

Slide Set E: Program Integration: The Virginia Experience
 ShareCompartir
ShareCompartir
This website is archived for historical purposes and is no longer being maintained or updated.
Download the complete slide set:
- 25 Slides in Adobe PDF Format - [56KB]
- 25 Slides in PowerPoint PPT Format - [76KB]
- 25 Slides in Adobe Flash Format - [116KB]

While the content is in the public domain and no copyright restriction applies, we do ask that users preserve the slides in their current format and cite CDC as the source.
Slide 1
Program Integration - The Virginia Experience
PDF File or PPT File
Slide 2
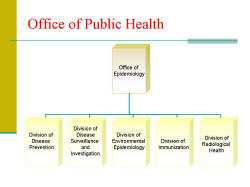
Office of Public Health
PDF File or PPT File
Slide 3
Programs Integrated & Rationale - AIDS Program
PDF File or PPT File
Slide 4
Programs Integrated & Rationale - Hepatitis Program
PDF File or PPT File
Slide 5
Programs Integrated & Rationale
PDF File or PPT File
Slide 6
Programs Integrated & Rationale
PDF File or PPT File
Slide 7
Programs Integrated & Rationale - The then Division of HIV/STD
PDF File or PPT File
Slide 8
Programs Integrated & Rationale - Pharmacy Services
PDF File or PPT File
Slide 9
Programs Integrated & Rationale
PDF File or PPT File
Slide 10
Programs Integrated & Rationale - TB Prevention and Control
PDF File or PPT File
Slide 11
Staff Perceptions to the Change - AIDS/HIV Program - New program, no merging of staff
PDF File or PPT File
Slide 12
Staff Perceptions to the Change - Hepatitis C Program - New program, no merging of staff
PDF File or PPT File
Slide 13
Staff Perceptions to the Change - Pharmacy Services - Involved staff merging
PDF File or PPT File
Slide 14
Staff Perceptions to the Change - TB Prevention and Control - Involved staff merging
PDF File or PPT File
Slide 15
Internal Barriers - AIDS Program - Pharmacy Services
PDF File or PPT File
Slide 16
Internal Barriers - TB Prevention and Control
PDF File or PPT File
Slide 17
Addressing Internal Barriers
PDF File or PPT File
Slide 18
Other Barriers
PDF File or PPT File
Slide 19
Wins - Client level
PDF File or PPT File
Slide 20
Wins - Health Department Level
PDF File or PPT File
Slide 21
Wins - Health Department Level
PDF File or PPT File
Slide 22
Embarking on Program Integration
PDF File or PPT File
Slide 23
Starting Process Again
PDF File or PPT File
Slide 24
Suggestions for CDC
PDF File or PPT File

- Page last reviewed: March 5, 2014 (archived document)
- Content source: