks may be measurable clinically by elevated levels of alkaline phosphatase and bone-specific alkaline phosphatase.[20] Another telltale sign of FOP is a shortened great toe with a malformed distal first metatarsal and a missing or abnormal first phalanx and/or interphalangeal joint.[21]
Treatment
There is no cure or approved treatment for FOP.[22] Attempts to surgically remove bone in a FOP patient may result in explosive growth of new bone.[23] While undergoing anesthesia, people with FOP may encounter difficulties with intubation, restrictive pulmonary disease, and changes in the electrical conduction system of the heart.[24] Activities that increase the risk of falling or soft tissue injury should be avoided, as even minor trauma may provoke heterotopic bone formation.[25]
Although there are no effective definitive treatments of the disorder, there are intermittent treatments such as anti-inflammatory drugs to suppress inflammation as a result from flare-ups or inflammation from bone damage. Currently, surgery is not possible for people with FOP as it can incite rapid bone formation at incision sites. Surgical release of joint contractures is generally unsuccessful and risks new, trauma-induced heterotopic ossification.[26]
Epidemiology
As of 2017, approximately 800 cases of FOP have been confirmed worldwide making FOP one of the rarest diseases known.[22] The estimated incidence of FOP is 0.5 cases per million people and affects all ethnicities.[22]
History

Medical reports describing individuals affected by FOP date back to Dr. Guy Patin in 1692.[22] FOP was originally called myositis ossificans progressiva and was thought to be caused by muscular inflammation (myositis) that caused bone formation.[22] The disease was renamed by Victor A. McKusick in 1970 following the discovery that soft tissue other than muscles (e.g. ligaments) were also affected by the disease process.[22]
The best known FOP case is that of Harry Eastlack (1933–1973). His condition began to develop at the age of ten, and by the time of his death from pneumonia in November 1973, six days before his 40th birthday, his body had completely ossified, leaving him able to move only his lips. Eastlack never met another person with FOP during his lifetime.[27]
Eastlack donated his body to science and his skeleton is now at the Mütter Museum in Philadelphia, and has proven to be an invaluable source of information in the study of FOP. Another person with FOP, Carol Orzel (April 20, 1959 – February 2018), also donated her body to the museum and her skeleton was placed on exhibit there, adjacent to Eastlack's, in February 2019.[28][29]
Research

Clinical trials of isotretinoin, etidronate with oral corticosteroids, and perhexiline maleate have failed to demonstrate effectiveness, though the variable course of the disease and small prevalence induces uncertainty.[20]
A handful of pharmaceutical companies focused on rare diseases are currently in varying stages of investigation into different therapeutic approaches for FOP.
In August 2015, the U.S. Food and Drug Administration (FDA) Office of Orphan Products Development granted La Jolla Pharmaceuticals orphan drug designation for two novel compounds for FOP. The compounds are small-molecule protein kinase inhibitors designed to selectively block ACVR1 (ALK2).[35]
In August 2015, Clementia Pharmaceuticals also began the enrollment of children (ages 6 and above) into its Phase II clinical trial investigating palovarotene for the treatment of FOP.[36] Preclinical studies demonstrated that palovarotene, a retinoic acid receptor gamma agonist, blocked abnormal bone formation in animal models by inhibition of secondary messenger systems in the BMP pathway.[37] Clementia licensed palovarotene from Roche Pharmaceuticals, which previously evaluated the compound in more than 800 individuals including healthy volunteers and patients with chronic obstructive pulmonary disease. Palovarotene received Fast Track designation from the FDA and orphan designations for the treatment of FOP from both the FDA and the European Medicines Agency (EMA).[36]
In September 2015, Regeneron announced new insight into the mechanism of disease involving the activation of the ACVR1 receptor by activin A. In 2016, the company initiated a phase 1 study of its activin antibody, REGN 2477, in healthy volunteers; a phase 2 trial in FOP patients was conducted in 2017.[38]
Another potential therapeutic approach involves allele-specific RNA interference that targets mutated mRNA for degradation while preserving normal ACVR1 gene expression.[39]
Further investigation into the mechanisms of heterotopic bone formation in FOP could aid in the development of treatments for other disorders involving extra-skeletal bone formation.
Fibro/adipogenic progenitors (FAPs) may be the disease-causing cell type responsible for activin A dependent ectopic bone formation in both the muscles and tendons of mice bearing the FOP causing ACVR1(R206H) mutation.[40]
Clinical trials of several potential treatments are in progress as of 2019.[41]
Recently, as of 2021, a potential therapeutic candidate, saracatinib, is in phase III clinical trials as a potent heterotopic ossification inhibitor in wild-type and ACVR1 mutant mice.[42]
See also
- International FOP Association
- Osteogenesis imperfecta, a condition characterized by bones breaking unusually easily, caused by mutations in genes related to those responsible for FOP
- Progressive osseous heteroplasia
- FOP Friends
References
- "Medical Definition of fibrodysplasia ossificans progressiva". www.merriam-webster.com. Retrieved 8 May 2022.
- Kaplan, Frederick S.; Shen, Qi; Lounev, Vitali; Seemann, Petra; Groppe, Jay; Katagiri, Takenobu; Pignolo, Robert J.; Shore, Eileen M. (2008). "Skeletal metamorphosis in fibrodysplasia ossificans progressiva (FOP)". Journal of Bone and Mineral Metabolism. 26 (6): 521–530. doi:10.1007/s00774-008-0879-8. PMC 3620015. PMID 18979151.
- Pinkowski, Jen (1 March 2019). "Here's what happens when your body tissues turn to bone". National Geographic. Archived from the original on 3 March 2019.
- Kaplan, Frederick S.; Le Merrer, Martine; Glaser, David L.; Pignolo, Robert J.; Goldsby, Robert E.; Kitterman, Joseph A.; Groppe, Jay; Shore, Eileen M. (March 2008). "Fibrodysplasia ossificans progressiva". Best Practice & Research Clinical Rheumatology. 22 (1): 191–205. doi:10.1016/j.berh.2007.11.007. PMC 2424023. PMID 18328989.
- Obamuyide, HA; Ogunlade, SO (March 2015). "A Tumour for which Surgery will do more harm than good: A Case Report of Fibrodysplasia Ossificans Progressiva". The Nigerian Postgraduate Medical Journal. 22 (1): 83–8. PMID 25875418. ProQuest 1850178336.
- "Fibrodysplasia ossificans progressiva". Lister Hill National Center for Biomedical Communications. Retrieved 12 December 2013.
- Saleh, Mohammed; Commandeur, Joost; Bocciardi, Renata; Kinabo, Grace; Hamel, Ben (2015). "Fibrodysplasia ossificans progressiva with minor unilateral hallux anomaly in a sporadic case from Northern Tanzania with the common ACVR1c.617G>A mutation". Pan African Medical Journal. 22: 299. doi:10.11604/pamj.2015.22.299.8032. PMC 4769042. PMID 26966495.
- Shore, Eileen M; Xu, Meiqi; Feldman, George J; Fenstermacher, David A; Cho, Tae-Joon; Choi, In Ho; Connor, J Michael; Delai, Patricia; Glaser, David L; LeMerrer, Martine; Morhart, Rolf; Rogers, John G; Smith, Roger; Triffitt, James T; Urtizberea, J Andoni; Zasloff, Michael; Brown, Matthew A; Kaplan, Frederick S (May 2006). "A recurrent mutation in the BMP type I receptor ACVR1 causes inherited and sporadic fibrodysplasia ossificans progressiva". Nature Genetics. 38 (5): 525–527. doi:10.1038/ng1783. PMID 16642017. S2CID 41579747.
- "Penn Researchers Discover Gene That Creates Second Skeleton" (Press release). University of Pennsylvania School of Medicine. 23 April 2006.
- Hatsell, Sarah J.; Idone, Vincent; Wolken, Dana M. Alessi; Huang, Lily; Kim, Hyon J.; Wang, Lili; Wen, Xialing; Nannuru, Kalyan C.; Jimenez, Johanna; Xie, Liqin; Das, Nanditha; Makhoul, Genevieve; Chernomorsky, Rostislav; D’Ambrosio, David; Corpina, Richard A.; Schoenherr, Christopher J.; Feeley, Kieran; Yu, Paul B.; Yancopoulos, George D.; Murphy, Andrew J.; Economides, Aris N. (2 September 2015). "ACVR1 R206H receptor mutation causes fibrodysplasia ossificans progressiva by imparting responsiveness to activin A". Science Translational Medicine. 7 (303): 303ra137. doi:10.1126/scitranslmed.aac4358. PMC 6164166. PMID 26333933.
