

Slide Set C: Painting the Picture: A Reality Check
 ShareCompartir
ShareCompartir
This website is archived for historical purposes and is no longer being maintained or updated.
Download the complete slide set:
- 32 Slides in Adobe PDF Format - [4MB]
- 32 Slides in PowerPoint PPT Format - [83KB]
- 32 Slides in Adobe Flash Format - [35KB]

While the content is in the public domain and no copyright restriction applies, we do ask that users preserve the slides in their current format and cite CDC as the source.
Slide 1
External Consultation on Program Collaboration and Service Integration
PDF File or PPT File
Slide 2
A “Glimpse” Into Local Public Health Practice
PDF File or PPT File
Slide 3
THREE PICTURES
PDF File or PPT File
Slide 4
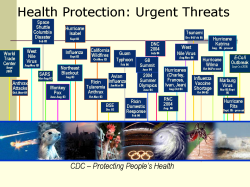
Health Protection: Urgent Threats
PDF File or PPT File
Slide 5
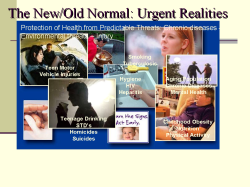
The New/Old Normal: Urgent Realities
PDF File or PPT File
Slide 6
The first 'unknown' to you
PDF File or PPT File
Slide 7
Raphael, age 10, 4th Grade
PDF File or PPT File
Slide 8
Renaldo, age 11, 6th grade
PDF File or PPT File
Slide 9
Amanda, age 8
PDF File or PPT File
Slide 10
Christopher, age 12, 5th grade
PDF File or PPT File
Slide 11
Kenny, age 12, 4th grade
PDF File or PPT File
Slide 12
Thomas, Kindergarten
PDF File or PPT File
Slide 13
Courtney, age 5, Kindergarten
PDF File or PPT File

Slide 14
Keisha, age 6, 1st grade
PDF File or PPT File
Slide 15
Jarvis
PDF File or PPT File
Slide 16
Jackie, age 12, 4th grade
PDF File or PPT File
Slide 17
Social Costs of This Disparity
PDF File or PPT File
Slide 18
The second "unknown" picture to you
PDF File or PPT File
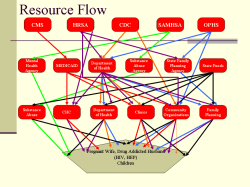
Slide 19
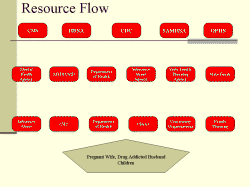
Resource Flow
PDF File or PPT File
Slide 20
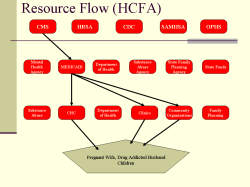
Resource Flow (HCFA)
PDF File or PPT File
Slide 21
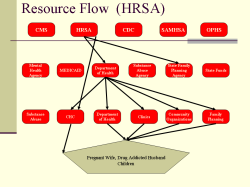
Resource Flow (HRSA)
PDF File or PPT File
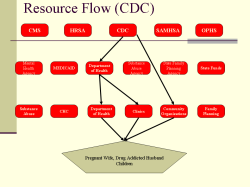
Slide 22
Resource Flow (CDC)
PDF File or PPT File
Slide 23
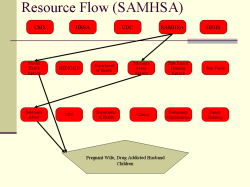
Resource Flow (SAMHSA)
PDF File or PPT File
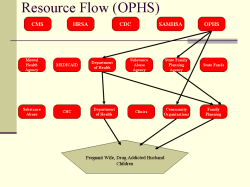
Slide 24
Resource Flow (OPHS)
PDF File or PPT File
Slide 25
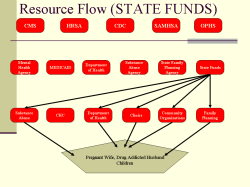
Resource Flow (STATE FUNDS)
PDF File or PPT File
Slide 26
Resource Flow (All Agencies)
PDF File or PPT File

Slide 27
The venue for making it happen everyday
PDF File or PPT File
Slide 28
One of my favorite books
PDF File or PPT File
Slide 29
Albert Einstein
PDF File or PPT File
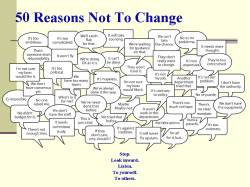
Slide 30
50 Reasons Not To Change
PDF File or PPT File
Slide 31
PUBLIC HEALTH IS LIFE BETTER
PDF File or PPT File
Slide 32
A "Glimpse" Into Local PH Practice
PDF File or PPT File

- Page last reviewed: March 5, 2014 (archived document)
- Content source: