Renal cell carcinoma
Renal cell carcinoma (RCC) is a kidney cancer that originates in the lining of the proximal convoluted tubule, a part of the very small tubes in the kidney that transport primary urine. RCC is the most common type of kidney cancer in adults, responsible for approximately 90–95% of cases.[1] RCC occurrence shows a male predominance over women with a ratio of 1.5:1. RCC most commonly occurs between 6th and 7th decade of life.[2]
| Renal cell carcinoma | |
|---|---|
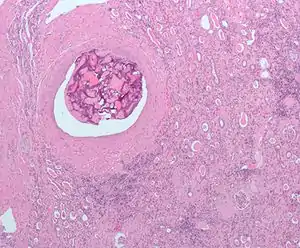
| Micrograph of the most common type of renal cell carcinoma (clear cell)—on right of the image; non-tumour kidney is on the left of the image. Nephrectomy specimen. H&E stain | |
| Specialty | Oncology |
Initial treatment is most commonly either partial or complete removal of the affected kidney(s).[3] Where the cancer has not metastasised (spread to other organs) or burrowed deeper into the tissues of the kidney, the five-year survival rate is 65–90%,[4] but this is lowered considerably when the cancer has spread.
The body is remarkably good at hiding the symptoms and as a result people with RCC often have advanced disease by the time it is discovered.[5] The initial symptoms of RCC often include blood in the urine (occurring in 40% of affected persons at the time they first seek medical attention), flank pain (40%), a mass in the abdomen or flank (25%), weight loss (33%), fever (20%), high blood pressure (20%), night sweats and generally feeling unwell.[1] When RCC metastasises, it most commonly spreads to the lymph nodes, lungs, liver, adrenal glands, brain or bones.[6] Immunotherapy and targeted therapy have improved the outlook for metastatic RCC.[7][8]
RCC is also associated with a number of paraneoplastic syndromes (PNS) which are conditions caused by either the hormones produced by the tumour or by the body's attack on the tumour and are present in about 20% of those with RCC.[1] These syndromes most commonly affect tissues which have not been invaded by the cancer.[1] The most common PNSs seen in people with RCC are: high blood calcium levels, high red blood cell count, high platelet count and secondary amyloidosis.[6]
Signs and symptoms
Historically, medical practitioners expected a person to present with three findings. This classic triad[9] is 1: haematuria, which is when there is blood present in the urine, 2: flank pain, which is pain on the side of the body between the hip and ribs, and 3: an abdominal mass, similar to bloating but larger. It is now known that this classic triad of symptoms only occurs in 10–15% of cases, and is usually indicative that the renal cell carcinoma (RCC) is in an advanced stage.[9] Today, RCC is often asymptomatic (meaning few to no symptoms) and is generally detected incidentally when a person is being examined for other ailments.[10]
Other signs and symptom may include haematuria;[9] loin pain;[9] abdominal mass;[10] malaise, which is a general feeling of unwellness;[10] weight loss and/or loss of appetite;[11] anaemia resulting from depression of erythropoietin;[9] erythrocytosis (increased production of red blood cells) due to increased erythropoietin secretion;[9] varicocele, which is seen in males as an enlargement of the pampiniform plexus of veins draining the testis (more often the left testis)[10] hypertension (high blood pressure) resulting from secretion of renin by the tumour;[12] hypercalcemia, which is elevation of calcium levels in the blood;[13] sleep disturbance or night sweats;[11] recurrent fevers;[11] and chronic fatigue.[14]
Risk factors
Lifestyle
The greatest risk factors for RCC are lifestyle-related; smoking, obesity and hypertension (high blood pressure) have been estimated to account for up to 50% of cases.[15] Occupational exposure to some chemicals such as asbestos, cadmium, lead, chlorinated solvents, petrochemicals and PAH (polycyclic aromatic hydrocarbon) has been examined by multiple studies with inconclusive results.[16][17][18] Another suspected risk factor is the long term use of non-steroidal anti-inflammatory drugs (NSAIDS).[19]
Finally, studies have found that women who have had a hysterectomy are at more than double the risk of developing RCC than those who have not.[20] Moderate alcohol consumption, on the other hand, has been shown to have a protective effect.[21]
Genetics
Hereditary factors have a minor impact on individual susceptibility with immediate relatives of people with RCC having a two to fourfold increased risk of developing the condition.[22] Other genetically linked conditions also increase the risk of RCC, including hereditary papillary renal carcinoma, hereditary leiomyomatosis, Birt–Hogg–Dube syndrome, hyperparathyroidism-jaw tumor syndrome, familial papillary thyroid carcinoma, von Hippel–Lindau disease[23] and sickle cell disease.[24]
The most significant disease affecting risk however is not genetically linked – patients with acquired cystic disease of the kidney requiring dialysis are 30 times more likely than the general population to develop RCC.[25]
Pathophysiology
The tumour arises from the cells of the proximal renal tubular epithelium.[1] It is considered an adenocarcinoma.[6] There are two subtypes: sporadic (that is, non-hereditary) and hereditary.[1] Both such subtypes are associated with mutations in the short-arm of chromosome 3, with the implicated genes being either tumour suppressor genes (VHL and TSC) or oncogenes (like c-Met).[1]
Diagnosis
The first steps taken to diagnose this condition are consideration of the signs and symptoms, and a medical history (the detailed medical review of past health state) to evaluate any risk factors. Based on the symptoms presented, a range of biochemical tests (using blood and/or urine samples) may also be considered as part of the screening process to provide sufficient quantitative analysis of any differences in electrolytes, kidney and liver function, and blood clotting times.[24] Upon physical examination, palpation of the abdomen may reveal the presence of a mass or an organ enlargement.[26]
Although this disease lacks characterization in the early stages of tumor development, considerations based on diverse clinical manifestations, as well as resistance to radiation and chemotherapy are important. The main diagnostic tools for detecting renal cell carcinoma are ultrasound, computed tomography (CT) scanning and magnetic resonance imaging (MRI) of the kidneys.[27]
Classification
Renal cell carcinoma (RCC) is not a single entity, but rather a collection of different types of tumours, each derived from the various parts of the nephron (epithelium or renal tubules) and possessing distinct genetic characteristics, histological features, and, to some extent, clinical phenotypes.[24]
| Classification of the Common Histological Subtypes of Renal Cell Carcinoma[24] | |||
|---|---|---|---|
| Renal Cell Carcinoma Subtype | Frequency | Genetic Abnormalities | Characteristics |
|
Clear Cell Renal Cell Carcinoma (CCRCC) Generally the cells have a clear cytoplasm, are surrounded by a distinct cell membrane and contain round and uniform nuclei. |
60–70% |
|
|
Papillary Renal Cell Carcinoma (PRCC)
 Type 1 PRCC consist of papillae covered with a single or double layer of small cuboid cells with scanty cytoplasm and Type 2 PRCC consist of papillae covered by large eosinophilic cells arranged in an irregular or pseudostratified manner. |
10–15% |
|
|
Chromophobe Renal Cell Carcinoma (ChRCC)
 ChRCC consists of tumor cells with abundant eosinophilic cytoplasm (pale cells and eosinophilic cells with a perinuclear halo) and show mainly a solid structure. |
3–5% |
|
|
| Clinical, Pathological and Genetic Features of Uncommon RCC Subtypes Included in the 2004 WHO Classification of RCC Pathology[29][32] | ||||
|---|---|---|---|---|
| RCC subtype | Clinical features | Cell/Tissue Characteristics | Genetics | Prognosis |
| Multilocular Cystic RCC |
|
Clear cytoplasm, small dark nuclei | 3p deletion as observed in CCRCC |
|
| Carcinoma of the Collecting Ducts of Bellini |
|
High-grade tumor cells with eosinophilic cytoplasm | Variable results: LOH on chromosomes 1q, 6p, 8p,9p, 13q, 19q32 and 21q; c-erB2 amplification associated with unfavorable outcome |
|
| Medullary Carcinoma |
|
Haemorrhage and necrosis, high-grade tumour cells with eosinophilic cytoplasm | Not well defined |
|
| Xp11.2 Translocation Carcinoma |
|
|
Chromosomal translocation involving TFE3 gene on Xp11.2 resulting in overexpression of the TFE3 protein |
|
| Mucinous Tubular Spindle Cell Carcinoma |
|
Tubules, extracellular mucin and spindle cells | Not well defined; Losses involving chromosomes 1, 4, 6, 8, 9, 11, 13, 14, 15, 18, 22 reported; 3p alterations and gain of chromosome 7, and 17 not present |
|
| Post-Neuroblastoma Renal Cell Carcinoma |
|
Eosinophilic cells with oncocytoid features (same as CCRCC) | Not well defined; Loss of multiple chromosomal loci observed | Similar to other common RCC subtypes |
Array-based karyotyping can be used to identify characteristic chromosomal aberrations in renal tumors with challenging morphology.[33][34] Array-based karyotyping performs well on paraffin embedded tumours[35] and is amenable to routine clinical use. See also Virtual Karyotype for CLIA certified laboratories offering array-based karyotyping of solid tumours.
The 2004 World Health Organization (WHO) classification of genitourinary tumours recognizes over 40 subtypes of renal neoplasms. Since the publication of the latest iteration of the WHO classification in 2004, several novel renal tumour subtypes have been described:[36]
- Clear cell papillary renal cell carcinoma and clear cell renal cell carcinoma with smooth muscle stroma[37]
- Mucinous tubular and spindle cell carcinoma (MTSCC) [36]
- Multilocular cystic clear cell renal cell carcinoma[36]
- Tubulocystic renal cell carcinoma
- Thyroid-like follicular renal cell carcinoma
- Acquired cystic kidney disease-associated renal cell carcinoma
- Renal cell carcinoma with t(6;11) translocation (TFEB)
- Hybrid oncocytoma/chromophobe renal cell carcinoma
- Hereditary leiomyomatosis and renal cell carcinoma (HLRCC)
Laboratory tests
Laboratory tests are generally conducted when the patient presents with signs and symptoms that may be characteristic of kidney impairment. They are not primarily used to diagnose kidney cancer, due to its asymptomatic nature and are generally found incidentally during tests for other illnesses such as gallbladder disease.[38] In other words, these cancers are not detected usually because they do not cause pain or discomfort when they are discovered. Laboratory analysis can provide an assessment on the overall health of the patient and can provide information in determining the staging and degree of metastasis to other parts of the body (if a renal lesion has been identified) before treatment is given.
Urine analysis
The presence of blood in urine is a common presumptive sign of renal cell carcinoma. The haemoglobin of the blood causes the urine to be rusty, brown or red in colour. Alternatively, urinalysis can test for sugar, protein and bacteria which can also serve as indicators for cancer. A complete blood cell count can also provide additional information regarding the severity and spreading of the cancer.[39]
Complete blood cell count
The CBC provides a quantified measure of the different cells in the whole blood sample from the patient. Such cells examined for in this test include red blood cells (erythrocytes), white blood cells (leukocytes) and platelets (thrombocytes). A common sign of renal cell carcinoma is anaemia whereby the patient exhibits deficiency in red blood cells.[40] CBC tests are vital as a screening tool for examination the health of patient prior to surgery. Inconsistencies with platelet counts are also common amongst these cancer patients and further coagulation tests, including erythrocyte sedimentation rate (ESR), prothrombin time (PT), activated partial thromboplastin time (APTT) should be considered.
Blood chemistry
Blood chemistry tests are conducted if renal cell carcinoma is suspected as cancer has the potential to elevate levels of particular chemicals in blood. For example, liver enzymes such as aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are found to be at abnormally high levels.[41] The staging of the cancer can also be determined by abnormal elevated levels of calcium, which suggests that the cancer may have metastasised to the bones.[42] In this case, a doctor should be prompted for a CT scan. Blood chemistry tests also assess the overall function of the kidneys and can allow the doctor to decide upon further radiological tests.
Radiology
The characteristic appearance of renal cell carcinoma (RCC) is a solid renal lesion which disturbs the renal contour. It will frequently have an irregular or lobulated margin and may be seen as a lump on the lower pelvic or abdomen region. Traditionally, 85 to 90% of solid renal masses will turn out to be RCC but cystic renal masses may also be due to RCC.[43] However, the advances of diagnostic modalities are able to incidentally diagnose a great proportion of patients with renal lesions that may appear to be small in size and of benign state. Ten percent of RCC will contain calcifications, and some contain macroscopic fat (likely due to invasion and encasement of the perirenal fat).[44]
Deciding on the benign or malignant nature of the renal mass on the basis of its localized size is an issue as renal cell carcinoma may also be cystic. As there are several benign cystic renal lesions (simple renal cyst, haemorrhagic renal cyst, multilocular cystic nephroma, polycystic kidney disease), it may occasionally be difficult for the radiologist to differentiate a benign cystic lesion from a malignant one.[45] The Bosniak classification system for cystic renal lesions classifies them into groups that are benign and those that need surgical resection, based on specific imaging features.[46]
The main imaging tests performed in order to identify renal cell carcinoma are pelvic and abdominal CT scans, ultrasound tests of the kidneys (ultrasonography), MRI scans, intravenous pyelogram (IVP) or renal angiography.[47] Among these main diagnostic tests, other radiologic tests such as excretory urography, positron-emission tomography (PET) scanning, ultrasonography, arteriography, venography, and bone scanning can also be used to aid in the evaluation of staging renal masses and to differentiate non-malignant tumours from malignant tumours.
Computed tomography
Contrast-enhanced computed tomography (CT) scanning is routinely used to determine the stage of the renal cell carcinoma in the abdominal and pelvic regions. CT scans have the potential to distinguish solid masses from cystic masses and may provide information on the localization, stage or spread of the cancer to other organs of the patient. Key parts of the human body which are examined for metastatic involvement of renal cell carcinoma may include the renal vein, lymph node and the involvement of the inferior vena cava.[48] According to a study conducted by Sauk et al., multidetector CT imaging characteristics have applications in diagnosing patients with clear renal cell carcinoma by depicting the differences of these cells at the cytogenic level.[49]
Ultrasound
Ultrasonographic examination can be useful in evaluating questionable asymptomatic kidney tumours and cystic renal lesions if computed tomography imaging is inconclusive. This safe and non-invasive radiologic procedure uses high frequency sound waves to generate an interior image of the body on a computer monitor. The image generated by the ultrasound can help diagnose renal cell carcinoma based on the differences of sound reflections on the surface of organs and the abnormal tissue masses. Essentially, ultrasound tests can determine whether the composition of the kidney mass is mainly solid or filled with fluid.[47]
A percutaneous biopsy can be performed by a radiologist using ultrasound or computed tomography to guide sampling of the tumour for the purpose of diagnosis by pathology. However this is not routinely performed because when the typical imaging features of renal cell carcinoma are present, the possibility of an incorrectly negative result together with the risk of a medical complication to the patient may make it unfavourable from a risk-benefit perspective.[50] However, biopsy tests for molecular analysis to distinguish benign from malignant renal tumours is of investigative interest.[50]
Magnetic resonance imaging
Magnetic resonance imaging (MRI) scans provide an image of the soft tissues in the body using radio waves and strong magnets. MRI can be used instead of CT if the patient exhibits an allergy to the contrast media administered for the test.[51][52] Sometimes prior to the MRI scan, an intravenous injection of a contrasting material called gadolinium is given to allow for a more detailed image. Patients on dialysis or those who have renal insufficiency should avoid this contrasting material as it may induce a rare, yet severe, side effect known as nephrogenic systemic fibrosis.[53] A bone scan or brain imaging is not routinely performed unless signs or symptoms suggest potential metastatic involvement of these areas. MRI scans should also be considered to evaluate tumour extension which has grown in major blood vessels, including the vena cava, in the abdomen. MRI can be used to observe the possible spread of cancer to the brain or spinal cord should the patient present symptoms that suggest this might be the case.
Intravenous pyelogram
Intravenous pyelogram (IVP) is a useful procedure in detecting the presence of abnormal renal mass in the urinary tract. This procedure involves the injection of a contrasting dye into the arm of the patient. The dye travels from the blood stream and into the kidneys which in time, passes into the kidneys and bladder. This test is not necessary if a CT or MRI scan has been conducted.[54]
Renal angiography
Renal angiography uses the same principle as IVP, as this type of X-ray also uses a contrasting dye. This radiologic test is important in diagnosing renal cell carcinoma as an aid for examining blood vessels in the kidneys. This diagnostic test relies on the contrasting agent which is injected in the renal artery to be absorbed by the cancerous cells.[55] The contrasting dye provides a clearer outline of abnormally-oriented blood vessels believed to be involved with the tumour. This is imperative for surgeons as it allows the patient's blood vessels to be mapped prior to operation.[48]
Staging
The staging of renal cell carcinoma is the most important factor in predicting its prognosis.[56] Staging can follow the TNM staging system, where the size and extent of the tumour (T), involvement of lymph nodes (N) and metastases (M) are classified separately. Also, it can use overall stage grouping into stage I–IV, with the 1997 revision of AJCC described below:[56]
| Stage I | Tumour of a diameter of 7 cm (approx. 2 3⁄4 inches) or smaller, and limited to the kidney. No lymph node involvement or metastases to distant organs. |
| Stage II | Tumour larger than 7.0 cm but still limited to the kidney. No lymph node involvement or metastases to distant organs. |
| Stage III any of the following | Tumor of any size with involvement of a nearby lymph node but no metastases to distant organs. Tumour of this stage may be with or without spread to fatty tissue around the kidney, with or without spread into the large veins leading from the kidney to the heart. |
| Tumour with spread to fatty tissue around the kidney and/or spread into the large veins leading from the kidney to the heart, but without spread to any lymph nodes or other organs. | |
| Stage IV any of the following | Tumour that has spread directly through the fatty tissue and the fascia ligament-like tissue that surrounds the kidney. |
| Involvement of more than one lymph node near the kidney | |
| Involvement of any lymph node not near the kidney | |
| Distant metastases, such as in the lungs, bone, or brain. |
At diagnosis, 30% of renal cell carcinomas have spread to the ipsilateral renal vein, and 5–10% have continued into the inferior vena cava.[57]
Histopathology



The gross and microscopic appearance of renal cell carcinomas is highly variable. The renal cell carcinoma may present reddened areas where blood vessels have bled, and cysts containing watery fluids.[58] The body of the tumour shows large blood vessels that have walls composed of cancerous cells. Gross examination often shows a yellowish, multilobulated tumor in the renal cortex, which frequently contains zones of necrosis, haemorrhage and scarring. In a microscopic context, there are four major histologic subtypes of renal cell cancer: clear cell (conventional RCC, 75%), papillary (15%), chromophobic (5%), and collecting duct (2%). Sarcomatoid changes (morphology and patterns of IHC that mimic sarcoma, spindle cells) can be observed within any RCC subtype and are associated with more aggressive clinical course and worse prognosis. Under light microscopy, these tumour cells can exhibit papillae, tubules or nests, and are quite large, atypical, and polygonal.
Recent studies have brought attention to the close association of the type of cancerous cells to the aggressiveness of the condition. Some studies suggest that these cancerous cells accumulate glycogen and lipids, their cytoplasm appear "clear", the nuclei remain in the middle of the cells, and the cellular membrane is evident.[59] Some cells may be smaller, with eosinophilic cytoplasm, resembling normal tubular cells. The stroma is reduced, but well vascularised. The tumour compresses the surrounding parenchyma, producing a pseudocapsule.[60]
The most common cell type exhibited by renal cell carcinoma is the clear cell, which is named by the dissolving of the cells' high lipid content in the cytoplasm. The clear cells are thought to be the least likely to spread and usually respond more favourably to treatment. However, most of the tumours contain a mixture of cells. The most aggressive stage of renal cancer is believed to be the one in which the tumour is mixed, containing both clear and granular cells.[61]
The recommended histologic grading schema for RCC is the Fuhrman system (1982), which is an assessment based on the microscopic morphology of a neoplasm with haematoxylin and eosin (H&E staining). This system categorises renal cell carcinoma with grades 1, 2, 3, 4 based on nuclear characteristics. The details of the Fuhrman grading system for RCC are shown below:[62]
| Grade Level | Nuclear Characteristics |
|---|---|
| Grade I | Nuclei appear round and uniform, 10 μm; nucleoli are inconspicuous or absent. |
| Grade II | Nuclei have an irregular appearance with signs of lobe formation, 15 μm; nucleoli are evident. |
| Grade III | Nuclei appear very irregular, 20 μm; nucleoli are large and prominent. |
| Grade IV | Nuclei appear bizarre and multilobated, 20 μm or more; nucleoli are prominent. |
Nuclear grade is believed to be one of the most imperative prognostic factors in patients with renal cell carcinoma.[24] However, a study by Delahunt et al. (2007) has shown that the Fuhrman grading is ideal for clear cell carcinoma but may not be appropriate for chromophobe renal cell carcinomas and that the staging of cancer (accomplished by CT scan) is a more favourable predictor of the prognosis of this disease.[63] In relation to renal cancer staging, the Heidelberg classification system of renal tumours was introduced in 1976 as a means of more completely correlating the histopathological features with the identified genetic defects.[64]
Prevention
The risk of renal cell carcinoma can be reduced by maintaining a normal body weight.[65]
Management
The type of treatment depends on multiple factors and the individual, some of which include the stage of renal cell carcinoma (organs and parts of the body affected/unaffected), type of renal cell carcinoma, pre-existing or comorbid conditions and overall health and age of the person.[9][66] Every form of treatment has both risks and benefits; a health care professional will provide the best options that suit the individual circumstances.
If it has spread outside of the kidneys, often into the lymph nodes, the lungs or the main vein of the kidney, then multiple therapies are used including surgery and medications. RCC is resistant to chemotherapy and radiotherapy in most cases but does respond well to immunotherapy with interleukin-2 or interferon-alpha, biologic, or targeted therapy. In early-stage cases, cryotherapy and surgery are the preferred options.
Active surveillance
Active surveillance or "watchful waiting" is becoming more common as small renal masses or tumours are being detected and also within the older generation when surgery is not always suitable.[67] Active surveillance involves completing various diagnostic procedures, tests and imaging to monitor the progression of the RCC before embarking on a more high risk treatment option like surgery.[67] In the elderly, patients with co-morbidities, and in poor surgical candidates, this is especially useful.
Surgery
Different procedures may be most appropriate, depending on circumstances.
The recommended treatment for renal cell cancer may be nephrectomy or partial nephrectomy, surgical removal of all or part of the kidney.[3] This may include some of the surrounding organs or tissues or lymph nodes. If cancer is only in the kidneys, which is about 60% of cases, it can be cured roughly 90% of the time with surgery.
Small renal tumors (< 4 cm) are treated increasingly by partial nephrectomy when possible.[68][69][70] Most of these small renal masses manifest indolent biological behavior with excellent prognosis.[71] Nephron-sparing partial nephrectomy is used when the tumor is small (less than 4 cm in diameter) or when the patient has other medical concerns such as diabetes or hypertension.[9] The partial nephrectomy involves the removal of the affected tissue only, sparing the rest of the kidney, Gerota's fascia and the regional lymph nodes. This allows for more renal preservation as compared to the radical nephrectomy, and this can have positive long-term health benefits.[72] Larger and more complex tumors can also be treated with partial nephrectomy by surgeons with a lot of kidney surgery experience.[73]
Surgical nephrectomy may be "radical" if the procedure removes the entire affected kidney including Gerota's fascia, the adrenal gland which is on the same side as the affected kidney, and the regional retroperitoneal lymph nodes, all at the same time.[9] This method, although severe, is effective. But it is not always appropriate, as it is a major surgery that contains the risk of complication both during and after the surgery and can have a longer recovery time.[74] It is important to note that the other kidney must be fully functional, and this technique is most often used when there is a large tumour present in only one kidney.

In cases where the tumor has spread into the renal vein, inferior vena cava, and possibly the right atrium, this portion of the tumor can be surgically removed, as well. When the tumor involved the inferior vena cava, it is important to classify which parts of the vena cava are involved and to plan accordingly, as sometimes complete resection will involve an incision into the chest with increased morbidity. For this reason, Dr. Gaetano Ciancio adapted liver mobilization techniques from liver transplant to address retrohepatic or even suprahepatic inferior vena caval thrombus associated with renal tumors.[75] With this technique, the whole abdominal inferior vena cava is able to be mobilized. This facilitates milking of the tumor down below the major hepatic veins by the surgeon's fingers, bypassing the need for a thoracoabdominal incision or cardiopulmonary bypass.[76] In cases of known metastases, surgical resection of the kidney ("cytoreductive nephrectomy") may improve survival,[77] as well as resection of a solitary metastatic lesion. Kidneys are sometimes embolized prior to surgery to minimize blood loss.[78]
Surgery is increasingly performed via laparoscopic techniques. Commonly referred to as key hole surgery, this surgery does not have the large incisions seen in a classically performed radical or partial nephrectomy, but still successfully removes either all or part of the kidney. Laparoscopic surgery is associated with shorter stays in the hospital and quicker recovery time but there are still risks associated with the surgical procedure. These have the advantage of being less of a burden for the patient and the disease-free survival is comparable to that of open surgery.[3] For small exophytic lesions that do not extensively involve the major vessels or urinary collecting system, a partial nephrectomy (also referred to as "nephron sparing surgery") can be performed. This may involve temporarily stopping blood flow to the kidney while the mass is removed as well as renal cooling with an ice slush. Mannitol can also be administered to help limit damage to the kidney. This is usually done through an open incision although smaller lesions can be done laparoscopically with or without robotic assistance.
Laparoscopic cryotherapy can also be done on smaller lesions. Typically a biopsy is taken at the time of treatment. Intraoperative ultrasound may be used to help guide placement of the freezing probes. Two freeze/thaw cycles are then performed to kill the tumor cells. As the tumor is not removed followup is more complicated (see below) and overall disease-free rates are not as good as those obtained with surgical removal.
Surgery for metastatic disease: If metastatic disease is present surgical treatment may still a viable option. Radical and partial nephrectomy can still occur, and in some cases, if the metastasis is small this can also be surgically removed.[9] This depends on what stage of growth and how far the disease has spread.
Percutaneous ablative therapies
Percutaneous ablation therapies use image-guidance by radiologists to treat localized tumors if a surgical procedure is not a good option. Although the use of laparoscopic surgical techniques for complete nephrectomies has reduced some of the risks associated with surgery,[79] surgery of any sort in some cases will still not be feasible. For example, the elderly, people who already have severe renal dysfunction, or people who have several comorbidities, surgery of any sort is not warranted.[80]
A probe is placed through the skin and into the tumor using real-time imaging of both the probe tip and the tumor by computed tomography, ultrasound, or even magnetic resonance imaging guidance, and then destroying the tumor with heat (radiofrequency ablation) or cold (cryotherapy). These modalities are at a disadvantage compared to traditional surgery in that pathologic confirmation of complete tumor destruction is not possible. Therefore, long-term follow-up is crucial to assess completeness of tumour ablation.[81][82] Ideally, percutaneous ablation is restricted to tumours smaller than 3.5 cm and to guide the treatment. However, there are some cases where ablation can be used on tumors that are larger.[80]
The two main types of ablation techniques that are used for renal cell carcinoma are radio frequency ablation and cryoablation.[80]
Radio frequency ablation uses an electrode probe which is inserted into the affected tissue, to send radio frequencies to the tissue to generate heat through the friction of water molecules. The heat destroys the tumor tissue.[9] Cell death will generally occur within minutes of being exposed to temperatures above 50 °C.
Cryoablation also involves the insertion of a probe into the affected area,[9] however, cold is used to kill the tumor instead of heat. The probe is cooled with chemical fluids which are very cold. The freezing temperatures cause the tumor cells to die by causing osmotic dehydration, which pulls the water out of the cell destroying the enzyme, organelles, cell membrane and freezing the cytoplasm.[80]
Targeted drugs
Cancers often grow in an unbridled fashion because they are able to evade the immune system.[8] Immunotherapy is a method that activates the person's immune system and uses it to their own advantage.[8] It was developed after observing that in some cases there was spontaneous regression.[83] Immunotherapy capitalises on this phenomenon and aims to build up a person's immune response to cancer cells.[83]
Other targeted therapy medications inhibit growth factors that have been shown to promote the growth and spread of tumours.[84][85] Most of these medications were approved within the past ten years.[86] These treatments are:[87]
- Nivolumab[88]
- Axitinib[89]
- Sunitinib[90]
- Cabozantinib[88]
- Everolimus
- Lenvatinib
- Pazopanib
- Bevacizumab
- Sorafenib
- Tivozanib
- Temsirolimus[91]
- Interleukin-2 (IL-2) has produced "durable remissions" in a small number of patients, but with substantial toxicity.[92]
- Interferon-α
For patients with metastatic cancer, sunitinib probably results in more progression of the cancer than pembrolizumab, axitinib and avelumab.[93] In comparison to pembrolizumab and axitinib, it probably results in more death, but it may slightly reduce serious unwanted effects.[93] When compared with combinations of immunotherapy (nivolumab and ipilimumab), sunitinib may lead to more progression and serious effects.[93] There may be little to no difference in progression, survival and serious effects between pazopanib and sunitib.[93]
Activity has also been reported for ipilimumab[94] but it is not an approved medication for renal cancer.[95]
More medications are expected to become available in the near future as several clinical trials are currently being conducted for new targeted treatments,[96] including: atezolizumab, varlilumab, durvalumab, avelumab, LAG525, MBG453, TRC105, and savolitinib.
Chemotherapy
Chemotherapy and radiotherapy are not as successful in the case of RCC. RCC is resistant in most cases but there is about a 4–5% success rate, but this is often short-lived with more tumours and growths developing later.[9]
Adjuvant and neoadjuvant therapy
Adjuvant therapy, which refers to therapy given after a primary surgery, has not been found to be beneficial in renal cell cancer.[97] Conversely, neoadjuvant therapy is administered before the intended primary or main treatment. In some cases neoadjuvant therapy has been shown to decrease the size and stage of the RCC to then allow it to be surgically removed.[85] This is a new form of treatment and the effectiveness of this approach is still being assessed in clinical trials.
Metastasis
Metastatic renal cell carcinoma (mRCC) is the spread of the primary renal cell carcinoma from the kidney to other organs. 25–30% of people have this metastatic spread by the time they are diagnosed with renal cell carcinoma.[98] This high proportion is explained by the fact that clinical signs are generally mild until the disease progresses to a more severe state.[99] The most common sites for metastasis are the lymph nodes, lung, bones, liver and brain.[10] How this spread affects the staging of the disease and hence prognosis is discussed in the "Diagnosis" and "Prognosis" sections.
MRCC has a poor prognosis compared to other cancers although average survival times have increased in the last few years due to treatment advances. Average survival time in 2008 for the metastatic form of the disease was under a year[100] and by 2013 this improved to an average of 22 months.[101] Despite this improvement the five-year survival rate for mRCC remains under 10%[102] and 20–25% of patients remain unresponsive to all treatments and in these cases, the disease has a rapid progression.[101]
The available treatments for RCC discussed in the "Treatment" section are also relevant for the metastatic form of the disease. Options include interleukin-2 which is a standard therapy for advanced renal cell carcinoma.[97] From 2007 to 2013, seven new treatments have been approved specifically for mRCC (sunitinib, temsirolimus, bevacizumab, sorafenib, everolimus, pazopanib and axitinib).[7] These new treatments are based on the fact that renal cell carcinomas are very vascular tumors – they contain a large number of blood vessels. The drugs aim to inhibit the growth of new blood vessels in the tumors, hence slowing growth and in some cases reducing the size of the tumors.[103] Side effects unfortunately are quite common with these treatments and include:[104]
- Gastrointestinal effects – nausea, vomiting, diarrhea, anorexia
- Respiratory effects – coughing, dyspnea (difficulty breathing)
- Cardiovascular effects – hypertension (high blood pressure)
- Neurological effects – intracranial hemorrhage (bleeding into the brain), thrombosis (blood clots) in the brain
- Effects on the skin and mucus membranes – rashes, hand-foot syndrome, stomatitis
- Bone marrow suppression – resulting in reduced white blood cells, increasing the risk of infections plus anemia and reduced platelets
- Renal effects – impaired kidney function
- Fatigue.
Radiotherapy and chemotherapy are more commonly used in the metastatic form of RCC to target the secondary tumors in the bones, liver, brain and other organs. While not curative, these treatments do provide relief for symptoms associated with the spread of tumors.[101]
Prognosis
The prognosis is influenced by several factors, including tumour size, degree of invasion and metastasis, histologic type, and nuclear grade.[24] Staging is the most important factor in the outcome of renal cell cancer. The following numbers are based on patients first diagnosed in 2001 and 2002 by the National Cancer Data Base:[105]
| Stage | Description | 5 Year Survival Rate |
|---|---|---|
| I | Confined to the kidney | 81% |
| II | Extend through the renal capsule, confined to Gerota's Fascia | 74% |
| III | Include the renal vein, or the hilar lymph nodes | 53% |
| IV | Includes tumors that are invasive to adjacent organs (except the adrenal glands), or distant metastases | 8% |
A Korean study estimated a disease-specific overall five-year survival rate of 85%.[106] Taken as a whole, if the disease is limited to the kidney, only 20–30% develop metastatic disease after nephrectomy.[107] More specific subsets show a five-year survival rate of around 90–95% for tumors less than 4 cm. For larger tumors confined to the kidney without venous invasion, survival is still relatively good at 80–85%. For tumors that extend through the renal capsule and out of the local fascial investments, the survivability reduces to near 60%. Factors as general health and fitness or the severity of their symptoms impact the survival rates. For instance, younger people (among 20–40 years old) have a better outcome despite having more symptoms at presentation, possibly due to lower rates spread of cancer to the lymph nodes (stage III).
Histological grade is related to the aggressiveness of the cancer, and it is classified in 4 grades, with 1 having the best prognosis (five-year survival over 89%), and 4 with the worst prognosis (46% of five-year survival).
Some people have the renal cell cancer detected before they have symptoms (incidentally) because of the CT scan (Computed Tomography Imaging) or ultrasound. Incidentally diagnosed renal cell cancer (no symptoms) differs in outlook from those diagnosed after presenting symptoms of renal cell carcinoma or metastasis. The five-year survival rate was higher for incidental than for symptomatic tumours: 85.3% versus 62.5%. Incidental lesions were significantly lower stage than those that cause symptoms, since 62.1% patients with incidental renal cell carcinoma were observed with Stage I lesions, against 23% were found with symptomatic renal cell carcinoma.[108]
If it has metastasized to the lymph nodes, the five-year survival is around 5% to 15%. For metastatic renal cell carcinoma, factors which may present a poor prognosis include a low Karnofsky performance-status score (a standard way of measuring functional impairment in patients with cancer), a low haemoglobin level, a high level of serum lactate dehydrogenase, and a high corrected level of serum calcium.[109][110] For non-metastatic cases, the Leibovich scoring algorithm may be used to predict post-operative disease progression.[111]
Renal cell carcinoma is one of the cancers most strongly associated with paraneoplastic syndromes, most often due to ectopic hormone production by the tumour. The treatment for these complications of RCC is generally limited beyond treating the underlying cancer.
Epidemiology
The incidence of the disease varies according to geographic, demographic and, to a lesser extent, hereditary factors. There are some known risk factors, however the significance of other potential risk factors remains more controversial. The incidence of the cancer has been increasing in frequency worldwide at a rate of approximately 2–3% per decade[100] until the last few years where the number of new cases has stabilised.[16]
The incidence of RCC varies between sexes, ages, races and geographic location around the world. Men have a higher incidence than women (approximately 1.6:1)[97] and the vast majority are diagnosed after 65 years of age.[97] Asians reportedly have a significantly lower incidence of RCC than whites and while African countries have the lowest reported incidences, African Americans have the highest incidence of the population in the United States.[16] Developed countries have a higher incidence than developing countries, with the highest rates found in North America, Europe and Australia / New Zealand.[112]
History
Daniel Sennert made the first reference suggesting a tumour arising in the kidney in his text Practicae Medicinae, first published in 1613.[113]
Miril published the earliest unequivocal case of renal carcinoma in 1810.[114] He described the case of Françoise Levelly, a 35-year-old woman, who presented to Brest Civic Hospital on April 6, 1809, supposedly in the late stages of pregnancy.[113]
Koenig published the first classification of renal tumours based on macroscopic morphology in 1826. Koenig divided the tumors into scirrhous, steatomatous, fungoid and medullary forms.[115]
Hypernephroma controversy
Following the classification of the tumour, researchers attempted to identify the tissue of origin for renal carcinoma.
The pathogenesis of renal epithelial tumours was debated for decades. The debate was initiated by Paul Grawitz when in 1883, he published his observations on the morphology of small, yellow renal tumours. Grawitz concluded that only alveolar tumours were of adrenal origin, whereas papillary tumours were derived from renal tissue.[113]
In 1893, Paul Sudeck challenged the theory postulated by Grawitz by publishing descriptions of renal tumours in which he identified atypical features within renal tubules and noted a gradation of these atypical features between the tubules and neighboring malignant tumour. In 1894, Otto Lubarsch, who supported the theory postulated by Grawitz coined the term hypernephroid tumor, which was amended to hypernephroma by Felix Victor Birch-Hirschfeld to describe these tumours.[116]
Vigorous criticism of Grawitz was provided by Oskar Stoerk in 1908, who considered the adrenal origin of renal tumours to be unproved. Despite the compelling arguments against the theory postulated by Grawitz, the term hypernephroma, with its associated adrenal connotation, persisted in the literature.[113]
Foot and Humphreys, and Foote et al. introduced the term Renal Celled Carcinoma to emphasize a renal tubular origin for these tumours. Their designation was slightly altered by Fetter to the now widely accepted term Renal Cell Carcinoma.[117]
Convincing evidence to settle the debate was offered by Oberling et al. in 1959 who studied the ultrastructure of clear cells from eight renal carcinomas. They found that the tumour cell cytoplasm contained numerous mitochondria and deposits of glycogen and fat. They identified cytoplasmic membranes inserted perpendicularly onto the basement membrane with occasional cells containing microvilli along the free borders. They concluded that these features indicated that the tumours arose from the epithelial cells of the renal convoluted tubule, thus finally settling one of the most debated issues in tumour pathology.[113][118]
See also
- Stauffer syndrome
- Knudson hypothesis[119]
- Interleukin-2
- Kidney cancer
- Rapamycin
- Vinblastine
- Dysuria
- Interferon
References
- Curti, B; Jana, BRP; Javeed, M; Makhoul, I; Sachdeva, K; Hu, W; Perry, M; Talavera, F (26 February 2014). Harris, JE (ed.). "Renal Cell Carcinoma". Medscape Reference. WebMD. Archived from the original on 7 March 2014. Retrieved 7 March 2014.
- "EAU Guidelines: Renal Cell Carcinoma". Retrieved 24 April 2020.
- Rini BI, Rathmell WK, Godley P (2008). "Renal cell carcinoma". Curr Opin Oncol. 20 (3): 300–6. doi:10.1097/CCO.0b013e3282f9782b. PMID 18391630.
- "Kidney cancer". nhs.uk. 2017-10-23. Archived from the original on 3 October 2017. Retrieved 19 March 2018.
- Fausto, V; Abbas, A; Fausto, N (2004). Robbins and Cotran Pathologic Basis of disease (7th ed.). Philadelphia, PA: Elsevier/Saunders. ISBN 978-0721601878.
- Master, VA (November 2013). "Renal Cell Carcinoma". Merck Manual Professional. Merck Sharp & Dohme Corp. Archived from the original on 7 March 2014. Retrieved 7 March 2014.
- Singer, Eric A.; Gupta, Gopal N.; Marchalik, Daniel; Srinivasan, Ramaprasad (2013). "Evolving therapeutic targets in renal cell carcinoma". Current Opinion in Oncology. 25 (3): 273–80. doi:10.1097/CCO.0b013e32835fc857. PMID 23455028. S2CID 11526724.
- Syn, Nicholas L; Teng, Michele W L; Mok, Tony S K; Soo, Ross A (2017). "De-novo and acquired resistance to immune checkpoint targeting". The Lancet Oncology. 18 (12): e731–e741. doi:10.1016/s1470-2045(17)30607-1. PMID 29208439.
- Cohen, Herbert T.; McGovern, Francis J. (2005). "Renal-Cell Carcinoma". New England Journal of Medicine. 353 (23): 2477–90. doi:10.1056/NEJMra043172. PMID 16339096.
- Motzer, Robert J.; Bander, Neil H.; Nanus, David M. (1996). "Renal-Cell Carcinoma". New England Journal of Medicine. 335 (12): 865–75. doi:10.1056/NEJM199609193351207. PMID 8778606.
- Kim, Hyung L.; Belldegrun, Arie S.; Freitas, Danielo G.; Bui, Matthew H.T.; Han, KEN-RYU; Dorey, Frederick J.; Figlin, Robert A. (2003). "Paraneoplastic Signs and Symptoms of Renal Cell Carcinoma: Implications for Prognosis". The Journal of Urology. 170 (5): 1742–6. doi:10.1097/01.ju.0000092764.81308.6a. PMID 14532767.
- Birkhauser; Kroeger, Pantuck (2013). "Etiology of Renal Cell Carcinoma: Incidence, Demographics, and Environmental Factors". Renal Cell Carcinoma Clinical Management. Humana Pr Inc. pp. 3–22. ISBN 978-1-62703-061-8.
- Lane, Brian R. (2013). "Prognostic Factors for Localized Renal Cell Carcinoma". Renal Cell Carcinoma. pp. 83–102. doi:10.1007/978-1-62703-062-5_5. ISBN 978-1-62703-061-8.
- Metz; Davis (2013). "Palliative and Supportive Care for Renal Cancer". Renal Cell Carcinoma Clinical Management. Humana. pp. 339–348. ISBN 978-1-62703-061-8.
- Häggström, Christel; Rapp, Kilian; Stocks, Tanja; Manjer, Jonas; Bjørge, Tone; Ulmer, Hanno; Engeland, Anders; Almqvist, Martin; Concin, Hans; Selmer, R; Ljungberg, B; Tretli, S; Nagel, G; Hallmans, G; Jonsson, H; Stattin, P (2013). Miller, Todd W (ed.). "Metabolic Factors Associated with Risk of Renal Cell Carcinoma". PLOS ONE. 8 (2): e57475. Bibcode:2013PLoSO...857475H. doi:10.1371/journal.pone.0057475. PMC 3585341. PMID 23468995.
- Ljungberg, Börje; Campbell, Steven C.; Choi, Han Yong; Jacqmin, Didier; Lee, Jung Eun; Weikert, Steffen; Kiemeney, Lambertus A. (2011). "The Epidemiology of Renal Cell Carcinoma". European Urology. 60 (4): 615–21. doi:10.1016/j.eururo.2011.06.049. PMID 21741761.
- Dhôte, R.; Pellicer-Coeuret, M.; Thiounn, N.; Debré, B.; Vidal-Trecan, G. (2007). "Risk factors for adult renal cell carcinoma: A systematic review and implications for prevention". BJU International. 86 (1): 20–7. doi:10.1046/j.1464-410x.2000.00708.x. PMID 10886077. S2CID 21271953.
- Boffetta, P.; Fontana, L.; Stewart, P.; Zaridze, D.; Szeszenia-Dabrowska, N.; Janout, V.; Bencko, V.; Foretova, L.; Jinga, V.; Matveev, V.; Kollarova, H.; Ferro, G.; Chow, W.-H.; Rothman, N.; Van Bemmel, D.; Karami, S.; Brennan, P.; Moore, L. E. (2011). "Occupational exposure to arsenic, cadmium, chromium, lead and nickel, and renal cell carcinoma: A case-control study from Central and Eastern Europe". Occupational and Environmental Medicine. 68 (10): 723–8. doi:10.1136/oem.2010.056341. hdl:11585/682305. PMID 21217163. S2CID 29328889.
- Cho, Eunyoung; Curhan, G; Hankinson, SE; Kantoff, P; Atkins, MB; Stampfer, M; Choueiri, TK (2011). "Prospective Evaluation of Analgesic Use and Risk of Renal Cell Cancer". Archives of Internal Medicine. 171 (16): 1487–93. doi:10.1001/archinternmed.2011.356. PMC 3691864. PMID 21911634.
- Zucchetto, Antonella; Talamini, Renato; Dal Maso, Luigino; Negri, Eva; Polesel, Jerry; Ramazzotti, Valerio; Montella, Maurizio; Canzonieri, Vincenzo; Serraino, Diego; La Vecchia, Carlo; Franceschi, Silvia (2008). "Reproductive, menstrual, and other hormone-related factors and risk of renal cell cancer". International Journal of Cancer. 123 (9): 2213–6. doi:10.1002/ijc.23750. PMID 18711701.
- Bellocco, R.; Pasquali, E.; Rota, M.; Bagnardi, V.; Tramacere, I.; Scotti, L.; Pelucchi, C.; Boffetta, P.; Corrao, G. (2012-09-01). "Alcohol drinking and risk of renal cell carcinoma: results of a meta-analysis". Annals of Oncology. 23 (9): 2235–2244. doi:10.1093/annonc/mds022. ISSN 1569-8041. PMID 22398178.
- Lipworth, L; Tarone, RE; Lund, L; McLaughlin, JK (2009). "Epidemiologic characteristics and risk factors for renal cell cancer". Clinical Epidemiology. 1: 33–43. doi:10.2147/clep.s4759. PMC 2943168. PMID 20865085.
- Pavlovich, Christian P.; Schmidt, Laura S. (2004). "Searching for the hereditary causes of renal-cell carcinoma". Nature Reviews Cancer. 4 (5): 381–93. doi:10.1038/nrc1364. PMID 15122209. S2CID 17905393.
- Rini, Brian I; Campbell, Steven C; Escudier, Bernard (2009). "Renal cell carcinoma". The Lancet. 373 (9669): 1119–1132. doi:10.1016/S0140-6736(09)60229-4. PMID 19269025. S2CID 24535138.
- Baldewijns, Marcella M.L.; Van Vlodrop, Iris J.H.; Schouten, Leo J.; Soetekouw, Patricia M.M.B.; De Bruïne, Adriaan P.; Van Engeland, Manon (2008). "Genetics and epigenetics of renal cell cancer". Biochimica et Biophysica Acta (BBA) - Reviews on Cancer. 1785 (2): 133–155. doi:10.1016/j.bbcan.2007.12.002. PMID 18187049.
- Tjaden, Christin; Werner, Jens; Buechler, Markus W.; Hackert, Thilo (2011). "Reactive Hypertrophy of an Accessory Spleen Mimicking Tumour Recurrence of Metastatic Renal Cell Carcinoma". Asian Journal of Surgery. 34 (1): 50–2. doi:10.1016/S1015-9584(11)60019-5. PMID 21515214.
- Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 978-0-7817-7153-5.
- Catto, James W.F.; Shariat, Shahrokh F. (2013). "The Changing Face of Renal Cell Carcinoma: The Impact of Systematic Genetic Sequencing on Our Understanding of This Tumor's Biology". European Urology. 63 (5): 855–7, discussion 857–8. doi:10.1016/j.eururo.2012.09.049. PMID 23026395.
- Zhou, Ming; He, Huiying (2013). "Pathology of Renal Cell Carcinoma". Renal Cell Carcinoma. pp. 23–41. doi:10.1007/978-1-62703-062-5_2. ISBN 978-1-62703-061-8. S2CID 2101851.
- Robbins and Cotran pathologic basis of disease (Ninth ed.). Elsevier. 2015. p. 954. ISBN 9780808924500.
- Kumar, Vinay; Abbas, Abul K.; Aster, Jon C. (2015). Robbins and Cotran pathologic basis of disease (Ninth ed.). p. 954. ISBN 9780808924500.
- Lopez-Beltran, Antonio; Scarpelli, Marina; Montironi, Rodolfo; Kirkali, Ziya (2006). "2004 WHO Classification of the Renal Tumors of the Adults". European Urology. 49 (5): 798–805. doi:10.1016/j.eururo.2005.11.035. PMID 16442207.
- Hagenkord, Jill M; Parwani, Anil V; Lyons-Weiler, Maureen A; Alvarez, Karla; Amato, Robert; Gatalica, Zoran; Gonzalez-Berjon, Jose M; Peterson, Leif; Dhir, Rajiv; Monzon, Federico A (2008). "Virtual karyotyping with SNP microarrays reduces uncertainty in the diagnosis of renal epithelial tumors". Diagnostic Pathology. 3: 44. doi:10.1186/1746-1596-3-44. PMC 2588560. PMID 18990225.
- Monzon, Federico A; Hagenkord, Jill M; Lyons-Weiler, Maureen A; Balani, Jyoti P; Parwani, Anil V; Sciulli, Christin M; Li, Jia; Chandran, Uma R; Bastacky, Sheldon I; Dhir, Rajiv (2008). "Whole genome SNP arrays as a potential diagnostic tool for the detection of characteristic chromosomal aberrations in renal epithelial tumors". Modern Pathology. 21 (5): 599–608. doi:10.1038/modpathol.2008.20. PMID 18246049.
- Lyons-Weiler M, Hagenkord J, Sciulli C, Dhir R, Monzon FA (2008). "Optimization of the Affymetrix GeneChip Mapping 10K 2.0 Assay for routine clinical use on formalin-fixed paraffin-embedded tissues". Diagn. Mol. Pathol. 17 (1): 3–13. doi:10.1097/PDM.0b013e31815aca30. PMID 18303412. S2CID 24420204.
- Crumley, S. M.; Divatia, M; Truong, L; Shen, S; Ayala, A. G.; Ro, J. Y. (2013). "Renal cell carcinoma: Evolving and emerging subtypes". World Journal of Clinical Cases. 1 (9): 262–275. doi:10.12998/wjcc.v1.i9.262. PMC 3868710. PMID 24364021.
- Rohan, S. M.; Xiao, Y; Liang, Y; Dudas, M. E.; Al-Ahmadie, H. A.; Fine, S. W.; Gopalan, A; Reuter, V. E.; Rosenblum, M. K.; Russo, P; Tickoo, S. K. (2011). "Clear-cell papillary renal cell carcinoma: Molecular and immunohistochemical analysis with emphasis on the von Hippel-Lindau gene and hypoxia-inducible factor pathway-related proteins". Modern Pathology. 24 (9): 1207–20. doi:10.1038/modpathol.2011.80. PMID 21602815.
- Wood, Laura S. (30 November 2009). "Renal Cell Carcinoma". Clinical Journal of Oncology Nursing. 13: 3–7. doi:10.1188/09.CJON.S2.3-7. PMID 19948453.
- Bonn, Dorothy (31 Jan 2004). "Urine test for renal-cell carcinoma". The Lancet Oncology. 5 (2): 72. doi:10.1016/S1470-2045(04)01368-3. PMID 14974475.
- Johann, Donald J.; Wei, Bih-Rong; Prieto, Darue A.; Chan, King C.; Ye, Xiaying; Valera, Vladimir A.; Simpson, R. Mark; Rudnick, Paul A.; Xiao, Zhen; Issaq, Haleem J.; Linehan, W. Marston; Stein, Stephen E.; Veenstra, Timothy D.; Blonder, Josip (2010). "Combined Blood/Tissue Analysis for Cancer Biomarker Discovery: Application to Renal Cell Carcinoma". Analytical Chemistry. 82 (5): 1584–8. doi:10.1021/ac902204k. PMC 3251958. PMID 20121140.
- Hatzaras, Ioannis; Gleisner, Ana L.; Pulitano, Carlo; Sandroussi, Charbel; Hirose, Kenzo; Hyder, Omar; Wolfgang, Christopher L.; Aldrighetti, Luca; Crawford, Michael; Choti, Michael A.; Pawlik, Timothy M. (2012). "A multi-institution analysis of outcomes of liver-directed surgery for metastatic renal cell cancer". HPB. 14 (8): 532–8. doi:10.1111/j.1477-2574.2012.00495.x. PMC 3406350. PMID 22762401.
- Motzer, RJ (Apr 1, 2003). "Renal cell carcinoma: a priority malignancy for development and study of novel therapies". Journal of Clinical Oncology. 21 (7): 1193–4. doi:10.1200/JCO.2003.12.072. PMID 12663704.
- Sahni, V.A. (1 January 2009). "REVIEW: Biopsy of renal masses: when and why". Cancer Imaging. 9 (1): 44–55. doi:10.1102/1470-7330.2009.0005. PMC 2739685. PMID 19602467.
- Nakada, G; Machida, T; Masuda, F; Onishi, T; Yamazaki, H; Kiyota, H; Suzuki, M; Goto, H (1983). "A case of arteriovenous fistulae secondary to renal cell carcinoma accompanied by congestive heart failure". Hinyokika Kiyo. Acta Urologica Japonica. 29 (8): 901–5. PMID 6675440.
- Pattamapaspong, Nuttaya; Muttarak, Malai; Sivasomboon, Chate (2011). "Tuberculosis Arthritis and Tenosynovitis". Seminars in Musculoskeletal Radiology. 15 (5): 459–69. doi:10.1055/s-0031-1293492. PMID 22081281.
- Israel, Gary M.; Bosniak, Morton A. (2005). "How I Do It: Evaluating Renal Masses1". Radiology. 236 (2): 441–50. doi:10.1148/radiol.2362040218. PMID 16040900. S2CID 1916092.
- Jubelirer, SJ; Rubin, M (1993). "The use of modern radiologic methods in identifying incidental renal cell carcinoma". The West Virginia Medical Journal. 89 (1): 21–3. PMID 8421912.
- Beck, AD (Oct 1997). "Renal cell carcinoma involving the inferior vena cava: radiologic evaluation and surgical management". The Journal of Urology. 118 (4): 533–7. doi:10.1016/S0022-5347(17)58098-2. PMID 916043.
- Sauk, Steven C.; Hsu, Margaret S.; Margolis, Daniel J. A.; Lu, David S. K.; Rao, Nagesh P.; Belldegrun, Arie S.; Pantuck, Allan J.; Raman, Steven S. (2011). "Clear Cell Renal Cell Carcinoma: Multiphasic Multidetector CT Imaging Features Help Predict Genetic Karyotypes". Radiology. 261 (3): 854–62. doi:10.1148/radiol.11101508. PMID 22025734.
- Lane, Brian R.; Samplaski, Mary K.; Herts, Brian R.; Zhou, Ming; Novick, Andrew C.; Campbell, Steven C. (2008). "Renal Mass Biopsy—A Renaissance?". The Journal of Urology. 179 (1): 20–7. doi:10.1016/j.juro.2007.08.124. PMID 17997455.
- Hricak, H; Demas, BE; Williams, RD; McNamara, MT; Hedgcock, MW; Amparo, EG; Tanagho, EA (1985). "Magnetic resonance imaging in the diagnosis and staging of renal and perirenal neoplasms". Radiology. 154 (3): 709–15. doi:10.1148/radiology.154.3.3969475. PMID 3969475.
- Janus, CL; Mendelson, DS (1991). "Comparison of MRI and CT for study of renal and perirenal masses". Critical Reviews in Diagnostic Imaging. 32 (2): 69–118. PMID 1863349.
- Nishimura, Kazuo; Hida, Shuichi; Okada, Kenichiro; Yoshida, Osamu; Nishimuara, Kazumasa (1988). "Staging and differential diagnosis of renal cell carcinoma: A comparison of magnetic resonance imaging (MRI) and computed tomography (CT)". Acta Urologica Japonica. 34 (8): 1323–31. hdl:2433/119684. PMID 3195400.
- Reznek, RH (Feb 14, 2004). "CT/MRI in staging renal cell carcinoma". Cancer Imaging. 4 Spec No A (Spec No A): S25–32. doi:10.1102/1470-7330.2004.0012. PMC 1435344. PMID 18215972.
- Kocak, Mehmet; Sudakoff, Gary S.; Erickson, Scott; Begun, Frank; Datta, Milton (2001). "Using MR Angiography for Surgical Planning in Pelvic Kidney Renal Cell Carcinoma". American Journal of Roentgenology. 177 (3): 659–60. doi:10.2214/ajr.177.3.1770659. PMID 11517066.
- Kidney Cancer / General Information Archived 2011-11-01 at the Wayback Machine at Weill Cornell Medical College, James Buchanan Brady Foundation, Department of Urology
- Oto, A; Herts, B R; Remer, E M; Novick, A C (1998). "Inferior vena cava tumor thrombus in renal cell carcinoma: Staging by MR imaging and impact on surgical treatment". American Journal of Roentgenology. 171 (6): 1619–24. doi:10.2214/ajr.171.6.9843299. PMID 9843299.
- "Clear-cell Carcinoma, Hypernephroid Tumour, or Hypernephroma". Archived from the original on 2010-05-07. Retrieved 2010-03-31.
- Vasil'Eva, NN; Koriakina, RF (1976). "Morphological diagnosis of renal cell carcinoma. Histo-cytological parallels". Arkhiv Patologii. 38 (12): 12–7. PMID 1016084.
- "Renal clear cell carcinoma (Grawitz tumor)". Atlas of Pathology. January 30, 2009. Archived from the original on March 10, 2009.
- López, JI (Mar 2013). "Renal tumors with clear cells. A review". Pathology, Research and Practice. 209 (3): 137–46. doi:10.1016/j.prp.2013.01.007. PMID 23433880.