- van Dinther, Maarten; Visser, Nils; de Gorter, David JJ; Doorn, Joyce; Goumans, Marie-José; de Boer, Jan; ten Dijke, Peter (23 November 2009). "ALK2 R206H Mutation Linked to Fibrodysplasia Ossificans Progressiva Confers Constitutive Activity to the BMP Type I Receptor and Sensitizes Mesenchymal Cells to BMP-Induced Osteoblast Differentiation and Bone Formation". Journal of Bone and Mineral Research. 25 (6): 091211115834058–35. doi:10.1359/jbmr.091110. PMID 19929436. S2CID 207269687.
- Lin, Shuxian; Svoboda, Kathy K. H.; Feng, Jian Q.; Jiang, Xinquan (5 April 2016). "The biological function of type I receptors of bone morphogenetic protein in bone". Bone Research. 4 (1): 16005. doi:10.1038/boneres.2016.5. ISSN 2095-6231. PMC 4820739. PMID 27088043.
- Cummings, Michael R. Human Heredity: Principles and Issues Cengage Learning, 2011, [2009]. p. 77
- Shore, Eileen M.; Kaplan, Frederick S. (2008). "Insights from a Rare Genetic Disorder of Extra-Skeletal Bone Formation, Fibrodysplasia Ossificans Progressiva (FOP)". Bone. 43 (3): 427–443. doi:10.1016/j.bone.2008.05.013. PMC 2601573. PMID 18590993.
- Kierszenbaum, Abraham (2002). Histology and cell biology. New York: Mosby. ISBN 978-0-323-01639-1.
- "AVCR1", Genetics Home Reference, U.S. National Library of Medicine, August 2007. Accessed February 18, 2014.
- "Fibrodysplasia ossificans progressiva", Genetics Home Reference, U.S. National Library of Medicine, August 2007. Accessed February 18, 2014.
- Petrie, KA; Lee, WH; Bullock, AN; Pointon, JJ; Smith, R; Russell, RG; Brown, MA; Wordsworth, BP; Triffitt, JT (2009). "Novel mutations in ACVR1 result in atypical features in two fibrodysplasia ossificans progressiva patients". PLOS ONE. 4 (3): e5005. Bibcode:2009PLoSO...4.5005P. doi:10.1371/journal.pone.0005005. PMC 2658887. PMID 19330033.
- Yamin, Ghiam; Daghighi, Shadi; Mafee, Mahmood (31 May 2021). "Fibrodysplasia ossificans progressiva (FOP) presenting as a rapidly growing non-calcified neck mass". Journal of Radiology Case Reports. 15 (5): 10–16. doi:10.3941/jrcr.v15i5.4103. ISSN 1943-0922. PMC 8253151. PMID 34276874.
- Kitoh, Hiroshi; Achiwa, Masataka; Kaneko, Hiroshi; Mishima, Kenichi; Matsushita, Masaki; Kadono, Izumi; Horowitz, John D; Sallustio, Benedetta C; Ohno, Kinji; Ishiguro, Naoki (2013). "Perhexiline maleate in the treatment of fibrodysplasia ossificans progressiva: an open-labeled clinical trial". Orphanet Journal of Rare Diseases. 8 (1): 163. doi:10.1186/1750-1172-8-163. PMC 4015865. PMID 24131551.
- "Fibrodysplasia Ossificans Progressiva". August 2020.
- Martelli, Anderson; Santos, Arnaldo Rodrigues (3 July 2014). "Cellular and morphological aspects of fibrodysplasia ossificans progressiva: Lessons of formation, repair, and bone bioengineering". Organogenesis. 10 (3): 303–311. doi:10.4161/org.29206. PMC 4750545. PMID 25482313.
- American Academy of Orthopaedic Surgeons (May 2006). "Fibrodysplasia Ossificans Progressiva (FOP)". orthoinfo.aaos.org. Archived from the original on 21 June 2012. Retrieved 7 October 2011.
- Newton, M.C.; Allen, P.W.; Ryan, D.C. (February 1990). "Fibrodysplasia Ossificans Progressiva". British Journal of Anaesthesia. 64 (2): 246–250. doi:10.1093/bja/64.2.246. PMID 2317429.
- "The Medical Management of Fibrodysplasia Ossificans Progressiva: Current Treatment Considerations" (PDF). International Fibrodysplasia Ossificans Progressiva Association. January 2020.
