Acute disseminated encephalomyelitis
Acute disseminated encephalomyelitis (ADEM), or acute demyelinating encephalomyelitis, is a rare autoimmune disease marked by a sudden, widespread attack of inflammation in the brain and spinal cord. As well as causing the brain and spinal cord to become inflamed, ADEM also attacks the nerves of the central nervous system and damages their myelin insulation, which, as a result, destroys the white matter. It is often triggered by a viral infection or (very rarely) vaccinations.[1][2][3][4][5][6]
| Acute disseminated encephalomyelitis | |
|---|---|
| Other names | Acute demyelinating encephalomyelitis |
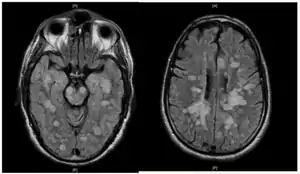 | |
| Fulminating ADEM showing many lesions. The patient survived, but remained in a persistent vegetative state | |
| Specialty | Neurology |
ADEM's symptoms resemble the symptoms of multiple sclerosis (MS), so the disease itself is sorted into the classification of the multiple sclerosis borderline diseases. However, ADEM has several features that distinguish it from MS.[7] Unlike MS, ADEM occurs usually in children and is marked with rapid fever, although adolescents and adults can get the disease too. ADEM consists of a single flare-up whereas MS is marked with several flare-ups (or relapses), over a long period of time. Relapses following ADEM are reported in up to a quarter of patients, but the majority of these 'multiphasic' presentations following ADEM likely represent MS.[8] ADEM is also distinguished by a loss of consciousness, coma and death, which is very rare in MS, except in severe cases.
It affects about 8 per 1,000,000 people per year.[9] Although it occurs in all ages, most reported cases are in children and adolescents, with the average age around 5 to 8 years old.[10][11][12][13] The disease affects males and females almost equally.[14] ADEM shows seasonal variation with higher incidence in winter and spring months which may coincide with higher viral infections during these months.[13] The mortality rate may be as high as 5%; however, full recovery is seen in 50 to 75% of cases with increase in survival rates up to 70 to 90% with figures including minor residual disability as well.[15] The average time to recover from ADEM flare-ups is one to six months.
ADEM produces multiple inflammatory lesions in the brain and spinal cord, particularly in the white matter. Usually these are found in the subcortical and central white matter and cortical gray-white junction of both cerebral hemispheres, cerebellum, brainstem, and spinal cord,[16] but periventricular white matter and gray matter of the cortex, thalami and basal ganglia may also be involved.
When a person has more than one demyelinating episode of ADEM, the disease is then called recurrent disseminated encephalomyelitis[17] or multiphasic disseminated encephalomyelitis[18] (MDEM). Also, a fulminant course in adults has been described.[19]
Signs and symptoms
ADEM has an abrupt onset and a monophasic course. Symptoms usually begin 1–3 weeks after infection. Major symptoms include fever, headache, nausea and vomiting, confusion, vision impairment, drowsiness, seizures and coma. Although initially the symptoms are usually mild, they worsen rapidly over the course of hours to days, with the average time to maximum severity being about four and a half days.[20] Additional symptoms include hemiparesis, paraparesis, and cranial nerve palsies.[21]
ADEM in COVID-19
Neurological symptoms were the main presentation of COVID-19, which did not correlate with the severity of respiratory symptoms. The high incidence of ADEM with hemorrhage is striking. Brain inflammation is likely caused by an immune response to the disease rather than neurotropism. CSF analysis was not indicative of an infectious process, neurological impairment was not present in the acute phase of the infection, and neuroimaging findings were not typical of classical toxic and metabolic disorders. The finding of bilateral periventricular relatively asymmetrical lesions allied with deep white matter involvement, that may also be present in cortical gray-white matter junction, thalami, basal ganglia, cerebellum, and brainstem suggests an acute demyelination process.[22] Additionally, hemorrhagic white matter lesions, clusters of macrophages related to axonal injury and ADEM-like appearance were also found in subcortical white matter.[23]
Causes
Since the discovery of the anti-MOG specificity against multiple sclerosis diagnosis[24] it is considered that ADEM is one of the possible clinical causes of anti-MOG associated encephalomyelitis.[25]
About how the anti-MOG antibodies appear in the patients serum there are several theories:
- A preceding antigenic challenge can be identified in approximately two-thirds of people.[14] Some viral infections thought to induce ADEM include influenza virus, dengue,[26] enterovirus, measles,[27] mumps, rubella, varicella zoster, Epstein–Barr virus, cytomegalovirus, herpes simplex virus, hepatitis A, coxsackievirus and COVID-19.[22][28] Bacterial infections include Mycoplasma pneumoniae, Borrelia burgdorferi, Leptospira, and beta-hemolytic Streptococci.[29]
- Exposure to vaccines: The only vaccine proven related to ADEM is the Semple form of the rabies vaccine, but hepatitis B, pertussis, diphtheria, measles, mumps, rubella, pneumococcus, varicella, influenza, Japanese encephalitis, and polio vaccines have all been implicated. The majority of the studies that correlate vaccination with ADEM onset use small samples or case studies. Large scale epidemiological studies (e.g., of MMR vaccine or smallpox vaccine) do not show increased risk of ADEM following vaccination.[9][30][31][32][20][33][34][35][36][37][38] An upper bound for the risk of ADEM from measles vaccination, if it exists, can be estimated to be 10 per million,[39] which is far lower than the risk of developing ADEM from an actual measles infection, which is about 1 per 1,000 cases. For a rubella infection, the risk is 1 per 5,000 cases.[33][40] Some early vaccines, later shown to have been contaminated with host animal CNS tissue, had ADEM incident rates as high as 1 in 600.[30]
- In rare cases, ADEM seems to follow from organ transplantation.[20]
Diagnosis
ADEM term has been inconsistently used at different times.[41] Currently, the commonly accepted international standard for the clinical case definition is the one published by the International Pediatric MS Study Group, revision 2007.[42]
Given that the definition is clinical, it is currently unknown if all the cases with ADEM are positive for anti-MOG autoantibody, but in any case, it seems strongly related to ADEM diagnosis.[25]
Multiple sclerosis
While ADEM and MS both involve autoimmune demyelination, they differ in many clinical, genetic, imaging, and histopathological aspects.[14][43] Some authors consider MS and its borderline forms to constitute a spectrum, differing only in chronicity, severity, and clinical course,[44][45] while others consider them discretely different diseases.[6]
Typically, ADEM appears in children following an antigenic challenge and remains monophasic. Nevertheless, ADEM does occur in adults,[8][12] and can also be clinically multiphasic.[46]
Problems for differential diagnosis increase due to the lack of agreement for a definition of multiple sclerosis.[47] If MS were defined just by the separation in time and space of the demyelinating lesions as McDonald did,[48] it would not be enough to make a difference, as some cases of ADEM satisfy these conditions. Therefore, some authors propose to establish the separation line in the shape of the lesions around the veins, being therefore "perivenous vs. confluent demyelination".[47][49]
.png.webp)
The pathology of ADEM is very similar to that of MS with some differences. The pathological hallmark of ADEM is perivenular inflammation with limited "sleeves of demyelination".[50][14] Nevertheless, MS-like plaques (confluent demyelination) can appear[51]
Plaques in the white matter in MS are sharply delineated, while the glial scar in ADEM is smooth. Axons are better preserved in ADEM lesions. Inflammation in ADEM is widely disseminated and ill-defined, and finally, lesions are strictly perivenous, while in MS they are disposed around veins, but not so sharply.[52]
Nevertheless, the co-occurrence of perivenous and confluent demyelination in some individuals suggests pathogenic overlap between acute disseminated encephalomyelitis and multiple sclerosis and misclassification even with biopsy[49] or even postmortem[51] ADEM in adults can progress to MS[12]
Multiphasic disseminated encephalomyelitis
When the person has more than one demyelinating episode of ADEM, the disease is then called recurrent disseminated encephalomyelitis or multiphasic disseminated encephalomyelitis[18] (MDEM).
It has been found that anti-MOG auto-antibodies are related to this kind of ADEM[53]
Another variant of ADEM in adults has been described, also related to anti-MOG auto-antibodies, has been named fulminant disseminated encephalomyelitis, and it has been reported to be clinically ADEM, but showing MS-like lesions on autopsy.[19] It has been classified inside the anti-MOG associated inflammatory demyelinating diseases.[54]
Acute hemorrhagic leukoencephalitis
Acute hemorrhagic leukoencephalitis (AHL, or AHLE), acute hemorrhagic encephalomyelitis (AHEM), acute necrotizing hemorrhagic leukoencephalitis (ANHLE), Weston-Hurst syndrome, or Hurst's disease, is a hyperacute and frequently fatal form of ADEM. AHL is relatively rare (less than 100 cases have been reported in the medical literature as of 2006),[55] it is seen in about 2% of ADEM cases,[20] and is characterized by necrotizing vasculitis of venules and hemorrhage, and edema.[56] Death is common in the first week[57] and overall mortality is about 70%,[55] but increasing evidence points to favorable outcomes after aggressive treatment with corticosteroids, immunoglobulins, cyclophosphamide, and plasma exchange.[29] About 70% of survivors show residual neurological deficits,[56] but some survivors have shown surprisingly little deficit considering the magnitude of the white matter affected.[57]
This disease has been occasionally associated with ulcerative colitis and Crohn's disease, malaria,[58] sepsis associated with immune complex deposition, methanol poisoning, and other underlying conditions. Also anecdotal association with MS has been reported[59]
Laboratory studies that support diagnosis of AHL are: peripheral leukocytosis, cerebrospinal fluid (CSF) pleocytosis associated with normal glucose and increased protein. On magnetic resonance imaging (MRI), lesions of AHL typically show extensive T2-weighted and fluid-attenuated inversion recovery (FLAIR) white matter hyperintensities with areas of hemorrhages, significant edema, and mass effect.[60]
Treatment
No controlled clinical trials have been conducted on ADEM treatment, but aggressive treatment aimed at rapidly reducing inflammation of the CNS is standard. The widely accepted first-line treatment is high doses of intravenous corticosteroids,[61] such as methylprednisolone or dexamethasone, followed by 3–6 weeks of gradually lower oral doses of prednisolone. Patients treated with methylprednisolone have shown better outcomes than those treated with dexamethasone.[20] Oral tapers of less than three weeks duration show a higher chance of relapsing,[11][18] and tend to show poorer outcomes. Other anti-inflammatory and immunosuppressive therapies have been reported to show beneficial effect, such as plasmapheresis, high doses of intravenous immunoglobulin (IVIg),[61][62] mitoxantrone and cyclophosphamide. These are considered alternative therapies, used when corticosteroids cannot be used or fail to show an effect.
There is some evidence to suggest that patients may respond to a combination of methylprednisolone and immunoglobulins if they fail to respond to either separately[63] In a study of 16 children with ADEM, 10 recovered completely after high-dose methylprednisolone, one severe case that failed to respond to steroids recovered completely after IV Ig; the five most severe cases – with ADAM and severe peripheral neuropathy – were treated with combined high-dose methylprednisolone and immunoglobulin, two remained paraplegic, one had motor and cognitive handicaps, and two recovered.[61] A recent review of IVIg treatment of ADEM (of which the previous study formed the bulk of the cases) found that 70% of children showed complete recovery after treatment with IVIg, or IVIg plus corticosteroids.[64] A study of IVIg treatment in adults with ADEM showed that IVIg seems more effective in treating sensory and motor disturbances, while steroids seem more effective in treating impairments of cognition, consciousness and rigor.[62] This same study found one subject, a 71-year-old man who had not responded to steroids, that responded to an IVIg treatment 58 days after disease onset.
Prognosis
Full recovery is seen in 50 to 70% of cases, ranging to 70 to 90% recovery with some minor residual disability (typically assessed using measures such as mRS or EDSS), average time to recover is one to six months.[15] The mortality rate may be as high as 5–10%.[15][65] Poorer outcomes are associated with unresponsiveness to steroid therapy, unusually severe neurological symptoms, or sudden onset. Children tend to have more favorable outcomes than adults, and cases presenting without fevers tend to have poorer outcomes. The latter effect may be due to either protective effects of fever, or that diagnosis and treatment is sought more rapidly when fever is present. [66]
ADEM can progress to MS. It will be considered MS if some lesions appear in different times and brain areas[67]
Motor deficits
Residual motor deficits are estimated to remain in about 8 to 30% of cases, the range in severity from mild clumsiness to ataxia and hemiparesis.[29]
Neurocognitive
Patients with demyelinating illnesses, such as MS, have shown cognitive deficits even when there is minimal physical disability.[68] Research suggests that similar effects are seen after ADEM, but that the deficits are less severe than those seen in MS. A study of six children with ADEM (mean age at presentation 7.7 years) were tested for a range of neurocognitive tests after an average of 3.5 years of recovery.[69] All six children performed in the normal range on most tests, including verbal IQ and performance IQ, but performed at least one standard deviation below age norms in at least one cognitive domain, such as complex attention (one child), short-term memory (one child) and internalizing behaviour/affect (two children). Group means for each cognitive domain were all within one standard deviation of age norms, demonstrating that, as a group, they were normal. These deficits were less severe than those seen in similar aged children with a diagnosis of MS.[70]
Another study compared nineteen children with a history of ADEM, of which 10 were five years of age or younger at the time (average age 3.8 years old, tested an average of 3.9 years later) and nine were older (mean age 7.7y at time of ADEM, tested an average of 2.2 years later) to nineteen matched controls.[71] Scores on IQ tests and educational achievement were lower for the young onset ADEM group (average IQ 90) compared to the late onset (average IQ 100) and control groups (average IQ 106), while the late onset ADEM children scored lower on verbal processing speed. Again, all groups means were within one standard deviation of the controls, meaning that while effects were statistically reliable, the children were as a whole, still within the normal range. There were also more behavioural problems in the early onset group, although there is some suggestion that this may be due, at least in part, to the stress of hospitalization at a young age.[72][73]
Research
The relationship between ADEM and anti-MOG associated encephalomyelitis is currently under research. A new entity called MOGDEM has been proposed.[74]
About animal models, the main animal model for MS, experimental autoimmune encephalomyelitis (EAE) is also an animal model for ADEM.[75] Being an acute monophasic illness, EAE is far more similar to ADEM than MS.[76]
See also
- Optic neuritis
- Transverse myelitis
- Victoria Arlen
References
- Dale RC (April 2003). "Acute disseminated encephalomyelitis". Seminars in Pediatric Infectious Diseases. 14 (2): 90–95. doi:10.1053/spid.2003.127225. PMID 12881796.
- Garg RK (January 2003). "Acute disseminated encephalomyelitis". Postgraduate Medical Journal. 79 (927): 11–17. doi:10.1136/pmj.79.927.11. PMC 1742586. PMID 12566545.
- Jones CT (November 2003). "Childhood autoimmune neurologic diseases of the central nervous system". Neurologic Clinics. 21 (4): 745–64. doi:10.1016/S0733-8619(03)00007-0. PMID 14743647.
- Huynh W, Cordato DJ, Kehdi E, Masters LT, Dedousis C (December 2008). "Post-vaccination encephalomyelitis: literature review and illustrative case". Journal of Clinical Neuroscience. 15 (12): 1315–22. doi:10.1016/j.jocn.2008.05.002. PMC 7125578. PMID 18976924.
- Rust RS (June 2000). "Multiple sclerosis, acute disseminated encephalomyelitis, and related conditions". Seminars in Pediatric Neurology. 7 (2): 66–90. doi:10.1053/pb.2000.6693. PMID 10914409.
- Poser CM, Brinar VV (October 2007). "Disseminated encephalomyelitis and multiple sclerosis: two different diseases – a critical review". Acta Neurologica Scandinavica. 116 (4): 201–06. doi:10.1111/j.1600-0404.2007.00902.x. PMID 17824894. S2CID 44411472.
- Krupp LB, Banwell B, Tenembaum S (April 2007). "Consensus definitions proposed for pediatric multiple sclerosis and related disorders" (PDF). Neurology. 68 (16 Suppl 2): S7–12. doi:10.1212/01.wnl.0000259422.44235.a8. PMID 17438241. S2CID 26001350. Archived from the original (PDF) on 9 February 2015.
- Koelman DL, Chahin S, Mar SS, Venkatesan A, Hoganson GM, Yeshokumar AK, et al. (May 2016). "Acute disseminated encephalomyelitis in 228 patients: A retrospective, multicenter US study". Neurology. 86 (22): 2085–93. doi:10.1212/WNL.0000000000002723. PMID 27164698. S2CID 20818721.
- Leake JA, Albani S, Kao AS, Senac MO, Billman GF, Nespeca MP, et al. (August 2004). "Acute disseminated encephalomyelitis in childhood: epidemiologic, clinical and laboratory features". The Pediatric Infectious Disease Journal. 23 (8): 756–64. doi:10.1097/01.inf.0000133048.75452.dd. PMID 15295226. S2CID 31668039.
- Hynson JL, Kornberg AJ, Coleman LT, Shield L, Harvey AS, Kean MJ (May 2001). "Clinical and neuroradiologic features of acute disseminated encephalomyelitis in children". Neurology. 56 (10): 1308–12. doi:10.1212/WNL.56.10.1308. PMID 11376179. S2CID 23898511.
- Anlar B, Basaran C, Kose G, Guven A, Haspolat S, Yakut A, et al. (August 2003). "Acute disseminated encephalomyelitis in children: outcome and prognosis". Neuropediatrics. 34 (4): 194–99. doi:10.1055/s-2003-42208. PMID 12973660.
- Schwarz S, Mohr A, Knauth M, Wildemann B, Storch-Hagenlocher B (May 2001). "Acute disseminated encephalomyelitis: a follow-up study of 40 adult patients". Neurology. 56 (10): 1313–18. doi:10.1212/WNL.56.10.1313. PMID 11376180. S2CID 25391094.
- Bhatt P, Bray L, Raju S, Dapaah-Siakwan F, Patel A, Chaudhari R, et al. (March 2019). "Temporal Trends of Pediatric Hospitalizations with Acute Disseminated Encephalomyelitis in the United States: An Analysis from 2006 to 2014 using National Inpatient Sample". The Journal of Pediatrics. 206: 26–32.e1. doi:10.1016/j.jpeds.2018.10.044. PMID 30528761. S2CID 54478510.
- Koelman DL, Mateen FJ (September 2015). "Acute disseminated encephalomyelitis: current controversies in diagnosis and outcome". Journal of Neurology. 262 (9): 2013–24. doi:10.1007/s00415-015-7694-7. PMID 25761377. S2CID 26642207.
- Menge T, Kieseier BC, Nessler S, Hemmer B, Hartung HP, Stüve O (June 2007). "Acute disseminated encephalomyelitis: an acute hit against the brain". Current Opinion in Neurology. 20 (3): 247–54. doi:10.1097/WCO.0b013e3280f31b45. PMID 17495616. S2CID 14049476.
- Wingerchuk DM (May 2003). "Postinfectious encephalomyelitis". Current Neurology and Neuroscience Reports. 3 (3): 256–64. doi:10.1007/s11910-003-0086-x. PMID 12691631. S2CID 453016.
- Poser CM (May 2008). "Multiple sclerosis and recurrent disseminated encephalomyelitis are different diseases". Archives of Neurology. 65 (5): 674, author reply 674–75. doi:10.1001/archneur.65.5.674-a. PMID 18474749.
- Dale RC, de Sousa C, Chong WK, Cox TC, Harding B, Neville BG (December 2000). "Acute disseminated encephalomyelitis, multiphasic disseminated encephalomyelitis and multiple sclerosis in children". Brain. 123 (12): 2407–22. doi:10.1093/brain/123.12.2407. PMID 11099444.
- Di Pauli F, Höftberger R, Reindl M, Beer R, Rhomberg P, Schanda K, et al. (December 2015). "Fulminant demyelinating encephalomyelitis: Insights from antibody studies and neuropathology". Neurology. 2 (6): e175. doi:10.1212/NXI.0000000000000175. PMC 4635550. PMID 26587556.
- Tenembaum S, Chamoles N, Fejerman N (October 2002). "Acute disseminated encephalomyelitis: a long-term follow-up study of 84 pediatric patients". Neurology. 59 (8): 1224–31. doi:10.1212/WNL.59.8.1224. PMID 12391351. S2CID 37405227.
- Allmendinger A, Krauthamer A, Spektor V (2009). "Acute Disseminated Encephalomyelitis". Diagnostic Imaging. Case of the month. 31 (12): 10. Archived from the original on 24 February 2011.
- Manikanta AK, Pradeep GV, Pydi R, Chanumolu AR, Joy LA, Kancherla N (14 June 2021). "Acute Disseminated Encephalomyelitis in COVID 19- Systematic Review". Annals of the Romanian Society for Cell Biology. 25 (6): 11443–50.
- Novi G, Rossi T, Pedemonte E, Saitta L, Rolla C, Roccatagliata L, et al. (September 2020). "Acute disseminated encephalomyelitis after SARS-CoV-2 infection". Neurology. 7 (5): e797. doi:10.1212/NXI.0000000000000797. PMC 7286650. PMID 32482781.
- Reindl M, Di Pauli F, Rostásy K, Berger T (August 2013). "The spectrum of MOG autoantibody-associated demyelinating diseases". Nature Reviews. Neurology. 9 (8): 455–61. doi:10.1038/nrneurol.2013.118. PMID 23797245. S2CID 7219279.
- Weber MS, Derfuss T, Brück W (August 2018). "Anti-Myelin Oligodendrocyte Glycoprotein Antibody-Associated Central Nervous System Demyelination-A Novel Disease Entity?". JAMA Neurology. 75 (8): 909–10. doi:10.1001/jamaneurol.2018.1055. PMID 29913011.
- Kamel MG, Nam NT, Han NH, El-Shabouny AE, Makram AM, Abd-Elhay FA, et al. (June 2017). "Post-dengue acute disseminated encephalomyelitis: A case report and meta-analysis". PLOS Neglected Tropical Diseases. 11 (6): e0005715. doi:10.1371/journal.pntd.0005715. PMC 5509372. PMID 28665957.
- Fisher DL, Defres S, Solomon T (March 2015). "Measles-induced encephalitis". QJM. 108 (3): 177–82. doi:10.1093/qjmed/hcu113. PMID 24865261.
- Sample I (8 July 2020). "Warning of serious brain disorders in people with mild coronavirus symptoms". The Guardian. ISSN 0261-3077. Retrieved 8 July 2020.
- Tenembaum S, Chitnis T, Ness J, Hahn JS (April 2007). International Pediatric MS Study Group. "Acute disseminated encephalomyelitis". Neurology. 68 (16 Suppl 2): S23–36. doi:10.1212/01.wnl.0000259404.51352.7f. PMID 17438235. S2CID 19893165.
- Hemachudha T, Griffin DE, Giffels JJ, Johnson RT, Moser AB, Phanuphak P (February 1987). "Myelin basic protein as an encephalitogen in encephalomyelitis and polyneuritis following rabies vaccination". The New England Journal of Medicine. 316 (7): 369–74. doi:10.1056/NEJM198702123160703. PMID 2433582.
- Hemachudha T, Griffin DE, Johnson RT, Giffels JJ (January 1988). "Immunologic studies of patients with chronic encephalitis induced by post-exposure Semple rabies vaccine". Neurology. 38 (1): 42–44. doi:10.1212/WNL.38.1.42. PMID 2447520. S2CID 21992894.