- Rioux-Leclercq, Nathalie (November 2006). "Le grade nucléaire de fuhrman, facteur pronostique du cancer du rein depuis 25 ans" [The Fuhrman grading system for kidney cancer prognosis]. Progrès en Urologie (in French). 16 (4): 5–8. PMID 17183964. INIST:18271804.
- Delahunt, Brett; Sika-Paotonu, Dianne; Bethwaite, Peter B.; McCredie, Margaret R. E.; Martignoni, Guido; Eble, John N.; Jordan, T. (2007). "Fuhrman Grading is not Appropriate for Chromophobe Renal Cell Carcinoma". The American Journal of Surgical Pathology. 31 (6): 957–60. doi:10.1097/01.pas.0000249446.28713.53. PMID 17527087. S2CID 27154220.
- Kovacs, Gyula; Akhtar, Mohammed; Beckwith, Bruce J.; Bugert, Peter; Cooper, Colin S.; Delahunt, Brett; Eble, John N.; Fleming, Stewart; Ljungberg, Börje; Medeiros, L. Jeffrey; Moch, Holger; Reuter, Victor E.; Ritz, Eberhard; Roos, Göran; Schmidt, Dietmar; Srigley, John R.; Störkel, Stephan; Van Den Berg, Eva; Zbar, Bert (1997). "The Heidelberg classification of renal cell tumours". The Journal of Pathology. 183 (2): 131–3. doi:10.1002/(SICI)1096-9896(199710)183:2<131::AID-PATH931>3.0.CO;2-G. PMID 9390023. S2CID 34796951.
- Lauby-Secretan, B; Scoccianti, C; Loomis, D; Grosse, Y; Bianchini, F; Straif, K; International Agency for Research on Cancer Handbook Working, Group (25 August 2016). "Body Fatness and Cancer—Viewpoint of the IARC Working Group". The New England Journal of Medicine. 375 (8): 794–798. doi:10.1056/nejmsr1606602. PMC 6754861. PMID 27557308.
- Simmons; Campbell (2012-09-26). "Assessment of Oncologic Risk for Clinical Stage T1 Renal Tumours". Renal Cell Carcinoma Clinical Management. Humana Pr Inc. pp. 105–118. ISBN 978-1-62703-061-8.
- Smaldone, Marc C.; Canter, Daniel; Kutikov, Alexander; Uzzo, Robert G. (2013). "Active Surveillance of the Small Renal Mass". Renal Cell Carcinoma. pp. 167–94. doi:10.1007/978-1-62703-062-5_10. ISBN 978-1-62703-061-8.
- Novick AC (September 1998). "Nephron-sparing surgery for renal cell carcinoma". Br J Urol. 82 (3): 321–4. doi:10.1046/j.1464-410X.1998.00751.x. PMID 9772865.
- Herr HW (January 1999). "Partial nephrectomy for unilateral renal carcinoma and a normal contralateral kidney: 10-year followup". J. Urol. 161 (1): 33–4, discussion 34–5. doi:10.1016/S0022-5347(01)62052-4. PMID 10037361.
- Van Poppel H, Bamelis B, Oyen R, Baert L (September 1998). "Partial nephrectomy for renal cell carcinoma can achieve long-term tumor control". J. Urol. 160 (3 Pt 1): 674–8. doi:10.1016/S0022-5347(01)62751-4. PMID 9720519.
- Mattar K, Jewett MA (January 2008). "Watchful waiting for small renal masses". Curr Urol Rep. 9 (1): 22–5. doi:10.1007/s11934-008-0006-3. PMID 18366970. S2CID 26763264.
- Weight, Christopher J.; Larson, Benjamin T.; Fergany, Amr F.; Gao, Tianming; Lane, Brian R.; Campbell, Steven C.; Kaouk, Jihad H.; Klein, Eric A.; Novick, Andrew C. (2010). "Nephrectomy Induced Chronic Renal Insufficiency is Associated with Increased Risk of Cardiovascular Death and Death from Any Cause in Patients with Localized cT1b Renal Masses". The Journal of Urology. 183 (4): 1317–23. doi:10.1016/j.juro.2009.12.030. PMID 20171688.
- Weight, Christopher J.; Crispen, Paul L.; Breau, Rodney H.; Kim, Simon P.; Lohse, Christine M.; Boorjian, Stephen A.; Thompson, R. Houston; Leibovich, Bradley C. (2013). "Practice-setting and surgeon characteristics heavily influence the decision to perform partial nephrectomy among American Urologic Association surgeons". BJU International. 111 (5): 731–8. doi:10.1111/j.1464-410X.2012.11112.x. PMID 22502641. S2CID 829345.
- Casey, R.G.; Raheem, O.A.; Elmusharaf, E.; Madhavan, P.; Tolan, M.; Lynch, T.H. (2013). "Renal cell carcinoma with IVC and atrial thrombus: A single centre's 10 year surgical experience". The Surgeon. 11 (6): 295–9. doi:10.1016/j.surge.2013.02.007. PMID 23510704.
- Ciancio, Gaetano; Livingstone, Alan S.; Soloway, Mark (2007). "Surgical Management of Renal Cell Carcinoma with Tumor Thrombus in the Renal and Inferior Vena Cava: The University of Miami Experience in Using Liver Transplantation Techniques". European Urology. Elsevier BV. 51 (4): 988–995. doi:10.1016/j.eururo.2006.11.055. ISSN 0302-2838. PMID 17175095.
- Ciancio, Gaetano; Soloway, Mark S. (2005). "Renal cell carcinoma with tumor thrombus extending above diaphragm: Avoiding cardiopulmonary bypass". Urology. Elsevier BV. 66 (2): 266–270. doi:10.1016/j.urology.2005.03.039. ISSN 0090-4295. PMID 16098354.
- Flanigan RC, Mickisch G, Sylvester R, Tangen C, Van Poppel H, Crawford ED (March 2004). "Cytoreductive nephrectomy in patients with metastatic renal cancer: a combined analysis". J. Urol. 171 (3): 1071–6. CiteSeerX 10.1.1.469.2497. doi:10.1097/01.ju.0000110610.61545.ae. PMID 14767273.
- Mulders PF, Brouwers AH, Hulsbergen-van der Kaa CA, van Lin EN, Osanto S, de Mulder PH (February 2008). "[Guideline 'Renal cell carcinoma']". Nederlands Tijdschrift voor Geneeskunde (in Dutch). 152 (7): 376–80. PMID 18380384.
- Russo (2013). "Radical Nephrectomy for Localised Renal Tumours: Oncological and Renal Functional Considerations". Renal Cell Carcinoma Clinical Management. Humana Pr Inc. pp. 119–132. ISBN 978-1-62703-061-8.
- Matin; Ahrar (2013). "Thermal Ablation". Renal Cell Carcinoma Clinical Management. Humana. pp. 155–166. ISBN 978-1-62703-061-8.
- Mogami T, Harada J, Kishimoto K, Sumida S (April 2007). "Percutaneous MR-guided cryoablation for malignancies, with a focus on renal cell carcinoma". Int. J. Clin. Oncol. 12 (2): 79–84. doi:10.1007/s10147-006-0654-6. PMID 17443274. S2CID 5743758.
- Boss A, Clasen S, Kuczyk M, Schick F, Pereira PL (March 2007). "Image-guided radiofrequency ablation of renal cell carcinoma". Eur Radiol. 17 (3): 725–33. doi:10.1007/s00330-006-0415-y. PMID 17021704. S2CID 12651841.
- Davar; Fenton; Appleman (2013). "Immunotherapy for Renal Cell Carcinoma". Renal Cell Carcinoma Clinical Management. Humana. pp. 279–302. ISBN 978-1-62703-061-8.
- Santoni, M; De Tursi, M; Felici, A; Lo Re, G; Ricotta, R; Ruggeri, EM; Sabbatini, R; Santini, D; Vaccaro, V; Milella, M (June 2013). "Management of metastatic renal cell carcinoma patients with poor-risk features: current status and future perspectives". Expert Review of Anticancer Therapy. 13 (6): 697–709. doi:10.1586/era.13.52. PMID 23773104. S2CID 36871651.
- Stroup (2013). "Neoadjuvant Targeted Therapy and Consolidative Surgery". Renal Cell Carcinoma Clinical Management. Humana. pp. 219–230. ISBN 978-1-62703-061-8.
- Shoji, S; Nakano, M; Sato, H; Tang, XY; Osamura, YR; Terachi, T; Uchida, T; Takeya, K (January 2014). "The current status of tailor-made medicine with molecular biomarkers for patients with clear cell renal cell carcinoma". Clinical & Experimental Metastasis. 31 (1): 111–34. doi:10.1007/s10585-013-9612-7. PMID 23959576. S2CID 15100003.
- Jonasch, E; Futreal, PA; Davis, IJ; Bailey, ST; Kim, WY; Brugarolas, J; Giaccia, AJ; Kurban, G; Pause, A; Frydman, J; Zurita, AJ; Rini, BI; Sharma, P; Atkins, MB; Walker, CL; Rathmell, WK (July 2012). "State of the science: an update on renal cell carcinoma". Molecular Cancer Research. 10 (7): 859–80. doi:10.1158/1541-7786.MCR-12-0117. PMC 3399969. PMID 22638109.
- Quinn DI, Lara PN (2015). "Renal-Cell Cancer – Targeting an Immune Checkpoint or Multiple Kinases". N. Engl. J. Med. 373 (19): 1872–4. doi:10.1056/NEJMe1511252. PMC 7526749. PMID 26406149.
- Dranitsaris, G; Schmitz, S; Broom, RJ (November 2013). "Small molecule targeted therapies for the second-line treatment for metastatic renal cell carcinoma: a systematic review and indirect comparison of safety and efficacy". Journal of Cancer Research and Clinical Oncology. 139 (11): 1917–26. doi:10.1007/s00432-013-1510-5. PMID 24037486. S2CID 27524034.
- Motzer, Robert J.; Hutson, Thomas E.; Tomczak, Piotr; Michaelson, M. Dror; Bukowski, Ronald M.; Rixe, Olivier; Oudard, Stéphane; Negrier, Sylvie; Szczylik, Cezary; Kim, Sindy T.; Chen, Isan; Bycott, Paul W.; Baum, Charles M.; Figlin, Robert A. (2007). "Sunitinib versus Interferon Alfa in Metastatic Renal-Cell Carcinoma". New England Journal of Medicine. 356 (2): 115–124. doi:10.1056/NEJMoa065044. ISSN 0028-4793. PMID 17215529.
- "TORISEL® (temsirolimus) -Safety Info- Renal Cell Carcinoma Treatment". www.torisel.com. Archived from the original on 13 April 2018. Retrieved 19 March 2018.
- Renal Cell Carcinoma Archived 2016-07-05 at the Wayback Machine MedlinePlus Medical Encyclopedia. Retrieved on 2010-09-10
- Hofmann, Fabian; Hwang, Eu Chang; Lam, Thomas BL; Bex, Axel; Yuan, Yuhong; Marconi, Lorenzo SO; Ljungberg, Börje (2020-10-14). "Targeted therapy for metastatic renal cell carcinoma". Cochrane Database of Systematic Reviews. 2020 (10): CD012796. doi:10.1002/14651858.cd012796.pub2. hdl:2164/11109. ISSN 1465-1858. PMC 8094280. PMID 33058158.
- Yang JC, Hughes M, Kammula U, Royal R, Sherry RM, Topalian SL, Suri KB, Levy C, Allen T, Mavroukakis S, Lowy I, White DE, Rosenberg SA (2007). "Ipilimumab (anti-CTLA4 antibody) causes regression of metastatic renal cell cancer associated with enteritis and hypophysitis". J. Immunother. 30 (8): 825–30. doi:10.1097/CJI.0b013e318156e47e. PMC 2134980. PMID 18049334.
- "Archived copy" (PDF). Archived (PDF) from the original on 2015-02-06. Retrieved 2014-10-29.
{{cite web}}: CS1 maint: archived copy as title (link) - "Kidney Cancer". Cancer Research Institute. Archived from the original on 24 December 2017. Retrieved 19 March 2018.
- Cohen, Herbert T.; McGovern, Francis J. (2005). "Renal-Cell Carcinoma". New England Journal of Medicine. 353 (23): 2477–90. doi:10.1056/NEJMra043172. PMID 16339096.
- Lam, John S.; Leppert, John T.; Belldegrun, Arie S.; Figlin, Robert A. (2005). "Novel approaches in the therapy of metastatic renal cell carcinoma". World Journal of Urology. 23 (3): 202–12. doi:10.1007/s00345-004-0466-0. PMID 15812574. S2CID 12091991.
- Ljungberg, Börje; Hanbury, Damian C.; Kuczyk, Marcus A.; Merseburger, Axel S.; Mulders, Peter F.A.; Patard, Jean-Jacques; Sinescu, Ioanel C.; European Association of Urology Guideline Group for renal cell carcinoma (2007). "Renal Cell Carcinoma Guideline". European Urology. 51 (6): 1502–10. doi:10.1016/j.eururo.2007.03.035. PMID 17408850.
- Gupta, Kiran; Miller, Jeffrey D.; Li, Jim Z.; Russell, Mason W.; Charbonneau, Claudie (2008). "Epidemiologic and socioeconomic burden of metastatic renal cell carcinoma (mRCC): A literature review". Cancer Treatment Reviews. 34 (3): 193–205. doi:10.1016/j.ctrv.2007.12.001. PMID 18313224.
- Buti, Sebastiano; Bersanelli, Melissa; Sikokis, Angelica; Maines, Francesca; Facchinetti, Francesco; Bria, Emilio; Ardizzoni, Andrea; Tortora, Giampaolo; Massari, Francesco (2013). "Chemotherapy in metastatic renal cell carcinoma today? A systematic review". Anti-Cancer Drugs. 24 (6): 535–54. doi:10.1097/CAD.0b013e3283609ec1. PMID 23552469. S2CID 205529087.
- Patil, Sujata; Manola, Judith; Elson, Paul; Negrier, Sylvie; Escudier, Bernard; Eisen, Tim; Atkins, Michael; Bukowski, Ronald; Motzer, Robert J. (2012). "Improvement in Overall Survival of Patients with Advanced Renal Cell Carcinoma: Prognostic Factor Trend Analysis from an International Data Set of Clinical Trials". The Journal of Urology. 188 (6): 2095–100. doi:10.1016/j.juro.2012.08.026. PMID 23083849.
- Calvo, Emiliano; Ravaud, Alain; Bellmunt, Joaquim (2013). "What is the optimal therapy for patients with metastatic renal cell carcinoma who progress on an initial VEGFr-TKI?". Cancer Treatment Reviews. 39 (4): 366–74. doi:10.1016/j.ctrv.2012.06.010. PMID 22832091.
- Alasker, Ahmed; Meskawi, Malek; Sun, Maxine; Ismail, Salima; Hanna, Nawar; Hansen, Jens; Tian, Zhe; Bianchi, Marco; Perrotte, Paul; Karakiewicz, Pierre I. (2013). "A contemporary update on rates and management of toxicities of targeted therapies for metastatic renal cell carcinoma". Cancer Treatment Reviews. 39 (4): 388–401. doi:10.1016/j.ctrv.2012.12.006. PMID 23317510.
- Kidney Cancer (Adult) – Renal Cell Carcinoma Archived 2016-04-05 at the Wayback Machine American Cancer Society. Retrieved on 2010-09-10
- "IN THIS ISSUE". Japanese Journal of Clinical Oncology. 41 (1): NP. 2010. doi:10.1093/jjco/hyq238. ISSN 0368-2811.
- Archived 2015-12-05 at the Wayback Machine Renal Cancer Causes, Symptoms, Treatment. eMedicine Health. Retrieved on 2010-09-10
- Tsui KH, Shvarts O, Smith RB, Figlin R, de Kernion JB, Belldegrun A (February 2000). "Renal cell carcinoma: prognostic significance of incidentally detected tumors". The Journal of Urology. 163 (2): 426–30. doi:10.1016/s0022-5347(05)67892-5. PMID 10647646.
- Motzer, R. J.; Bacik, J; Schwartz, LH; Reuter, V; Russo, P; Marion, S; Mazumdar, M (2003). "Prognostic Factors for Survival in Previously Treated Patients with Metastatic Renal Cell Carcinoma". Journal of Clinical Oncology. 22 (3): 454–63. doi:10.1200/JCO.2004.06.132. PMID 14752067.
- Motzer, RJ; Mazumdar, M; Bacik, J; Berg, W; Amsterdam, A; Ferrara, J (1999). "Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma". Journal of Clinical Oncology. 17 (8): 2530–40. doi:10.1200/jco.1999.17.8.2530. PMID 10561319.
- Leibovich, Bradley C.; Blute, Michael L.; Cheville, John C.; Lohse, Christine M.; Frank, Igor; Kwon, Eugene D.; Weaver, Amy L.; Parker, Alexander S.; Zincke, Horst (2003). "Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma". Cancer. 97 (7): 1663–71. doi:10.1002/cncr.11234. PMID 12655523.
- Birkhäuser, Frédéric D.; Kroeger, Nils; Pantuck, Allan J. (2013). "Etiology of Renal Cell Carcinoma: Incidence, Demographics, and Environmental Factors". Renal Cell Carcinoma. pp. 3–22. doi:10.1007/978-1-62703-062-5_1. ISBN 978-1-62703-061-8.
- Delahunt, Brett (March 8, 2009). "History of Renal Neoplasia" (PDF). United States and Canadian Academy of Pathology 2009 Annual Meeting. Archived from the original (PDF) on March 29, 2020. Retrieved April 27, 2013.
- Delahunt, Brett; Thornton A (1996). "Renal cell carcinoma. A historical perspective". J Urol Pathol. 4: 31–49.
- Delahunt, Brett; Eble, John N. (2005). "History of the Development of the Classification of Renal Cell Neoplasia". Clinics in Laboratory Medicine. 25 (2): 231–46, v. doi:10.1016/j.cll.2005.01.007. PMID 15848734.
- Judd, E. Starr (1929). "Carcinoma of the Renal Cortex with Factors Bearing on Prognosis". Archives of Internal Medicine. 44 (5): 746. doi:10.1001/archinte.1929.00140050123011.
- Foot, NC; Humphreys, GA; Whitmore, WF (1951). "Renal tumors: Pathology and prognosis in 295 cases". The Journal of Urology. 66 (2): 190–200. doi:10.1016/S0022-5347(17)74326-1. PMID 14861941.
- Oberling, CH.; Rivière, M.; Haguenau, FR. (1960). "Ultrastructure of the Clear Cells in Renal Carcinomas and its Importance for the Demonstration of their Renal Origin". Nature. 186 (4722): 402–403. Bibcode:1960Natur.186..402O. doi:10.1038/186402a0. PMID 14428164. S2CID 4224899.
- Valladares Ayerbes, Manuel; Aparicio Gallego, Guadalupe; Díaz Prado, Silvia; Jiménez Fonseca, Paula; García Campelo, Rosario; Antón Aparicio, Luis Miguel (2008). "Origin of renal cell carcinomas". Clinical and Translational Oncology. 10 (11): 697–712. doi:10.1007/s12094-008-0276-8. hdl:2183/19413. PMID 19015066.