- Kaplan, Frederick S.; Le Merrer, Martine; Glaser, David L.; Pignolo, Robert J.; Goldsby, Robert; Kitterman, Joseph A.; Groppe, Jay; Shore, Eileen M. (March 2008). "Fibrodysplasia ossificans progressiva". Best Practice & Research. Clinical Rheumatology. 22 (1): 191–205. doi:10.1016/j.berh.2007.11.007. ISSN 1521-6942. PMC 2424023. PMID 18328989.
- Kaplan, F. S. (2013). The skeleton in the closet. Gene, 528(1), 7–11. https://doi.org/10.1016/j.gene.2013.06.022
- McCullough, Marie (28 February 2019). "New Mutter Museum exhibit grants final wish for woman who turned to bone". The Philadelphia Inquirer. Retrieved 28 February 2019.
- "Mütter Museum Reveals New Exhibit: Philadelphia Woman's Skeleton With Rare Bone Disease". Mütter Museum. 5 March 2019. Archived from the original on 28 August 2021. Retrieved 7 March 2020.
- "Dr. Frederick Kaplan, M.D. 2017 Rare Impact Award Honoree". National Organization for Rare Disorders. 15 March 2017. Retrieved 8 May 2022.
- "Frederick Kaplan: Rare Impact Award" (PDF). Almanac. University of Pennsylvania. 63 (32): 7. 25 April 2017. Retrieved 8 May 2022.
- "An FOP Timeline". Penn Medicine. University of Pennsylvania. Retrieved 8 May 2022.
- "AP: Scientists solve rare bone disease mystery". NBC News. 24 April 2006. Retrieved 8 May 2022.
- Maeder, Thomas (1 February 1998). "A Few Hundred People Turned To Bone". The Atlantic. Retrieved 8 May 2022.
- "La Jolla Pharmaceutical Company Receives Orphan Drug Designation for Two Novel Compounds for Fibrodysplasia Ossificans Progressiva" (Press release). La Jolla Pharmaceutical Company. 18 August 2015.
- "Clementia Pharmaceuticals Expands Ongoing Phase 2 Study to Include Children with Fibrodysplasia Ossificans Progressiva (FOP)" (Press release). Clementia Pharmaceuticals. 25 August 2015.
- "Pipeline". www.clementiapharma.com. Archived from the original on 29 September 2015. Retrieved 22 November 2015.
- "Regeneron Shares Updates on its Ongoing FOP Research Program". International Fibrodysplasia Ossificans Progressiva Association. 9 March 2017.
- J. W. Lowery; V. Rosen (2012). "Allele-Specific RNA Interference in FOP Silencing the FOP gene". Gene Therapy. 19 (7): 701–702. doi:10.1038/gt.2011.190. PMID 22130446. S2CID 24990800.
- Lees-Shepard, John B.; Yamamoto, Masakazu; Biswas, Arpita A.; Stoessel, Sean J.; Nicholas, Sarah-Anne E.; Cogswell, Cathy A.; Devarakonda, Parvathi M.; Schneider, Michael J.; Cummins, Samantha M.; Legendre, Nicholas P.; Yamamoto, Shoko; Kaartinen, Vesa; Hunter, Jeffrey W.; Goldhamer, David J. (December 2018). "Activin-dependent signaling in fibro/adipogenic progenitors causes fibrodysplasia ossificans progressiva". Nature Communications. 9 (1): 471. Bibcode:2018NatCo...9..471L. doi:10.1038/s41467-018-02872-2. PMC 5797136. PMID 29396429.
- McCullough, Marie (28 February 2019). "Therapies in sight for FOP, a disease that turns muscle to bone". The Philadelphia Inquirer.
- Williams, Eleanor; Bagarova, Jana; Kerr, Georgina; Xia, Dong-Dong; Place, Elsie S.; Dey, Devaveena; Shen, Yue; Bocobo, Geoffrey A.; Mohedas, Agustin H.; Huang, Xiuli; Sanderson, Philip E. (2021). "Saracatinib is an efficacious clinical candidate for fibrodysplasia ossificans progressiva". JCI Insight. 6 (8): e95042. doi:10.1172/jci.insight.95042. ISSN 2379-3708. PMC 8119212. PMID 33705358.
Further reading
- Cohen, M. Michael; Howell, Robin E. (October 1999). "Etiology of fibrous dysplasia and McCune-Albright syndrome". International Journal of Oral and Maxillofacial Surgery. 28 (5): 366–371. doi:10.1016/s0901-5027(99)80085-x. PMID 10535539.