- Murthy JM (September 2002). "Acute disseminated encephalomyelitis". Neurology India. 50 (3): 238–43. PMID 12391446.
- Fenichel GM (August 1982). "Neurological complications of immunization". Annals of Neurology. 12 (2): 119–28. doi:10.1002/ana.410120202. PMID 6751212. S2CID 2352985.
- Takahashi H, Pool V, Tsai TF, Chen RT (July 2000). "Adverse events after Japanese encephalitis vaccination: review of post-marketing surveillance data from Japan and the United States. The VAERS Working Group". Vaccine. 18 (26): 2963–69. doi:10.1016/S0264-410X(00)00111-0. PMID 10825597.
- Tourbah A, Gout O, Liblau R, Lyon-Caen O, Bougniot C, Iba-Zizen MT, Cabanis EA (July 1999). "Encephalitis after hepatitis B vaccination: recurrent disseminated encephalitis or MS?". Neurology. 53 (2): 396–401. doi:10.1212/WNL.53.2.396. PMID 10430433. S2CID 25061061.
- Karaali-Savrun F, Altintaş A, Saip S, Siva A (November 2001). "Hepatitis B vaccine related-myelitis?". European Journal of Neurology. 8 (6): 711–15. doi:10.1046/j.1468-1331.2001.00290.x. PMID 11784358. S2CID 30784630.
- Sejvar JJ, Labutta RJ, Chapman LE, Grabenstein JD, Iskander J, Lane JM (December 2005). "Neurologic adverse events associated with smallpox vaccination in the United States, 2002–2004". JAMA. 294 (21): 2744–50. doi:10.1001/jama.294.21.2744. PMID 16333010.
- Ozawa H, Noma S, Yoshida Y, Sekine H, Hashimoto T (August 2000). "Acute disseminated encephalomyelitis associated with poliomyelitis vaccine". Pediatric Neurology. 23 (2): 177–79. doi:10.1016/S0887-8994(00)00167-3. PMID 11020647.
- Stratton KR, Howe CJ, Johnston Jr RB, et al. (Institute of Medicine (US) Vaccine Safety Committee) (1994). Adverse Events Associated with Childhood Vaccines: Evidence Bearing on Causality. The National Academies Press. pp. 125–26. doi:10.17226/2138. ISBN 978-0-309-07496-4. PMID 25144097. Retrieved 6 December 2015.
- Gibbons JL, Miller HG, Stanton JB (October 1956). "Para-infectious encephalomyelitis and related syndromes; a critical review of the neurological complications of certain specific fevers". The Quarterly Journal of Medicine. 25 (100): 427–505. PMID 13379602.
- Cole J, Evans E, Mwangi M, Mar S (November 2019). "Acute Disseminated Encephalomyelitis in Children: An Updated Review Based on Current Diagnostic Criteria". Pediatric Neurology. 100: 26–34. doi:10.1016/j.pediatrneurol.2019.06.017. PMID 31371120.
- Tenembaum S, Chitnis T, Ness J, Hahn JS (April 2007). "Acute disseminated encephalomyelitis". Neurology. 68 (16 Suppl 2): S23–36. doi:10.1212/01.wnl.0000259404.51352.7f. PMID 17438235. S2CID 19893165.
- Wingerchuk DM, Lucchinetti CF (June 2007). "Comparative immunopathogenesis of acute disseminated encephalomyelitis, neuromyelitis optica, and multiple sclerosis". Current Opinion in Neurology. 20 (3): 343–50. doi:10.1097/WCO.0b013e3280be58d8. PMID 17495631. S2CID 17386506.
- Weinshenker B, Miller D (1999). "Multiple sclerosis: one disease or many?". In Siva A, Kesselring J, Thompson A (eds.). Frontiers in multiple sclerosis. London: Dunitz. pp. 37–46. ISBN 978-1-85317-506-0.
- Hartung HP, Grossman RI (May 2001). "ADEM: distinct disease or part of the MS spectrum?". Neurology. 56 (10): 1257–60. doi:10.1212/WNL.56.10.1257. PMID 11376169.
- Krupp LB, Banwell B, Tenembaum S, et al. (International Pediatric MS Study Group) (April 2007). "Consensus definitions proposed for pediatric multiple sclerosis and related disorders". Neurology. 68 (16 Suppl 2): S7–12. doi:10.1212/01.wnl.0000259422.44235.a8. PMID 17438241. S2CID 26001350.
- Lassmann H (February 2010). "Acute disseminated encephalomyelitis and multiple sclerosis". Brain. 133 (Pt 2): 317–19. doi:10.1093/brain/awp342. PMID 20129937.
- McDonald WI, Compston A, Edan G, Goodkin D, Hartung HP, Lublin FD, et al. (July 2001). "Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis". Annals of Neurology. 50 (1): 121–27. CiteSeerX 10.1.1.466.5368. doi:10.1002/ana.1032. PMID 11456302. S2CID 13870943.
- Young NP, Weinshenker BG, Parisi JE, Scheithauer B, Giannini C, Roemer SF, et al. (February 2010). "Perivenous demyelination: association with clinically defined acute disseminated encephalomyelitis and comparison with pathologically confirmed multiple sclerosis". Brain. 133 (Pt 2): 333–48. doi:10.1093/brain/awp321. PMC 2822631. PMID 20129932.
- Young NP, Weinshenker BG, Lucchinetti CF (February 2008). "Acute Disseminated Encephalomyelitis: Current Understanding and Controversies". Seminars in Neurology. 28 (1): 84–94. doi:10.1055/s-2007-1019130. PMID 18256989.
- Guenther AD, Munoz DG (2013). "Plaque-like demyelination in acute disseminated encephalomyelitis (ADEM) – an autopsy case report". Clinical Neuropathology. 32 (6): 486–91. doi:10.5414/NP300634. PMID 23863345.
- Lu Z, Zhang B, Qiu W, Kang Z, Shen L, Long Y, et al. (2011). "Comparative brain stem lesions on MRI of acute disseminated encephalomyelitis, neuromyelitis optica, and multiple sclerosis". PLOS ONE. 6 (8): e22766. Bibcode:2011PLoSO...622766L. doi:10.1371/journal.pone.0022766. PMC 3154259. PMID 21853047.
- Baumann M, Hennes EM, Schanda K, Karenfort M, Bajer-Kornek B, Diepold K, et al. (May 2015). "OP65–3006: Clinical characteristics and neuroradiological findings in children with multiphasic demyelinating encephalomyelitis and MOG antibodies". European Journal of Paediatric Neurology. Abstracts of the 11th EPNS Congress. 19 (supplement 1): S21. doi:10.1016/S1090-3798(15)30066-0.
- Baumann M, Hennes EM, Schanda K, Karenfort M, Kornek B, Seidl R, et al. (December 2016). "Children with multiphasic disseminated encephalomyelitis and antibodies to the myelin oligodendrocyte glycoprotein (MOG): Extending the spectrum of MOG antibody positive diseases". Multiple Sclerosis. 22 (14): 1821–29. doi:10.1177/1352458516631038. PMID 26869530. S2CID 30428892.
- Davies NW, Sharief MK, Howard RS (July 2006). "Infection-associated encephalopathies: their investigation, diagnosis, and treatment". Journal of Neurology. 253 (7): 833–45. doi:10.1007/s00415-006-0092-4. PMID 16715200. S2CID 26350300.
- Stone MJ, Hawkins CP (2007). "A medical overview of encephalitis". Neuropsychological Rehabilitation. 17 (4–5): 429–49. doi:10.1080/09602010601069430. PMID 17676529. S2CID 24249705.
- Archer H, Wall R (February 2003). "Acute haemorrhagic leukoencephalopathy: two case reports and review of the literature". The Journal of Infection. 46 (2): 133–37. doi:10.1053/jinf.2002.1096. PMID 12634076.
- Venugopal V, Haider M (2013). "First case report of acute hemorrhagic leukoencephalitis following Plasmodium vivax infection". Indian Journal of Medical Microbiology. 31 (1): 79–81. doi:10.4103/0255-0857.108736. PMID 23508437.
- Yildiz Ö, Pul R, Raab P, Hartmann C, Skripuletz T, Stangel M (September 2015). "Acute hemorrhagic leukoencephalitis (Weston-Hurst syndrome) in a patient with relapse-remitting multiple sclerosis". Journal of Neuroinflammation. 12 (1): 175. doi:10.1186/s12974-015-0398-1. PMC 4574135. PMID 26376717.
- Mondia MW, Reyes NG, Espiritu AI, Pascual V JL (September 2019). "Acute hemorrhagic leukoencephalitis of Weston Hurst secondary to herpes encephalitis presenting as status epilepticus: A case report and review of literature". Journal of Clinical Neuroscience. 67: 265–70. doi:10.1016/j.jocn.2019.06.020. PMID 31239199. S2CID 195261409.
- Shahar E, Andraus J, Savitzki D, Pilar G, Zelnik N (November 2002). "Outcome of severe encephalomyelitis in children: effect of high-dose methylprednisolone and immunoglobulins". Journal of Child Neurology. 17 (11): 810–14. doi:10.1177/08830738020170111001. PMID 12585719. S2CID 25519230.
- Ravaglia S, Piccolo G, Ceroni M, Franciotta D, Pichiecchio A, Bastianello S, et al. (November 2007). "Severe steroid-resistant post-infectious encephalomyelitis: general features and effects of IVIg". Journal of Neurology. 254 (11): 1518–23. doi:10.1007/s00415-007-0561-4. PMID 17965959. S2CID 21922460.
- Straussberg R, Schonfeld T, Weitz R, Karmazyn B, Harel L (February 2001). "Improvement of atypical acute disseminated encephalomyelitis with steroids and intravenous immunoglobulins". Pediatric Neurology. 24 (2): 139–43. doi:10.1016/S0887-8994(00)00229-0. PMID 11275464.
- Feasby T, Banwell B, Benstead T, Bril V, Brouwers M, Freedman M, et al. (April 2007). "Guidelines on the use of intravenous immune globulin for neurologic conditions". Transfusion Medicine Reviews. 21 (2 Suppl 1): S57–107. doi:10.1016/j.tmrv.2007.01.002. PMID 17397768.
- Kamel MG, Nam NT, Han NH, El-Shabouny AE, Makram AM, Abd-Elhay FA, et al. (June 2017). "Post-dengue acute disseminated encephalomyelitis: A case report and meta-analysis". PLOS Neglected Tropical Diseases. 11 (6): e0005715. doi:10.1371/journal.pntd.0005715. PMC 5509372. PMID 28665957.
- Lin CH, Jeng JS, Hsieh ST, Yip PK, Wu RM (February 2007). "Acute disseminated encephalomyelitis: a follow-up study in Taiwan". Journal of Neurology, Neurosurgery, and Psychiatry. 78 (2): 162–67. doi:10.1136/jnnp.2005.084194. PMC 2077670. PMID 17028121.
- Malo-Pion C, Lambert R, Décarie JC, Turpin S (February 2018). "Imaging of Acquired Demyelinating Syndrome With 18F-FDG PET/CT". Clinical Nuclear Medicine. 43 (2): 103–05. doi:10.1097/RLU.0000000000001916. PMID 29215409.
- Foong J, Rozewicz L, Quaghebeur G, Davie CA, Kartsounis LD, Thompson AJ, et al. (January 1997). "Executive function in multiple sclerosis. The role of frontal lobe pathology". Brain. 120 (1): 15–26. doi:10.1093/brain/120.1.15. PMID 9055794.
- Hahn CD, Miles BS, MacGregor DL, Blaser SI, Banwell BL, Hetherington CR (August 2003). "Neurocognitive outcome after acute disseminated encephalomyelitis". Pediatric Neurology. 29 (2): 117–23. doi:10.1016/S0887-8994(03)00143-7. PMID 14580654.
- Banwell BL, Anderson PE (March 2005). "The cognitive burden of multiple sclerosis in children". Neurology. 64 (5): 891–94. doi:10.1212/01.WNL.0000152896.35341.51. PMID 15753431. S2CID 6532050.
- Jacobs RK, Anderson VA, Neale JL, Shield LK, Kornberg AJ (September 2004). "Neuropsychological outcome after acute disseminated encephalomyelitis: impact of age at illness onset". Pediatric Neurology. 31 (3): 191–97. doi:10.1016/j.pediatrneurol.2004.03.008. PMID 15351018.
- Douglas JW (August 1975). "Early hospital admissions and later disturbances of behaviour and learning". Developmental Medicine and Child Neurology. 17 (4): 456–80. doi:10.1111/j.1469-8749.1975.tb03497.x. PMID 1158052. S2CID 19270009.
- Daviss WB, Racusin R, Fleischer A, Mooney D, Ford JD, McHugo GJ (May 2000). "Acute stress disorder symptomatology during hospitalization for pediatric injury". Journal of the American Academy of Child and Adolescent Psychiatry. 39 (5): 569–75. doi:10.1097/00004583-200005000-00010. PMID 10802974.
- Misu T, Fujihara K (February 2019). "Neuromyelitis optica spectrum and myelin oligodendrocyte glycoprotein antibody‐related disseminated encephalomyelitis". Clinical and Experimental Neuroimmunology. 10 (1): 9–17. doi:10.1111/cen3.12491. S2CID 59566930.
- Rivers TM, Schwentker FF (April 1935). "Encephalomyelitis accompanied by myelin destruction experimentally produced in monkeys". The Journal of Experimental Medicine. 61 (5): 689–702. doi:10.1084/jem.61.5.689. PMC 2133246. PMID 19870385.
- Sriram S, Steiner I (December 2005). "Experimental allergic encephalomyelitis: a misleading model of multiple sclerosis". Annals of Neurology. 58 (6): 939–45. doi:10.1002/ana.20743. PMID 16315280. S2CID 12141651.
External links
- Acute disseminated encephalomyelitis at NIH's Office of Rare Diseases
- Acute Disseminated Encephalomyelitis Information Page at NINDS
- Information for parents about Acute disseminated encephalomyelitis