Post-exertional malaise
Post-exertional malaise (PEM) is a worsening of chronic fatigue syndrome symptoms that occurs after exertion. PEM involves increased fatigue, and an exacerbation of other symptoms. PEM is often severe enough to be disabling, and is triggered by ordinary activities that healthy people tolerate. Post-exertional malaise typically begins 12–48 hours after the activity that triggers it, and lasts for days, but this is highly variable.[1][2][3] Management of PEM is symptomatic, and patients are recommended to pace their activities to avoid triggering PEM.
| Post-exertional malaise | |
|---|---|
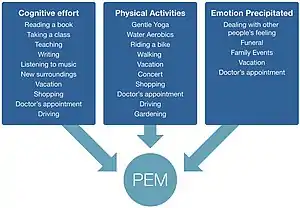 | |
| Chart of physical, cognitive, and emotional activities that may trigger PEM | |
| Symptoms | Worsening of symptoms after ordinary activity |
| Causes | Chronic fatigue syndrome Long Covid |
| Treatment | Symptomatic |
Description
Post-exertional malaise involves fatigue, and is of such a severity that it impacts a person's functioning.[3] Other symptoms that may be experienced during PEM include cognitive impairment, flu-like symptoms, pain, weakness or trouble sleeping.[3][1] While typically cast as a worsening of existing symptoms, patients may experience some symptoms exclusively during PEM.[3] Patients often describe PEM as "crash," "relapse," or "setback."[3]
PEM is triggered by "minimal"[2] physical or mental activities that were previously tolerated, and that healthy people tolerate, like attending a social event, grocery shopping, or even taking a shower.[1] Emotional distress, injury, sleep deprivation, infections, and spending too long standing or sitting up are also cited as potential triggers.[3] The resulting symptoms are disproportionate to the triggering activity and distinct from typical fatigue.[3][4] PEM is often debilitating,[5] and may render someone housebound or bedbound until they recover.[1] The course of a crash is highly variable. The onset of symptoms typically occurs 12–48 hours after the triggering activity,[2] but may be immediate, or delayed up to 7 days.[3] PEM lasts "usually a day or longer,"[5] but can span hours, days, weeks, or months.[3] The level of activity that triggers PEM, as well as the symptoms, vary from person to person, and within individuals over time.[3] Due to this variability, people with CFS may be unable to predict what will trigger PEM.[1]
Diagnosis
PEM is a common symptom of ME/CFS, occurring in 60 to 100% of patients, depending on how the condition is defined.[3] PEM is also a common symptom of long COVID, where long COVID symptoms may get worse after exertion, in a similar manner as ME/CFS.[6]
PEM is considered a cardinal symptom by a number of the different diagnostic criteria for ME/CFS: the International Consensus Criteria,[1][5][7] the National Academy of Medicine criteria,[8][9] and NICE's definition of CFS[4] all require it. The Canadian Consensus Criteria require "post exertional malaise and/or [post exertional] fatigue" instead.[10][11][12][8][13] On the other hand, the older Oxford Criteria lack any mention of PEM,[14] and the Fukuda Criteria consider it optional. A 2-day Cardiopulmonary Exercise Test (CPET) has emerged as a helpful tool in documenting PEM, showing apparent abnormalities in the way the body responds to exercise.[15] Still, there needs to be more attention and urgency placed on firmly establishing a diagnostic test.
Management
There is no treatment or cure for ME/CFS or PEM. Pacing, a management strategy in which someone plans their activities to stay within their limits, may help people avoid triggering PEM.[16]
References
- "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Symptoms". Centers for Disease Control and Prevention. U.S. Department of Health & Human Services. 14 July 2017. Retrieved 23 September 2017.
- "Terms: Post-exertional malaise". Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management - Recommendations. NICE (Report). 29 October 2021. NICE guideline NG206.
- "Beyond Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Redefining an Illness" (PDF). National Academy of Medicine. 2015. pp. 78–86. Retrieved 12 May 2022.
- "1.2 Suspecting ME/CFS". Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management - Recommendations. NICE (Report). 29 October 2021. NICE guideline NG206.
- Carruthers, B. M.; van de Sande, M. I.; De Meirleir, K. L.; Klimas, N. G.; Broderick, G.; Mitchell, T.; Staines, D.; Powles, A. C. P.; Speight, N.; Vallings, R.; Bateman, L.; Baumgarten-Austrheim, B.; Bell, D. S.; Carlo-Stella, N.; Chia, J.; Darragh, A.; Jo, D.; Lewis, D.; Light, A. R.; Marshall-Gradisbik, S.; Mena, I.; Mikovits, J. A.; Miwa, K.; Murovska, M.; Pall, M. L.; Stevens, S. (October 2011). "Myalgic encephalomyelitis: International Consensus Criteria". Journal of Internal Medicine. 270 (4): 327–338. doi:10.1111/j.1365-2796.2011.02428.x. PMC 3427890. PMID 21777306.
- "Long COVID or Post-COVID Conditions". Centers for Disease Control and Prevention. 1 September 2022.
- Maes, Michael; Anderson, George; Morris, Gerwyn; Berk, Michael (27 February 2013). "Diagnosis of myalgic encephalomyelitis: where are we now?". Expert Opinion on Medical Diagnostics. 7 (3): 221–225. doi:10.1517/17530059.2013.776039. PMID 23480562.
- "IOM 2015 Diagnostic Criteria | Diagnosis | Healthcare Providers | Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) | CDC". www.cdc.gov. 2018-11-08. Retrieved 2019-03-08.
- "Symptoms of ME/CFS | Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)". CDC. 2021-01-27.
- Myhill, Sarah; Booth, Norman E; McLaren-Howard, John (2009). "Chronic fatigue syndrome and mitochondrial dysfunction" (PDF). Int J Clin Exp Med. 2 (1): 1–16. PMC 2680051. PMID 19436827.
- Carruthers, Bruce M; van de Sande, Marjorie I. (2005). "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Clinical Case Definition and Guidelines for Medical Practitioners" (PDF). sacfs.asn.au. p. 8.
There is an inappropriate loss of physical and mental stamina, rapid muscular and cognitive fatigability, post exertional malaise and/or fatigue and/or pain and a tendency for other associated symptoms within the patient's cluster of symptoms to worsen.
- "Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Key Facts" (PDF). nap.edu. 2015. p. 2.
- Wright Clayton, Ellen; Alegria, Margarita; Bateman, Lucinda; Chu, Lily; Cleeland, Charles; Davis, Ronald; Diamond, Betty; Ganlats, Theodore; Keller, Betsy (2015). "Beyond Myalgic Encephalomyelits/Chronic Fatigue Syndrome: Redefining an Illness (Report Guide for Clinicians)" (PDF). nationalacademies.org. Nancy Klimas, A. Martin Lerner, Cynthia Mulrow, Benjamin Natelson, Peter Rowe, Michael Shelanski. National Academy of Medicine (Institutes of Medicine). p. 7.
- Sharpe, Michael (February 1991). "A report--chronic fatigue syndrome: guidelines for research". Journal of the Royal Society of Medicine. 84 (2): 118–121. doi:10.1177/014107689108400224. PMC 1293107. PMID 1999813.
- Eun-Jin, Lim; Eun-Bum, Kang; Eun-Su, Jang; Chang-Gue, Son. "The Prospects of the Two-Day Cardiopulmonary Exercise Test (CPET) in ME/CFS Patients: A Meta-Analysis". National Library of Medicine. J Clin Med. Retrieved 3 October 2022.
- "1.11 Managing ME/CFS". Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management - Recommendations. NICE (Report). 29 October 2021. NICE guideline NG206.